Download presentation
Presentation is loading. Please wait.

1
Tissue viability assessment tools Explore the purpose of assessment tools Review the meaning of validity and reliability with reference to a selection of assessment tools Explore the development of key wound/tissue viability assessment assessment tools Anne Ferguson Updated 30.4.13

2
What do we mean by assessment tools? Assessment is the first stage of the nursing process, tools enables us to gather information in order to plan care effectively making the best use of available resources. Tools that give us a score or have a measuring scale enable us to select interventions more precisely and evaluate the effectiveness of that intervention. By documenting our assessment in a standard format, it enables us to demonstrate a coordinated, consistent and comprehensive approach. Therefore assessment tools are designed for the purpose of:- Information gathering and monitoring Information gathering and prediction of risk/outcome

3
How are wound/skin assessment tools developed? What do you think the tool was designed for? Which patients was the tool meant to be used for? Has the tool been piloted prior to use? Who uses the tool? What literature was used as evidence when the tool was designed? Do the key components of the tool to demonstrate validity and reliability? Will the components of the tool measure what you want to measure? Are the components of the tool substantiated by research? Are terms used in the tool clearly explained? Are the terms used subjective or objective?

4
How effective are wound assessment tools (in other words, what do we mean by reliability and validity?) The two terms that need to be clarified in order to evaluate the utility of an assessment tools are reliability and validity. Validity means that the tool is measuring what it is intending to measure. –e.g a clock measures time, if it did not measure the true time it would be invalid Reliability simply means that the tool can be relied upon to give the same result on a single occasion despite the number of individuals who use it. The terminology is clear and does not allow for subjective interpretation. –e.g. a clock can be slow or fast making it unreliable. If, as a result of its unreliablity, it does not tell you the true time, then you can consider it to be invalid This means that if a tool is unreliable, then it cannot be valid as it can not be relied upon to give you a true measure of whatever it is that you are measuring

5
Assessment ‘data’ is a measurement, or measurements. For example: When you measure urine output, the amounts entered on the chart are data Definition: Data

6
Valid assessment data is evidence that is reliable and which is relevant to the question being investigated. Just being reliable evidence is not enough. The evidence has to be relevant as well For example… Validity

7
‘evidence’ is data which is judged to be relevant. For example: When you investigate dehydration, the urine output data is relevant, so it is evidence. The type of urine collection device is not relevant, so it is not evidence. Definition: Evidence

8
Definition: evidence

9
Discuss which of the following is valid evidence: Example 1 Measuring the length of a patient’s arm to decide their muscle strength? No, this is not valid evidence. A long arm can be strong or weak, and a short arm can be strong or weak Validity

10
Discuss which of the following is valid evidence: Example 2 Measuring the patient’s BMI to assess their nutritional status Yes, this is valid evidence as there is a recognised normal range of body weight to height. Having a low BMI can be indicator of inadequate nutritional input But..It is good but it is not the perfect evidence! Validity

11
Discuss if the following is valid evidence: Example 3 Measuring a patient’s ability to watch television as a measure of the degree of pain they are in? No, this is not valid evidence. A patient in pain will watch TV to distract their attention away from the pain, a patient who is not in pain will watch the TV to relax, because they are bored etc, depending on the mood they are in. Validity

12
Secondary evidence is data collected by someone else. You may find it in a book or on the internet. BUT You should always check to see if it is reliable and valid. For example… Validity

13
Example 1 Data on a pain assessment tool from a pharmaceutical company which produces analgesics. Would you trust this evidence, without further data? Validity: Secondary evidence

14
Example 2 Confirmation on the value of a tissue viability assessment tool, published by the person who designed it, but with either no supporting evidence or questionable evidence. Would you trust this evidence, without further data? Can you think of an assessment tool that is widely used in clinical practice, yet was developed with no supporting evidence? Validity

15
Validity: Types of Face validity: Does the tool look as if it will measure the concept (thing being measured) it was intended to measure? Content validity: Does it include all the components that adequately represent all characteristics of the concept (thing being measured). You would want experts to have complete agreements on components to be included. E.g. BAPEN brought together a panel of experts to agree on what should be included in the MUST, but which patients was it created for?
. You would want experts to have complete agreements on components to be included. E.g. BAPEN brought together a panel of experts to agree on what should be included in the MUST, but which patients was it created for .")
16
Validity: Types of Construct validity: How does it measure up to other things that you know should be in the tool, e.g. the BMI. There should be correlation between abnormal BMIs and poor nutritional status Internal Validity: The validity of the tool can change over time. E.g. patients expectations about pain may change during their stay in hospital External validity: mEWS has internal validity for critically ill patients in the acute setting but can you use the tool for other types of patients. i.e. would the mEWS work in the community with chronically ill patients?

