Download presentation
Presentation is loading. Please wait.

1
Oxford The John Radcliffe Hospital Multi-vessel disease… Le Mans implications Dr Adrian Banning

2
Multi-vessel disease… Le Mans - implications ? Lemans trial J Am Coll Cardiol 2008 –Small randomised trial of CABG vs PCI for patients with left main disease Syntax Lemans –Subset of the Syntax trial –patients with left main disease –follow up angios at 15 months (both surgical and PCI) –To be reported at PCR 09
 –To be reported at PCR 09.")
3
Why is the Left Main important? It supplies at least 2/3 of the blood to the heart!!!

4
Why is the left main special? Large vessel –Prone to calcification –Large volume of plaque required to cause stenosis –Intubated by the diagnostic catheter –ostium? –By definition terminates in a bifurcation – at least Untreated LMS stenosis > 20% mortality at 1yr

5
Results of initial intervention on the LMS- the early years 1980s Hartzler using POBA –10% procedural mortality in hospital –64% 3yr mortality Early 1993-8 ULTIMA –279 pts unprotected LMS –14% procedural mortality in hospital –25% mortality at one year –NB if 46% inoperable are excluded – 97% 1yr survival in these low risk pts

6
Can we predict risk when stenting the LMS?

7
Stent the LMS with BMS safe, but high rate of MACE due to restenosis Am J Cardiol. 2003;91:12-6.

8
103 patients BMS (n 50) or PES (n 53). All IVUS guidance and Cutting balloon pretreatment x 3 to cover entire lesion Ostium and body were treated with a single stent Single stent 49/50 and 52/53 Final kissing balloon dilation was performed only in cases with suboptimal result at the LCX ostium (6% and 19%) Follow-up: 6 months angio and IVUS No “late” stent thrombosis in either group A Randomized Comparison of Paclitaxel-Eluting Stents Versus Bare-Metal Stents for Treatment of Unprotected Left Main Coronary Artery Stenosis Erglis et al JACC 2007
 Follow-up: 6 months angio and IVUS No late stent thrombosis in either group A Randomized Comparison of Paclitaxel-Eluting Stents Versus Bare-Metal Stents for Treatment of Unprotected Left Main Coronary Artery Stenosis Erglis et al JACC")
9
A Randomized Comparison of Paclitaxel-Eluting Stents Versus Bare-Metal Stents for Treatment of Unprotected Left Main Coronary Artery Stenosis Erglis et al JACC 2007

10
A Randomized Comparison of Paclitaxel-Eluting Stents Versus Bare-Metal Stents for Treatment of Unprotected Left Main Coronary Artery Stenosis Erglis et al JACC 2007

11
A Randomized Comparison of Paclitaxel-Eluting Stents Versus Bare-Metal Stents for Treatment of Unprotected Left Main Coronary Artery Stenosis Erglis et al JACC 2007

12
A Randomized Comparison of Paclitaxel-Eluting Stents Versus Bare-Metal Stents for Treatment of Unprotected Left Main Coronary Artery Stenosis

13
Location matters Distal- bifurcation Shaft Ostium

14
What makes the left main special? Anatomy matters –OstialNeeds 1 stent –BodyNeeds 1 stent –Bifurcation Usually >1 stent, 2 wires, >6F

15
Preliminary DES in LMS disease?

16
Long-Term Outcome After DES in Nonbifurcation Lesions that involve Unprotected LMS Chieffo et al Circulation 2007 Population: 147 pts elective (only) consecutive pts SES or PES in 5 centers - stenosis in the ostium and/or the mid-shaft of an unprotected LMCA PCI instead of surgery was considered either (1) suitable anatomy for stenting and preference patient and physician (2) suitable anatomy for stenting and EuroSCORE 6 and/or Parsonnet score 13 and/or prior bypass surgery with failure of all conduits (n=2).
 consecutive pts SES or PES in 5 centers - stenosis in the ostium and/or the mid-shaft of an unprotected LMCA PCI instead of surgery was considered either (1) suitable anatomy for stenting and preference patient and physician (2) suitable anatomy for stenting and EuroSCORE 6 and/or Parsonnet score 13 and/or prior bypass surgery with failure of all conduits (n=2).")
17
Favorable Long-Term Outcome After Drug-Eluting Stent Implantation in Nonbifurcation Lesions That Involve Unprotected Left Main Coronary Chieffo et al Circulation 2007 Medications: IIb/IIIa inhibitors at the discretion of the operator. Dual antiplatelet therapy for at least 6 months after. All patients were advised to maintain lifelong use of aspirin (100 mg/d). Clinical follow-up: at 1, 6, 12, and 24 months. Patients eligible for longer clinical follow-up were contacted at 36 and 48 months. Angio follow-up: 4 and 9 months or earlier if neccesary Total follow up mean 886 days
. Clinical follow-up: at 1, 6, 12, and 24 months. Patients eligible for longer clinical follow-up were contacted at 36 and 48 months. Angio follow-up: 4 and 9 months or earlier if neccesary Total follow up mean 886 days.")
18
Favorable Long-Term Outcome After Drug-Eluting Stent Implantation in Nonbifurcation Lesions That Involve Unprotected Left Main Coronary Chieffo et al Circulation 2007

