Download presentation
Presentation is loading. Please wait.

1
Javed Sethi

2
Which type of malarial plasmodium is the most common? What is the incubation period? Is the antimalarial prophylaxis on NHS prescriptions? Which antimalarial is safe in pregnancy?

3
Travelling 70 million trips in 2007 compared to 30 million in 1987 6% fall in visits abroad, but yet large numbers travel 1 in 10 seek medical advice

4
Epidemiology At risk areas include Africa, South America, Indian Subcontinent, Far East 1600 cases per year of malaria notified between 2003 to 2008 in travellers returning to UK Visiting family or friends > holiday makers 83% have not taken prophylaxis

5
Malaria Most common imported tropical disease 85 deaths from 2000 to 2008 Our role as GPs – in care of the acutely ill and in promoting health and preventing disease

7
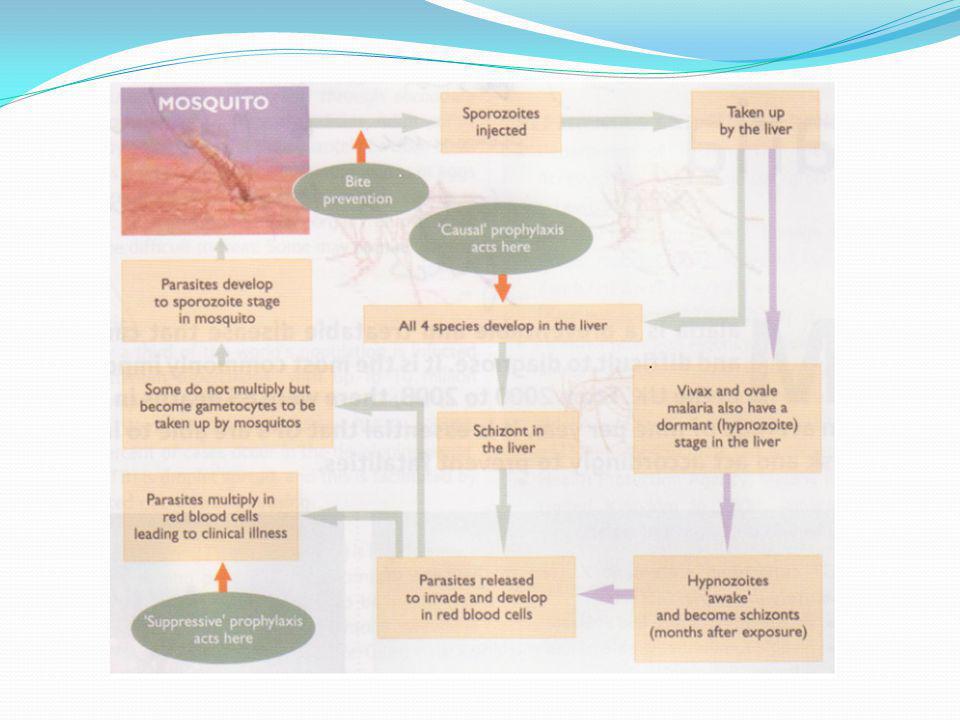
Malaria Plasmodium, by a mosquito bite- Anopheles Multiplies in liver and then attacks the RBCs Fever, nausea, shivering, headache and may result in multi-organ failure or even death Dormant in liver for months

9
Causes

10
Risk assessment Our responsibility under GMS Preventative measures – identify risks and those at risk Assessment with a questionnaire and face to face appointment Travel to visit family accounts 18% Destination, length of stay, accomodation, healthcare, budget and insurance Age, comorbidities, cultural beliefs

11
Post assessment advice General and specific advice Explain disease transmission Chemoprophylaxis Prevention advice Ensure understanding Sign post travellers to www.travax.nhs.uk, www.fitfortravel.nhs.ukwww.travax.nhs.uk

12
Clinical features Intermittent fever with rigors and sweating Headache, malaise, myalgia and anorexia Flu like symptoms Children can present with vague symptoms Incubation period is 6 days May manifest in 6 months or suspect for upto 12 months in travellers from high risk areas Complications occur with parasitaemia (> 2% blood cells parasitized)
")
13
Complications Impaired conciousness Seizures Renal impairment Acidosis Hypoglycaemia Pulmonary oedema DIC, Haemoglobinuria Shock

14
Investigations Discuss with microbiologist Thick and Thin blood films Repeat in 12 to 24 hours 3 negative films make diagnosis unlikely Malarial parasitic antigen FBC Notifiable disease Malaria reference laboratory Relatives/travelling group should be informed that they may be at risk

15
Treatment Falciparum malaria Uncomplicated: Quinine and doxycycline for 5 to 7 days Atovaqoune-proguanil for 3 days Complicated: IV quinine Mefloquine (side effects) Chloroquine (resistance)
 Chloroquine (resistance)")
16
Treatment Non falciparum malaria Chloroquine for 3 days then Primaquine for 14 days to treat hypnozoite stage

17
Prevention Risk of exposure versus side effects of chemoprophylaxis. Awareness of risk Prevention of Bites Chemoprophylaxis Diagnosis and treatment

18
Prevention of Bites Bite from dusk to dawn, peak at 02:00 am Repellants - Diethyltoluamide 50% Advisory Committee on Malaria Prevention recommend it in pregnancy, breast feeding, children Insecticides Mosquito nets Clothing, Electric heated devices

19
DrugAdvantagesDisadvantageDoseSide effects ProguanilWell toleratedResistance200 mg 1 wk before and 4 wks after GI upset ChloroquinePregnancy and breast feeding Exacerbate Myasthenia, Psoriasis 300mg wkly and 4 wks later GI upset and headache Mefloquine2 nd and third trimester, weekly dose CI in depression and epilepsy 250mg weekly begin 3 wks before til 4 wks Neuropsychiat ric problems DoxycyclineCheap, started close to departure Photosensitivi ty, CI in <12 100mg OD 2 days before and 4 wks later Oesophagitis, photosensitivi ty Atovaquone/ proguanil Short courseExpensive250/100mg, 2 days before til 7 days after GI upset and headache

20
Chemoprophylaxis Primaquine: Effective prophylactic against hynozoite stage Not recommended by ACMP Haemolysis in patients with G6PD deficiency

21
Prophylaxis Causal prophylaxis is against liver stage as it takes 7 days to develop To be taken for 7 days after Suppressive prophylaxis is against the red cell stage and is taken 4 weeks after Give travellers written information Not on NHS To buy over the counter or private prescription

22
Precautions in special conditions with antimalarials Pregnancy, Breastfeeding Epilepsy Anticoagulants G6PD deficiency Immunosuppression Sickle cell disease Liver disease, Renal impairment Porphyria

23
MYTH: I used to live in Africa so I am immune to Malaria FACT: Nobody is 100% immune and partial immunity fades

Similar presentations









 Symptoms and Diagnosis Treatment Preventive measures Where malaria occurs in the world.>")










