Download presentation
Presentation is loading. Please wait.

1
Treatments in Parkinson’s disease

2
Treatment in PD Complex because of Progressive nature of disease
Motor and non-motor features Early and late side effects associated with the treatments

3
Available Interventions

4
Goals of treatment in PD
Prevention of disease progression Symptomatic treatment of motor symptoms Management of motor complications Wearing off/motor fluctuations Dyskinesias Symptomatic treatment of non-motor symptoms

5
Prevention of disease progression
“Neuroprotection is an unmet need in Parkinson’s disease and no drug can be recommended yet for this purpose in practice.”

6
Motor symptoms Symptoms that are being targeted by medications Tremor
Rigidity Bradykinesia Gait/postural instability

7
Motor complications What are motor fluctuations/off time?
Periods of alteration of symptom control On/off time – initially predictable, later unpredictable What are dyskinesias? Drug-induced involuntary movements that include chorea and dystonia Risk factors for development Younger age at onset of PD, severity, higher L-dopa dose and longer disease duration

8
Overview of topics Levodopa Entocapone Dopamine agonists
MAOB inhibitors Amantadine Anticholinergics Deep brain stimulation Treatment of non-motor symptoms

9
Question The mechanism of the antiparkinsonian effect of rasagiline and selegiline is inhibition of: A. aromatic amino acid decarboxylase B. catechol-O-methyltransferase C. monoamine oxidase type A D. monoamine oxidase type B E. tyrosine hydroxylase

10
Question True or false? There is good evidence to support the use of MAOB inhibitors as adjuncts to DA-agonists. MAOB inhibitors effectively reduce dyskinesias in patients with PD.

11
MAO INHIBITORS

12
Monoamine Oxidase (MAO)
Group of enzymes involved in monoamine metabolism Dopamine, serotonin, norepinephrine Two enzyme subtypes Type A and type B In brain Both A+B In GI tract mostly A

13
Substrates of MAOs

14
MAO Inhibitors (MAOI) Serendipitously discovered group of drugs with anti-depressant effect Despite effectiveness, second-line drug “Cheese reaction” Extensive side effect profile

15
What is the Cheese Reaction?
Hypertensive crisis in patients on MAOIs who ingest tyramine Tyramine is a monoamine present in aged cheeses, red wine, sausages Usu. metabolised by MAO-A Gut, portal circulation, peripheral neurons With MAOI (non-selective or selective for A) Tyramine stimulates peripheral adrenergic neurons Hypertensive crisis The cheese reaction is the consequence of inhibition of MAO-A, an enzyme predominantly present in the gut, portal system, and peripheral and central adrenergic neurons, by at least 80%
 Tyramine stimulates peripheral adrenergic neurons. Hypertensive crisis. The cheese reaction is the consequence of inhibition of MAO-A, an enzyme predominantly present in the gut, portal system, and peripheral and central adrenergic neurons, by at least 80%")
16
Why use MAOIs in PD? MAO is present in brain, including the BG
Type B (80%) >> A If use selective MAO-B inhibitor: Will inhibit dopamine metabolism in the BG (80% type B) Avoid cheese reaction (dependent on MAO-A) Avoid extensive side effect profile Selective MAO-B inhibitors Selegiline and rasagiline Note: almost no MAO activity in neurons of the SN
 >> A. If use selective MAO-B inhibitor: Will inhibit dopamine metabolism in the BG (80% type B) Avoid cheese reaction (dependent on MAO-A) Avoid extensive side effect profile. Selective MAO-B inhibitors. Selegiline and rasagiline. Note: almost no MAO activity in neurons of the SN.")
17
Selegiline - Use What is the role of selegiline in the treatment of PD for relief of motor symptoms? AAN Practice Parameters (2002): Can be used initially as monotherapy for mild symptomatic relief Movement Disorder Society (2002) Effective as monotherapy Insufficient data to recommend use as as adjunct in patients already on DA-ergic agents
: Can be used initially as monotherapy for mild symptomatic relief. Movement Disorder Society (2002) Effective as monotherapy. Insufficient data to recommend use as as adjunct in patients already on DA-ergic agents.")
18
Selegiline - Use What about its role in motor complications?
Insufficient data for fluctuations Non-efficacious in preventing dyskinesias What about its role in neuroprotection? Insufficient evidence to suggest that it has a neuroprotective effect (despite initial studies) Doses Start at 5mg daily Increase to 5mg bid (maximum dose) Neuroprotection was initially thought to be the case, because in comparison to placebo, patients on selegiline had improved UPDRS scores and slower disease progression. However, this was later determined that these were likely be due to symptomatic relief and not neuroproteciton The trials were done in patients who were early onset PD and were compared to placebo. Neuroprotection was suspected because there was a delay to initiation of L-dopa.
 Doses. Start at 5mg daily. Increase to 5mg bid (maximum dose) Neuroprotection was initially thought to be the case, because in comparison to placebo, patients on selegiline had improved UPDRS scores and slower disease progression. However, this was later determined that these were likely be due to symptomatic relief and not neuroproteciton. The trials were done in patients who were early onset PD and were compared to placebo. Neuroprotection was suspected because there was a delay to initiation of L-dopa.")
19
Selegiline – Side effects
Mortality One study showed excess mortality in selegiline group Meta-analysis did not confirm this Headache, nausea, insomnia Confusion in the elderly Can enhance side effects of L-dopa (But no evidence to use together) Be careful with cold remedies that contain pseudoephedrine or phenylephrine
 Be careful with cold remedies that contain pseudoephedrine or phenylephrine.")
20
Rasagiline (Azilect) What is the role for rasagiline in mgmnt of motor symptoms? Movement Disorder Society (2005) Effective as monotherapy Insufficient data to recommend use as adjunct in patients already on DA-ergic agents Insufficient data regarding role in motor complications (MDS)
")
21
Rasagiline (Azilect) Doses Side effects Start at 0.5mg daily
Increase to 1mg daily (maximum dose) Side effects Same as selegiline More potent than selegiline and irreversible action
 Side effects. Same as selegiline. More potent than selegiline and irreversible action.")
22
other

