Download presentation
Presentation is loading. Please wait.

1
New England TB Case Series January 18, 2006
Ford von Reyn MD Dartmouth Medical School

2
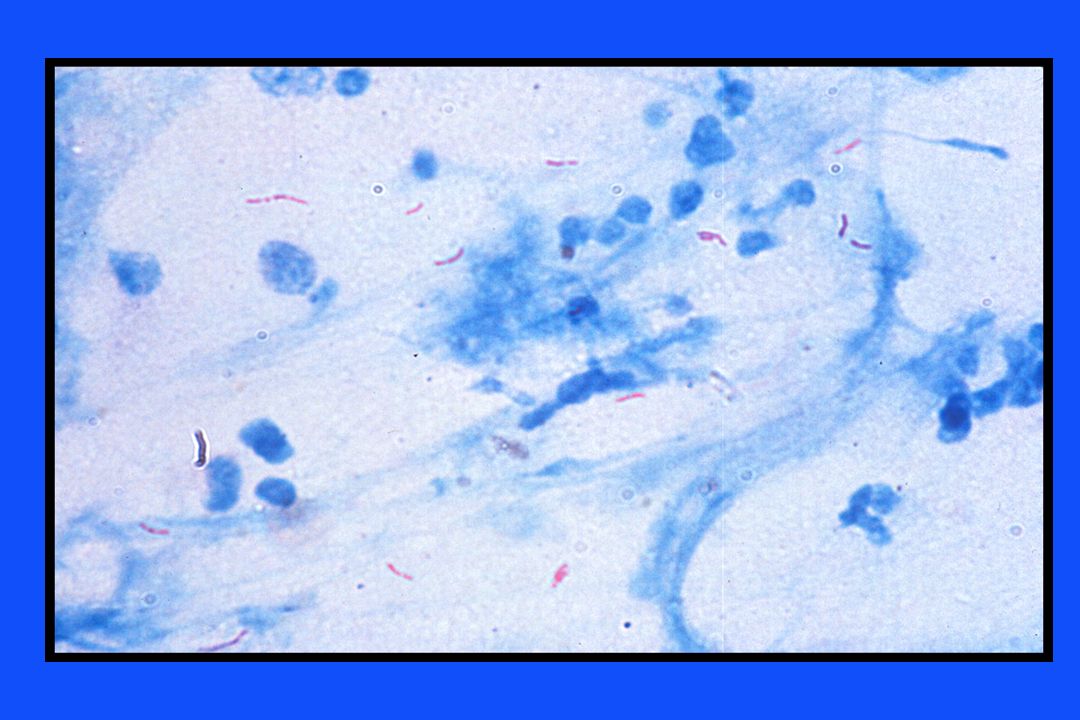
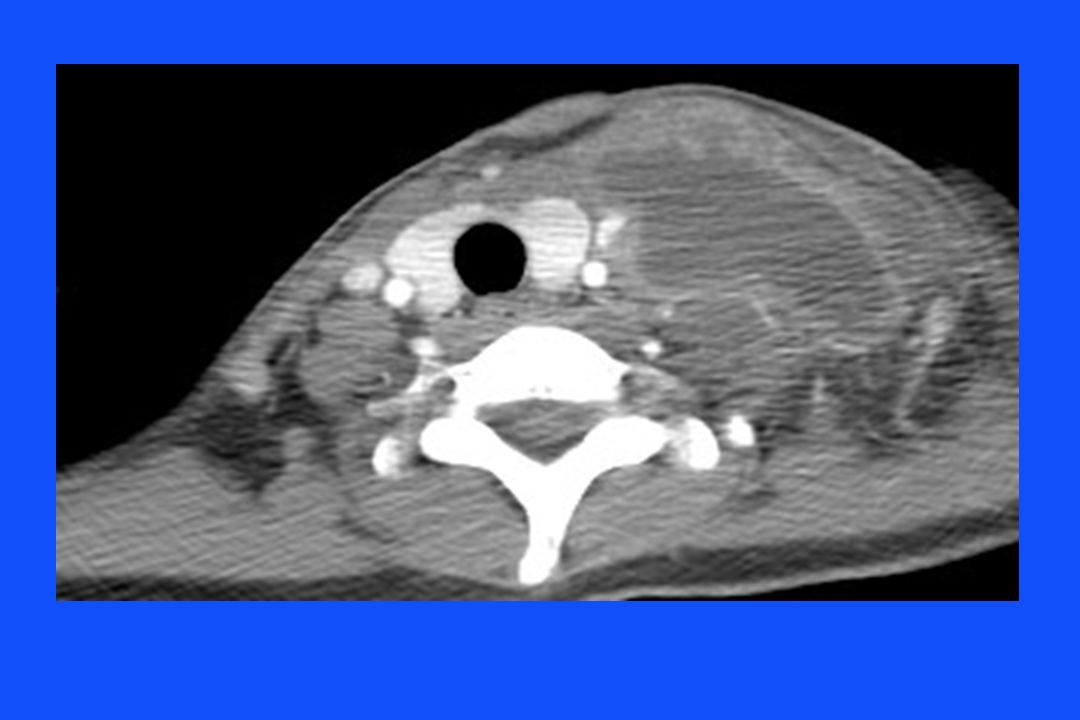
Case - 1 33 yo Thai woman working living in northern New Hampshire, unemployed February 2004: sore throat, followed by dysphagia, R neck swelling, 5 pound weight loss and fever March 10, 2004 (Boston): cervical node Bx under CT and US guidance showed AFB and necrotizing granulomatous inflammation, no Hx TB exposure, no PPD done Chest x-ray: next slide
: cervical node Bx under CT and US guidance showed AFB and necrotizing granulomatous inflammation, no Hx TB exposure, no PPD done. Chest x-ray: next slide.")
3
CXR from Dartmouth but probably the same at Mt A, shows deviation of trachea to left, no infiltrates