17
If a tool has a scoring system how were the scores arrived at? At what point does a low score truly indicated there is no risk, for example, of malnutrition occurring or for a patient to be critically ill? At what point does a high score truly indicate the opposite, i.e. a patient is malnourished or a patient is critically ill? Validity: Scoring

18
Sensitivity: The tool accurately identifies those people at risk. If the tool incorrectly identifies people who are not at risk when they are, then the tool lacks sensitivity Specificity: The tool accurately identifies those people who are not at risk. If it incorrectly identifies people at risk when they are not, then the tool lacks specificity Validity: Sensitivity and specificity

19
In a group of 100 people, 60 are at risk of malnutrition, 40 are not. The ideal tool will give 60 positive results in those who are at risk and 40 negative results in those who are not. The tool would therefore have a sensitivity of 100% and a specificity of 100%. Most tools are not 100% accurate. If a tool gives a positive result in 48 out of the 60 who are at risk, what is the sensitivity? If the tool gives a negative result in 28/40 who are not at risk. What is the specificity? Validity: Sensitivity and specificity

20
It misses 12 out 60 who are at risk – they could go on to die as no referral would be made - FALSE NEGATIVES It lacks sensitivity It over identifies 12 as being at risk when they are not, referrals are made and extra treatment costs incurred that are a waste of resources – FALSE POSITIVES It lacks specificity Is it better to have false positives or false negatives? Validity: Sensitivity and specificity

21
Reliable data is evidence you can trust. Inter-rater reliability: If someone else assessed the same patient, using the same tool, at the same time, they would get the same result. If the information gathered is objective i.e. it can be measured or counted, it is more reliable than if the information is subjective, a personal impression that cannot be verified, For example, the wound is discharging +++ Is this subjective or objective? Reliability

22
Test-retest reliability: If the person using the assessment tool repeats the assessment, after a time interval, on the same patient and that patient’s condition has not altered, then the result should be the same. For example, if someone’s pain has not altered when you assess it again after 20 minutes, then the result should be the same. Reliability

25
ItemAssessmentDate Score Date Score Date Score 1. Size1 = Length x width <4 sq cm 2 = Length x width 4--<16 sq cm 3 = Length x width 16.1--<36 sq cm 4 = Length x width 36.1--<80 sq cm 5 = Length x width >80 sq cm 2. Depth1 = Non-blanchable erythema on intact skin 2 = Partial thickness skin loss involving epidermis &/or dermis 3 = Full thickness skin loss involving damage or necrosis of subcutaneous tissue; may extend down to but not through underlying fascia; &/or mixed partial & full thickness &/or tissue layers obscured by granulation tissue 4 = Obscured by necrosis 5 = Full thickness skin loss with extensive destruction, tissue necrosis or damage to muscle, bone or supporting structures 3. Edges1 = Indistinct, diffuse, none clearly visible 2 = Distinct, outline clearly visible, attached, even with wound base 3 = Well-defined, not attached to wound base 4 = Well-defined, not attached to base, rolled under, thickened 5 = Well-defined, fibrotic, scarred or hyperkeratotic 4. Under- mining 1 = None present 2 =Undermining < 2 cm in any area 3 = Undermining 2-4 cm involving < 50% wound margins 4 = Undermining 2-4 cm involving > 50% wound margins 5 = Undermining > 4 cm or Tunneling in any area BATES-JENSEN WOUND ASSESSMENT TOOL NAME Complete the rating sheet to assess wound status. Evaluate each item by picking the response that best describes the wound and entering the score in the item score column for the appropriate date. Location: Anatomic site. Circle, identify right (R) or left (L) and use "X" to mark site on body diagrams: ___________Sacrum & coccyx ___________Lateral ankle ___________ Trochanter ___________Medial ankle ___________Ischial tuberosity ___________Heel Other Site Shape: Overall wound pattern; assess by observing perimeter and depth. Circle and date appropriate description: __________Irregula___________Linear or elongated __________Round/oval ___________Bowl/boat __________Square/rectangle ___________Butterfly Other Shape
 or left (L) and use X to mark site on body diagrams: ___________Sacrum & coccyx ___________Lateral ankle ___________ Trochanter ___________Medial ankle ___________Ischial tuberosity ___________Heel Other Site Shape: Overall wound pattern; assess by observing perimeter and depth. Circle and date appropriate description: __________Irregula___________Linear or elongated __________Round/oval ___________Bowl/boat __________Square/rectangle ___________Butterfly Other Shape.")
26
5. Necrotic Tissue Type 1 = None visible 2 = White/grey non-viable tissue &/or non-adherent yellow slough 3 = Loosely adherent yellow slough 4 = Adherent, soft, black eschar 5 = Firmly adherent, hard, black eschar 6. Necrotic Tissue Amount 1 = None visible 2 = < 25% of wound bed covered 3 = 25% to 50% of wound covered 4 = > 50% and < 75% of wound covered 5 = 75% to 100% of wound covered 7. Exudate Type 1 = None 2 = Bloody 3 = Serosanguineous: thin, watery, pale red/pink 4 = Serous: thin, watery, clear 5 = Purulent: thin or thick, opaque, tan/yellow, with or without odor 8. Exudate Amount 1 = None, dry wound 2 = Scant, wound moist but no observable exudate 3 = Small 4 = Moderate 5 = Large 9. Skin Color Surrounding Wound 1 = Pink or normal for ethnic group 2 = Bright red &/or blanches to touch 3 = White or grey pallor or hypopigmented 4 = Dark red or purple &/or non-blanchable 5 = Black or hyperpigmented 10. Peripheral Tissue Edema 1 = No swelling or edema 2 = Non-pitting edema extends <4 cm around wound 3 = Non-pitting edema extends >4 cm around wound 4 = Pitting edema extends < 4 cm around wound 5 = Crepitus and/or pitting edema extends >4 cm around wound