23
Question In which group of PD patients would you consider using anticholinergics? A. Younger patients with predominant rigidity B. Younger patients with predominant tremor C. Elderly patients with predominant motor fluctuations D. Elderly patients with predominant non-motor symptoms

24
Anticholinergics Mechanism of Action in PD Not clearly known
Degeneration of DA-ergic nigrostriatal neurons imbalance between striatal dopamine and Ach Anticholinergics help counteract the imbalance ounteracting the imbalance between striatal dopamine and acetylcholine activities caused by the degeneration of dopaminergic nigrostriatal neurons in Parkinson´s disease

25
Anticholinergics - Use
What is the role for anticholinergics in the management of PD? 1993 AAN Practice parameters Can be considered as initial therapy esp. if tremor predominant MDS (2002) Likely efficacious as monotherapy in early PD and as adjunct in patients on L-dopa Insufficient data re: efficacy for prevention/treatment of motor fluctuations Typically: young patients with predominant tremor
 Likely efficacious as monotherapy in early PD and as adjunct in patients on L-dopa. Insufficient data re: efficacy for prevention/treatment of motor fluctuations. Typically: young patients with predominant tremor.")
26
Anticholinergics – Side effects
Main ones (start low, go slow): Trihexyphenidyl (Artane) Start 0.5-1mg bid, increase to 2mg tid Benztropine (Cogentin) Start mg bid, increase to 2 bid Side effects Confusion, hallucinations, blurry vision, increased intraocular pressure, dry mouth, urinary retention, constipation
: Trihexyphenidyl (Artane) Start 0.5-1mg bid, increase to 2mg tid. Benztropine (Cogentin) Start mg bid, increase to 2 bid. Side effects. Confusion, hallucinations, blurry vision, increased intraocular pressure, dry mouth, urinary retention, constipation.")
27
Amantadine Used in PD for over 40 years
Antiparkinsonian MoA not fully known Partial NMDA receptor antagonist Partial dopamine agonist

28
Amantadine - Use What is the role for amantadine in the treatment of motor symptoms? Safe and modestly effective (AAN) “Likely efficacious” as monotherapy in early PD (MDS) What about its role in motor complications? “Possibly efficacious” at reducing dyskinesias May be considered for pts with motor fluctuations Efficacious in pts on L-Dopa with motor complications
 What about its role in motor complications Possibly efficacious at reducing dyskinesias. May be considered for pts with motor fluctuations. Efficacious in pts on L-Dopa with motor complications.")
29
Amantadine - Use Role in motor complications ctn’d Dose Side effects
Effect on dyskinesias likely better than more frequent dosing of L-Dopa Unknown efficacy in comparison to DA-agonist (pramipexole, ropinirole) Dose 100 mg po daily to qid Side effects Livedo reticularis, leg edema, Same side effect profile as dopamine agonists Generally well-tolerated
 Dose. 100 mg po daily to qid. Side effects. Livedo reticularis, leg edema, Same side effect profile as dopamine agonists. Generally well-tolerated.")
30
Non-motor symptoms