5
Questions Differential diagnosis? Isolation? Next steps?
NTM lymphadenitis, XX No isolation needed (except working with wound) Determine drug resistance in Thailand – 2% according to Palwatwichai, Apirak (2001) Tuberculosis in Thailand. Respirology 6 (1), doi: / j x
 Determine drug resistance in Thailand – 2% according to Palwatwichai, Apirak (2001) Tuberculosis in Thailand. Respirology 6 (1), doi: / j x.")
6
Differential Diagnosis
Mycobacterial adenitis: TB or non-tuberculous mycobacteria (NTM) Other bacterial: cat scratch, S. aureus or Streptococcal spp, tularemia Parasitic: Toxoplasmosis Viral Fungal Sarcoidosis Malignancy: lymphoma, sarcoma, carcinoma
 Other bacterial: cat scratch, S. aureus or Streptococcal spp, tularemia. Parasitic: Toxoplasmosis. Viral. Fungal. Sarcoidosis. Malignancy: lymphoma, sarcoma, carcinoma.")
7
MDR tuberculosis Defined as resistance to at least INH and rifampin
Website: o_htm_tb_2004_343/en/index.html Thailand: approximately 1-2% CDC suggests Rx for MDR TB if >4% (no data) NTM lymphadenitis, XX No isolation needed (except working with wound) Determine drug resistance in Thailand – 2% according to Palwatwichai, Apirak (2001) Tuberculosis in Thailand. Respirology 6 (1), doi: / j x
 NTM lymphadenitis, XX. No isolation needed (except working with wound) Determine drug resistance in Thailand – 2% according to Palwatwichai, Apirak (2001) Tuberculosis in Thailand. Respirology 6 (1), doi: / j x.")
8
Case - 2 March 17, 2004: Started on 4 drug Rx for TB
INH, Rifampin, Pyrazinamide, Ethambutol April 9, 2004: Positive culture for TB, later reported as sensitive to all first line drugs Rx once daily x 2 weeks, then twice weekly on Tues and Friday

9
Case - 3 April 19, 2004 (Dartmouth): Referred for evaluation of poorly responsive tuberculous lymphadenitis Hx: Neck still painful, no decrease in size No fever, last night sweats 2 weeks ago PE: Afebrile Weight 105 lb Lungs clear Tender L supraclavicular area 10 x 10 cm, woody induration, no fluctuance L arm weakness

10
April 2004 Scrofula

12
Questions What is the problem? Other studies? Therapy?
DDx is drug resistance, drug dosing, drug absorption, need for drainage. Or, just usual time course of TB adenitis? HIV negative

13
Case - 4 April 21: Admitted to Dartmouth- Hitchcock Medical Center for further increase in size of neck mass Daily Rx, PZA reduced from 2.0 to 1.2 gm because of nausea April 23: Neck aspirate AFB positive Next steps?