27
Anne Ferguson Updated 30.4.13 12. Granu- lation Tissue 1 = Skin intact or partial thickness wound 2 = Bright, beefy red; 75% to 100% of wound filled &/or tissue overgrowth 3 = Bright, beefy red; 25% of wound filled 4 = Pink, &/or dull, dusky red &/or fills <25% of wound 5 = No granulation tissue present 13. Epithe- lializa- tion 1 = 100% wound covered, surface intact 2 = 75% to <100% wound covered &/or epithelial tissue extends >0.5cm into wound bed 3 = 50% to <75% wound covered &/or epithelial tissue extends to <0.5cm into wound bed 4 = 25% to < 50% wound covered 5 = < 25% wound covered TOTAL SCORE SIGNATURE 11. Peripheral Tissue Induration 1 = None present 2 = Induration, < 2 cm around wound 3 = Induration 2-4 cm extending < 50% around wound 4 = Induration 2-4 cm extending >50% around wound 5 = Induration > 4 cm in any area around wound

29
Percentage scoring for wound characteristic variables, according to ASEPSIS tool Wilson et al, 1986 Additional points were also scored for objective data related to: (Additional treatment) antibiotics (10 points); (Additional treatment)drainage of pus under local anaesthetic (5 points); (Additional treatment)debridement of wound under general anaesthetic (10 point); isolation of bacteria (10 points); and any stay in hospital > 14 days (5points)
 antibiotics (10 points); (Additional treatment)drainage of pus under local anaesthetic (5 points); (Additional treatment)debridement of wound under general anaesthetic (10 point); isolation of bacteria (10 points); and any stay in hospital > 14 days (5points)")
30
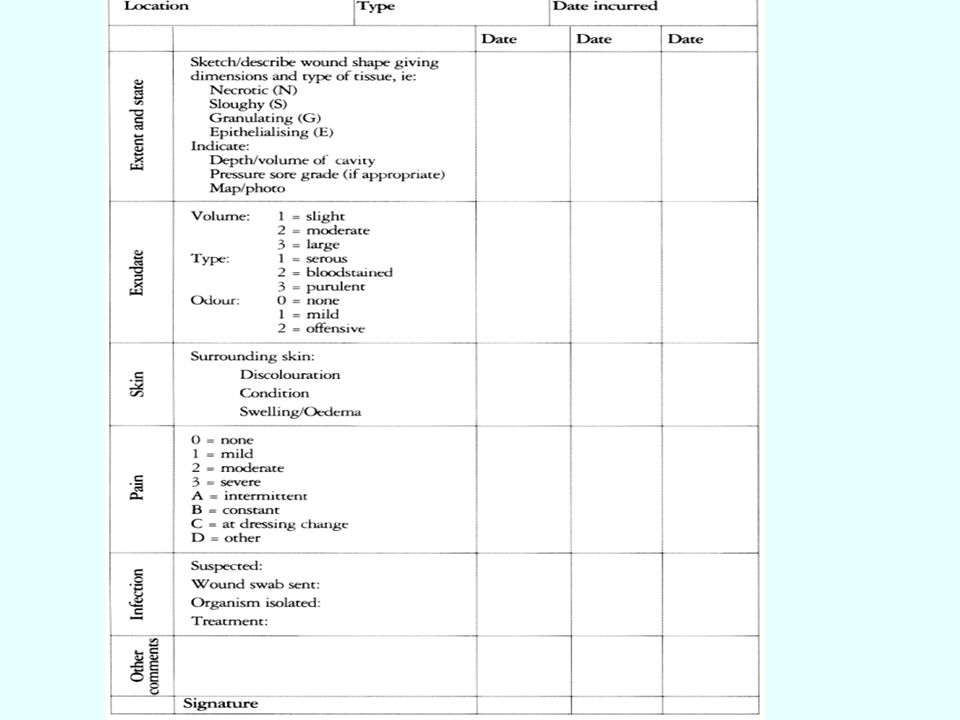
What is wrong with this assessment? What is wrong with this tool?

31
Put simply, reliability is the degree to which a tool measures the same way each time it is used in under the same conditions with the same subjects. Validity, is the degree to which a tool measures what you are supposed to, more simply, the accuracy of your measurement. Validity is more important than reliability because if a tool does not accurately measure what it is supposed to, there is no reason to use it even if it measures consistently (reliably), e.g. The inclusion of male/female in the Pressure risk assessment tool, easy and reliable to measure but WRONG indicator of risk Summary
, e.g. The inclusion of male/female in the Pressure risk assessment tool, easy and reliable to measure but WRONG indicator of risk Summary.")
Similar presentations