31
A 78-year-old woman with a 15-year history of PD has developed visual hallucinations. Her medications include carbidopa/levodopa, ropinirole, and rasagiline. Her hallucinations have not diminished significantly with trials of reductions of each of her medications. Which of the following medications is most appropriate for this patient? A. chlorpromazine B. haloperidol C. quetiapine D. thioridazine E. thiothixene

32
Non-motor symptoms “Non-motor symptoms dominate the clinical picture of advanced Parkinson’s disease and contribute to severe disability, impaired quality of life, and shortened life expectancy”

33
Pathophysiology Non-dopaminergic-cell dysfunction thought to play a major part in the development of the non-motor symptoms However, neuroanatomy and neurochemistry of non-motor symptoms are unknown

35
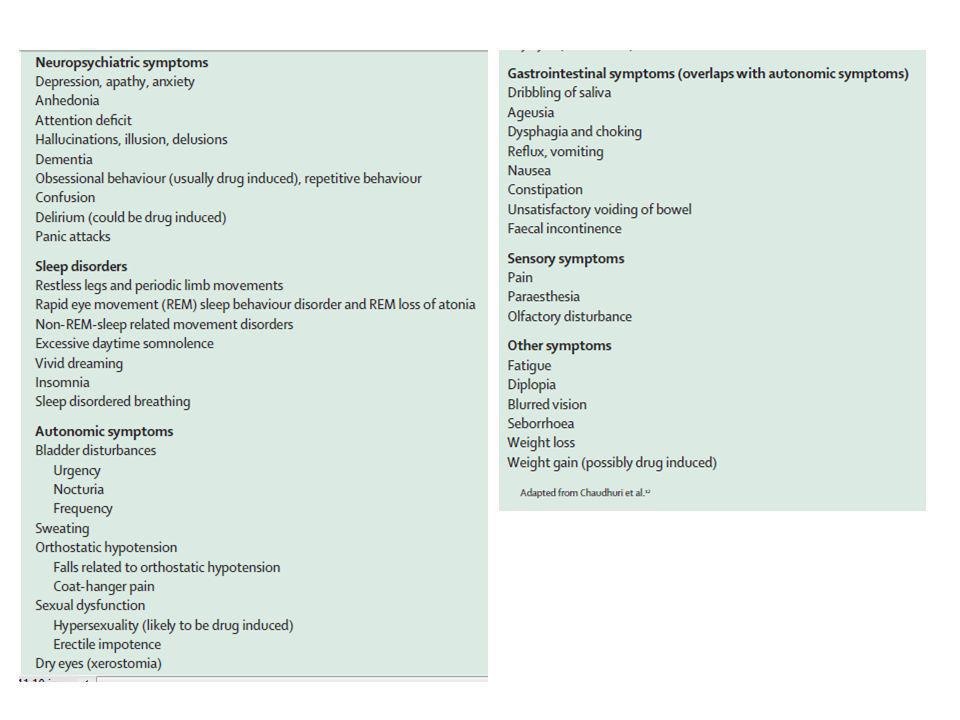
Non-motor symptoms Neuropsychiatric symptoms Sleep disorders
Depression, apathy, anxiety, hallucinations, dementia, impulsive behavior (usu drug-induced) Sleep disorders Restless legs and period limb movements, REM-sleep behavior disorder, excessive daytime somnolence Autonomic symptoms Bladder (urgency, nocturia, frequency), sweating, orthostatic hypotension, sexual dysfunction GI symptoms (overlap with dysautonomia) Dribbling saliva, constipation, dysphagia, ageusia, Sensory symptoms Olfactory disturbance, pain, paresthesias
 Sleep disorders. Restless legs and period limb movements, REM-sleep behavior disorder, excessive daytime somnolence. Autonomic symptoms. Bladder (urgency, nocturia, frequency), sweating, orthostatic hypotension, sexual dysfunction. GI symptoms (overlap with dysautonomia) Dribbling saliva, constipation, dysphagia, ageusia, Sensory symptoms. Olfactory disturbance, pain, paresthesias.")
36
Management Depression Anxiety Psychosis Orthostatic hypotension
Dementia Sexual dysfunction Sleep dysfunction