14
Case - 5 April 28, 2004: Prednisone 80 mg/d
May 4, 2004: Neck still painful and mass enlarging I & D at 3 sites by ENT: brown pus, clots, AFB pos May 11, 2004: Prednisone D/Ced, fever and muscle pain developed Prednisone 20 mg/d resumed, fever cleared May 14, 2004: Discharged home on 2x weekly Rx

15
Case - 6 May 27, 2004: OPD visit. No fevers, still some leg pain, wounds packed daily, less neck pain, 11 lb weight gain June 25, 2004: L leg swelling, neg US, clinical suspicion of DVT, Rx ASA July 27, 2005: Cont’d decrease in neck swelling, weight up 20 lbs, continue prednisone 20 mg Completed 8 mos total Rx in December 2004

16
Scrofula Scrofula = mycobacterial lymphadenitis
King’s Evil: Medieval term, “cured” by touch of the king Historical: common in Europe in 19th century (24% of children had evidence of current or past infection) Latin for swelling of glands (diminuitive of sow).
 Latin for swelling of glands (diminuitive of sow).")
17
Copperplate engraving by André Du Laurens ( ), an anatomist and Paris court physician, showing King Henry IV of France touching a number of sufferers who are gathered about him in a circle. Legend of the original plate: Des mirabili strumas sanandi vi solis Galliae regibus christianissimis divinitus concessa liber unus. Paris: Apud Marcum Orry, 1609

18
Scrofula Etiology M. tuberculosis (MTB) M. bovis (MB)
Non-tuberculous mycobacteria (NTM) Developing countries: MTB> MB>>>NTM Developed countries: NTM>>MTB>MB MTB all human. MB from cow’s milk. Bovis was the classic cause before widespread pasteruization of milk
 Developing countries: MTB> MB>>>NTM. Developed countries: NTM>>MTB>MB. MTB all human. MB from cow’s milk. Bovis was the classic cause before widespread pasteruization of milk.")
19
Lymphadenitis due to MTB
Age most common, F: M ratio is 2:1 Ethnic: esp Asian (80%), Indian; also African, Af-Am, Hispanic, Native American 3-5% of US TB cases Clinical settings Primary TB (children) Reactivation TB (adults) HIV IRIS (HIV) Previously predominantly a disease of children (still true in endemic countries). Males dominate in pulmonary TB, females in scrofula. As many as 40% of AIDS pts with TB have lymphadenitis. Immunologic immaturity seems to be a common theme.
, Indian; also African, Af-Am, Hispanic, Native American. 3-5% of US TB cases. Clinical settings. Primary TB (children) Reactivation TB (adults) HIV. IRIS (HIV) Previously predominantly a disease of children (still true in endemic countries). Males dominate in pulmonary TB, females in scrofula. As many as 40% of AIDS pts with TB have lymphadenitis. Immunologic immaturity seems to be a common theme.")
20
Lymphadenitis due to MTB
Nodes: usu multiple nodes, jugular, posterior triangle, supraclavicular Pathophysiology: systemic dissemination Symptoms: weeks to months, fever, wt loss, fatigue, nt sweats in 20-50% Chest x-ray: 30% have findings Tuberculin skin test: 70-90% positive Does MB pathophys differ? Wide variation in reports of abnl CXR prob depends on pathophys.