37
Management - Depression
Can affect from 10-45% of patients Likely has a biological contribution May be a result of impaired 5HT transmission What is best pharmacological treatment? (AAN 2006) The highest level of evidence is for amitriptyline Although it may be considered, it is not necessarily the first choice for treatment of depression associated with PD. Insufficient evidence to make recommendations regarding other treatments for depression SSRIs and SNRIs are used but little published data in PD amitriptyline, nortriptyline, citalopram, fluoxetine, sertraline, pergolide, pramipexole, and nefazodone
 The highest level of evidence is for amitriptyline. Although it may be considered, it is not necessarily the first choice for treatment of depression associated with PD. Insufficient evidence to make recommendations regarding other treatments for depression. SSRIs and SNRIs are used but little published data in PD. amitriptyline, nortriptyline, citalopram, fluoxetine, sertraline, pergolide, pramipexole, and nefazodone.")
38
Management – Anxiety and Apathy
Anxiety disorder common Often coexists with depression Panic attacks, phobias, GAD, related to motor fluctuations AAN practice parameters regarding treatment Insufficient evidence to make any recommendations

39
Management - Psychosis
What is the best treatment for patients with PD and psychosis? Clozapine should be considered Remember: associated with agranulocytosis that may be fatal. The absolute neutrophil count must be monitored. Quetiapine may be considered Olanzapine should not be routinely considered No proven efficacy and may worsen motor function Note that not FDA approved because of increased risk of death in pts with dementia Side effects are worsening of motor function, weight gain, insulin resistance and diabetes

40
Management - Dementia What are the most accurate screening tools in PD? MMSE and CAMCog (Cambridge cognitive assessment) MMSE as sensitive but not as specific What is the most effective treatment for dementia in PD? Rivastigmine probably effective in improving cognitive function. Modest effect and may exacerbate tremor Donepezil is probably effective in improving cognitive function. Modest effect. Donepezil – non-competitive ACHesterase inhibitor One study – measured at 20 weeks, MMSE, improved by 2 points

41
Management – Orthostatic Hypotension
Defined as a 20mmHg drop in systolic BP or a 10mmHg drop in diastolic BP Challenge in PD DA-ergic agents often worsen OH Reducing dose usually insufficient to treat What treatments are effective? (AAN 2006) Insufficient data to recommend to any particular treatment Symptoms variable – can be disabling Lightheadedness, syncope, fatigue, cognitive slowing, neck tightness, headache, unsteadiness
 Insufficient data to recommend to any particular treatment. Symptoms variable – can be disabling. Lightheadedness, syncope, fatigue, cognitive slowing, neck tightness, headache, unsteadiness.")
42
Management – Orthostatic Hypotension
Compression stockings Increasing water intake Fludrocortisone Dose: 0.1 – 0.3mg daily + high Na intake Supine hypertension, peripheral edema Midodrine Peripheral alpha1 receptor agonist Dose: 2.5 to 5mg tid Others: domperidone, pyridostigmine, indomethacin Domperidone – peripheral DA antagonist therefore blocks peripheral effects of DA

43
Management – Sexual Dysfunction
Common in both men and women Multifactorial Motor dysfunction, medication side effects, mood disorders, and dysautonomia Dysautonomia erectile dysfunction One study looked at sildenafil in ED 12 patients with PD, BP > 90/50 Sildenafil at 50mg significantly improved ED

44
Management – Sexual Dysfunction
AAN Practice Parameter Sildenafil possibly efficacious Need to ensure that other treatable causes of ED/sexual dysfctn have also been addressed Note: hypersexuality can be seen in PD associated with DA-ergic agents

45
A 48-year-old man with a 1-year history of PD comes to the office with his wife. She states that for the past 5 years he’s had episodes of kicking and punching during sleep. This has resulted in injuries to both. He is currently taking no medications. What is the diagnosis? Which of the following is most likely to benefit this patient’s nocturnal symptoms? A. amantadine B. clonazepam C. pramipexole D. ropinirole E. selegiline

46
Management – Sleep Dysfunction
Range of sleep dysfunction REM sleep behavior disorder (RBD) Excessive daytime somnolence (EDS) Insomnia Restless legs syndrome and periodic limb movement
 Excessive daytime somnolence (EDS) Insomnia. Restless legs syndrome and periodic limb movement.")
47
Management – RBD A type of parasomnia characterized by patients acting out dramatic or violent dreams during the REM sleep stage. What treatments are effective in PD? Insufficient data What treatments are available for RBD? Clonazepam to 1mg po qhs Melatonin

48
Question

49
Management - EDS May be 2ary to disease process or medication side effect Dopaminergic agents can cause mild to severe somnolence Falling asleep at wheel of car Agonists > L-dopa FDA warnings for pramipexole and ropinirole Patients should be advised to d/c DA agonists if marked increase in sleepiness

50
Management - EDS What treatments are available?
Modafinil improves SUBJECTIVE feeling of sleepiness but doesn’t change OBJECTIVE measurements of somnolence Dose: 200mg daily in am

51
Management - Insomnia Etiology is multifactorial
Mood disturbances, persistent tremor, nighttime PD symptoms, nocturia, and reversal of sleep patterns Practice parameter: Insufficient data Available treatments Bedtime L-dopa – may improve nocturnal PD sx Melatonin – Improves perception Sedating antidepressants (trazodone) Mild sedatives – zopiclone, zolpidem Over-the-counter sleeping aids – beware of side effects (anticholinergic effect)
 Mild sedatives – zopiclone, zolpidem. Over-the-counter sleeping aids – beware of side effects (anticholinergic effect)")
52
Management - RLS Occurs in up to 20% of patients
No evidence on how to treat of RLS in PD May use ropinirole and pramipexole FDA approved treatment in primary RLS

54
Summary MAOB Inhibitors Anticholinergics Amantadine
Monotherapy, early PD Not for motor complications or neuroprotection Anticholinergics Young patients with predominant tremor Not for motor complications Amantadine Monotherapy for motor symptoms Adjunct if L-dopa induced motor complications

55
Summary Depression Psychosis Dementia Orthostatic hypotension
Consider amitryptilline Psychosis Clozapine > quetiapine Dementia Rivastigmine and donepezil Orthostatic hypotension Non-pharm; fludro, midodrine, domperidone

56
Summary RBD EDS RLS Clonazepam Warn patients! Remove offending agent
Pramipexole and ropinirole

57
Cases

58
Case 1 44 y.o. woman. New left hand tremor and shoulder stiffness. Not yet interfering with work. On exam – left sided rigidity, bradykinesia and tremor Assuming that your best diagnosis is IPD: Should you start the patient on treatment? What treatment would you start? What are the benefits/disadvantages of the different options?

59
Case 1 Should you start the patient on treatment?
No evidence that starting treatment early is harmful or worsens long-term outcome Therefore, generally decision to start treatment should take into account degree of symptoms/disability versus adverse effects of medication

60
Case 1 What treatment would you start? What are the benefits/disadvantages of the different options? Levodopa –less sleepiness and psych Ses, but higher rate of dyskinesias Dopamine agonists – longer duration of action, less dyskinesias, but greater sleepiness and psychiatric SEs MAOB inhibitors Anticholinergics Amantadine

61
Case 2 65 y.o. man, PD x 5 yrs On Sinemet 100/25 qid and selegiline 5 bid For 1 yr: am off time before meds kick in and pm dyskinesias How can you decrease morning off time? How can you decrease dyskinesias?

62
Case 2 How can you decrease morning off time?
Adding a COMT inhibitor however, can increase dyskinesias Adding pramipexole or ropinirole may increase dyskinesias Adding amantadine (less evidence for motor fluctuations) How can you decrease dyskinesias? Adding DA- agonist and reducing L-Dopa dose slowly Adding Amantadine
 How can you decrease dyskinesias Adding DA- agonist and reducing L-Dopa dose slowly. Adding Amantadine.")
63
Case 3 73 y.o. woman, PD x 10 years On Sinemet and pramipexole
Mild dyskinesias and motor fluctuation Recent forgetfulness and apparent visual hallucinations. On exam, MMSE 27/30 and mild choreatic dyskinesias

64
Case 3 What single intervention is most likely to reduce hallucinations? If that fails to control hallucinations, what is the next step? Would you treat her mild cognitive impairment?