21
Subclinical TB in HIV: Tanzania
HIV positive ambulatory patients with CD4>200 screened for a TB vaccine trial in Tanzania Among first 93 patients 14 (15%) met clinical criteria for active tuberculosis “Subclinical TB”: 10 patients with no signs, symptoms or x-ray abnormalities but positive sputum cultures (DNA typing showed not contaminants); 3/10 pos AFB smears, 60% adenopathy Implications Need for better diagnostics Inappropriate INH for latent TB that is really early active TB -Mtei, von Reyn 2003
 met clinical criteria for active tuberculosis. Subclinical TB : 10 patients with no signs, symptoms or x-ray abnormalities but positive sputum cultures (DNA typing showed not contaminants); 3/10 pos AFB smears, 60% adenopathy. Implications. Need for better diagnostics. Inappropriate INH for latent TB that is really early active TB. -Mtei, von Reyn")
23
Immune reconstitution syndrome (IRIS) in HIV/TB
• Fever, lymphadenitis, +/- pulmonary infiltrate, expansion of CNS lesions, in HIV pos patients on Rx for TB who are then started on HAART and experience immune reconstitution Also called “paradoxical reactions” Occurred in 6 (35%) patients started on HAART (for HIV) while on TB therapy • All occurred with HAART start <2 mos after TB Rx start (median 22 days), 5/6 had initial CD4<100, more likely if >2 log drop in HIV viral load Smears pos in 4/6, culture pos in 2/6 Management: distinguish treatment failure, continue TB Rx, NSIADs for mild Sx, steroids for severe Sx Most cases resolve within a few weeks -Navas, 2002 Flare of clinical symptoms that had previous improved after initiation of TB Rx. Study done in Madrid. Other feature can be swelling of CNS lesions,
 patients started on HAART (for HIV) while on TB therapy. • All occurred with HAART start <2 mos after TB Rx start (median 22 days), 5/6 had initial CD4<100, more likely if >2 log drop in HIV viral load. Smears pos in 4/6, culture pos in 2/6. Management: distinguish treatment failure, continue TB Rx, NSIADs for mild Sx, steroids for severe Sx. Most cases resolve within a few weeks. -Navas, Flare of clinical symptoms that had previous improved after initiation of TB Rx. Study done in Madrid. Other feature can be swelling of CNS lesions,")
24
Lymphadenitis due to MTB - Dx
Fine needle aspiration (FNA) for cytology and AFB smear sensitivity 80% specificity 90% Excisional Bx: second choice for Dx because of possibility for fistula, sinus tracts Culture: positive in 35% Culture pos highest if necrosis.
 for cytology and AFB smear sensitivity 80% specificity 90% Excisional Bx: second choice for Dx because of possibility for fistula, sinus tracts. Culture: positive in 35% Culture pos highest if necrosis.")
25
Lymphadenitis due to MTB - Rx
Standard 4 drug chemotherapy Slow response: common for enlargement of nodes or new nodes on Rx, cultures usu negative Surgical drainage: for painful lesions or very slow response on chemoRx Culture pos highest if necrosis. Neg cultures suggest that the 15% or so who seem to progress prob have immunologic basis.

26
Lymphadenitis due to NTM
Clinical: indolent lymphadenitis in healthy children age 1-5 usu due to M. avium complex Nodes: upper cervical, salivary area nodes Risk factors: unknown (?soil/water exposure with erupting teeth), BCG protects (Sweden, Finland) Rx: surgical excision; two drug Rx (from macrolide, ethambutol, rifamycin) may benefit those who are not surgical candidates Incidence: rising in the United States, increased in Sweden with decreased BCG use MAC cervical adenitis in healthy children occurs during the same age that Ab studies show many children are first encountering the organism. This occurs from age 1-5 when children have started to walk, are cutting teeth and live in close proximity to water and soil.
, BCG protects (Sweden, Finland) Rx: surgical excision; two drug Rx (from macrolide, ethambutol, rifamycin) may benefit those who are not surgical candidates. Incidence: rising in the United States, increased in Sweden with decreased BCG use. MAC cervical adenitis in healthy children occurs during the same age that Ab studies show many children are first encountering the organism. This occurs from age 1-5 when children have started to walk, are cutting teeth and live in close proximity to water and soil.")
28
Childhood adenitis: Cleveland, US
These are data frmo Dr. Wolinsky on cases of MAC cervical adenitis by 3 year interval among children in Cleveland. There was clearly a sharp increase around 1980 as disease due to scrofulacem was falling. Although the incidence of TB was falling progressively at the same time and might mean there was less cross protective immunity this would not explain the rather sudden increase in 1980. [wolinsky: 2x more common for onset in winter or spring than summer or fall] [Pang: western Australia: MAC 74%, scrof 20, TB 4%] [Trnka, Czech: 4/100,000 children MAC adenitis, higher in those without BCG] [Kuth, Aachen, Germany: increse starting in 1990] [John Grange: in crease in south east England starting 1980] -Wolinsky. Clin Infect Dis 1995;20:

29
Summary - Scrofula Case presentation: slowly resolving drug sensitive MTB lymphadenitis in a Thai woman, Rx required 8 mos chemo and surgical drainage Usu demographics: F>M, esp Asian, age 20-30 Other clinical settings: HIV, IRIS, primary infection Most adult cases in US due to MTB, childhood cases due to NTM Rx for childhood NTM is usually surgery

Similar presentations







 Bob Colebunders.>")

 Lawrence Pike.>")




 is an infectious disease caused by the bacterium: “Mycobacterium tuberculosis”>")
 in Children>")