65
Case 3 What single intervention is most likely to reduce hallucinations? Remove the pramipexole This may lead to increased motor fluctuations and dyskinesias and require Sinemet dose adjustment If that fails to control hallucinations, what is the next step? Atypical antipsychotics: clozapine, quetiapine

66
Thank you

69
Review Question A 51 y.o. woman developed PD and was started on treatment. Soon after, she began to spend money on frivolous items and went to the casino where she lost her life savings. What is the diagnosis? It is a side effect of which class of medication? MAOB inhibitors Dopamine agonists Anticholinergics COMT inhibitors

70
Review Question Which of the following agents can be used as monotherapy in PD (choose as many as apply) Pramipexole Ropinirole Rasagiline and selegiline Benztropine and trihexyphenidyl Amantadine

71
Figure 1. The mechanism of potentiation of cardiovascular effects of tyramine, the cheese reaction, and NE release and metabolism after MAO-A inhibition. Figure 1. The mechanism of potentiation of cardiovascular effects of tyramine, the cheese reaction, and NE release and metabolism after MAO-A inhibition. Youdim M B , Riederer P F Neurology 2004;63:S32-S35 ©2004 by Lippincott Williams & Wilkins

72
Mechanism of action of MAOI (no pdf)
Treatment interventions in PD: and evidence based assessment. Rascol et al. Lancet 2002;359:1589. Evidence-based medical review update: Pharmacological and surgical treatments of PD: Movement Disorders 2005;20(5):523
:523.")
73
Goetz CG, Koller WC, Poewe W, et al
Goetz CG, Koller WC, Poewe W, et al. Management of Parkinson’s disease: an evidence-based review. Mov Disord 2002;17(Suppl. 4)S1–S166. Update on the medical management of parkinson disease. Continuum 2010;16:96-109 Chaudhuri et al. Non-motor symptoms of Parkinson’s disease: diagnosis and management. Lancet Neurol 2006;5:
S1–S166. Update on the medical management of parkinson disease. Continuum 2010;16: Chaudhuri et al. Non-motor symptoms of Parkinson’s disease: diagnosis and management. Lancet Neurol 2006;5:")
74
Figure 2. The pathway of dopamine (DA) synthesis from levodopa (l-dopa) and its metabolism by intraneuronal MAO-A and by MAO-A and B extraneuronally by glia and astrocytes and the inhibition of MAO by various selective (moclobemide, selegiline, rasagiline) ... Figure 2. The pathway of dopamine (DA) synthesis from levodopa (l-dopa) and its metabolism by intraneuronal MAO-A and by MAO-A and B extraneuronally by glia and astrocytes and the inhibition of MAO by various selective (moclobemide, selegiline, rasagiline) and nonselective (TV3326) inhibitors. D1 and D2″ = dopamine receptors; DAT = dopamine transporter; AR = amine reuptake; SV = synaptic vesicle; DDC = dopa decarboxylase; COMT = catechol-o-methyl transferase; 3OMD = O-methyl dopa. Youdim M B , Riederer P F Neurology 2004;63:S32-S35 ©2004 by Lippincott Williams & Wilkins
 synthesis from levodopa (l-dopa) and its metabolism by intraneuronal MAO-A and by MAO-A and B extraneuronally by glia and astrocytes and the inhibition of MAO by various selective (moclobemide, selegiline, rasagiline) and nonselective (TV3326) inhibitors. D1 and D2″ = dopamine receptors; DAT = dopamine transporter; AR = amine reuptake; SV = synaptic vesicle; DDC = dopa decarboxylase; COMT = catechol-o-methyl transferase; 3OMD = O-methyl dopa. Youdim M B , Riederer P F Neurology 2004;63:S32-S35. ©2004 by Lippincott Williams & Wilkins.")
75
Which of the following sleep disorders is most common in patients with Parkinson disease?
A. central sleep apnea B. delayed sleep phase syndrome C. narcolepsy D. REM sleep behavior disorder

Similar presentations





 Treatment Update. Outlines The Basics: – PD Introduction and motor symptoms. – DDx not to miss. – Different classes of Anti PD.>")




>")

 are a class of powerful antidepressant drugs. They are particularly effective in treating.>")



>")