19
Favorable Long-Term Outcome After Drug-Eluting Stent Implantation in Nonbifurcation Lesions That Involve Unprotected Left Main Coronary Chieffo et al Circulation 2007

20
Favorable Long-Term Outcome After Drug-Eluting Stent Implantation in Nonbifurcation Lesions That Involve Unprotected Left Main Coronary Chieffo et al Circulation 2007

21
Favorable Long-Term Outcome After Drug-Eluting Stent Implantation in Nonbifurcation Lesions That Involve Unprotected Left Main Coronary Chieffo et al Circulation 2007

22
Favorable Long-Term Outcome After Drug-Eluting Stent Implantation in Nonbifurcation Lesions That Involve Unprotected Left Main Coronary Chieffo et al Circulation 2007 No proven late stent thrombosis 4 unexpected deaths

23
Favorable Long-Term Outcome After Drug-Eluting Stent Implantation in Nonbifurcation Lesions That Involve Unprotected Left Main Coronary Chieffo et al Circulation 2007

24
What about late stent thrombosis in LMS disease? Specific worries –Late thrombosis for all DES >BMS –Late thrombosis higher off label –Higher risk of incomplete expansion? –Left main occlusion will be fatal Reassurances –Big vessel

25
Late and very late stent thrombosis following DES in ULM. Chieffo et al, EHJ Sept 2008. Multicentre registry of 731 pts with Elective DES stenting of ULM disease. Definite ST 4 pts (0.5%). 3 early (≤30d), 1 late (≤ 1 yr). No VLST. Probable ST = 3 pts. All early (≤30d) Definite or probable ST = 7 / 731 = 0.95% All were on dual AP Rx. Possible ST (8 late, 12 very late) in 20 (2.7%) pts.
. 3 early (≤30d), 1 late (≤ 1 yr). No VLST. Probable ST = 3 pts. All early (≤30d) Definite or probable ST = 7 / 731 = 0.95% All were on dual AP Rx. Possible ST (8 late, 12 very late) in 20 (2.7%) pts..")
26
Late and very late stent thrombosis following DES in ULM. Chieffo et al, EHJ Sept 2008. Outcomes after 29.5±13.7 months follow up: –Death: 6.2% (n=45). –Cardiac death: 4.2% (n=31) –TVR: 12.9% (n=95) –TLR: 10.9% (n=76) –Restenosis rate: 14.1% on angiographic follow-up of 548 pts. (NB: 76% of lesions involved the distal LM.) Predictors of ST at logistic analysis: –Euroscore –LVEF Consistent with general PCI population. No unique ST predictor among ULM pts identified in this analysis. Conclusion: Elective DES stenting of ULM is safe - low rates of ST.
. –Cardiac death: 4.2% (n=31) –TVR: 12.9% (n=95) –TLR: 10.9% (n=76) –Restenosis rate: 14.1% on angiographic follow-up of 548 pts. (NB: 76% of lesions involved the distal LM.) Predictors of ST at logistic analysis: –Euroscore –LVEF Consistent with general PCI population. No unique ST predictor among ULM pts identified in this analysis. Conclusion: Elective DES stenting of ULM is safe - low rates of ST..")
27
358 consecutive patients 7 centres All DES

28
ElectiveUrgent MACE free74%68% Mortality6%21% Reinfarction 8%10% TLR7% 3% TVR16%7% DelftJ Am Coll Cardiol 2008 ; 51 2212-9

29
So can stents replace surgery in left main disease?

30
Unprotected left main stenting vs CABG Seung et al, NEJM April 2008. Long term follow up of 1102 patients stenting for ULM disease, vs propensity-matched cohort of CABG patients No significant difference in the risk of death and the composite outcome of death, Q-wave MI, or stroke between the two groups. TVR higher in the stents group, even with DES. Seung KB et al. N Engl J Med 2008;358:1781-1792

31
Study of unprotected LEft MAiN Stenting versus bypass surgery J Am Coll Cardiol 2008; 51: 538-45

32
Lemans study design

33
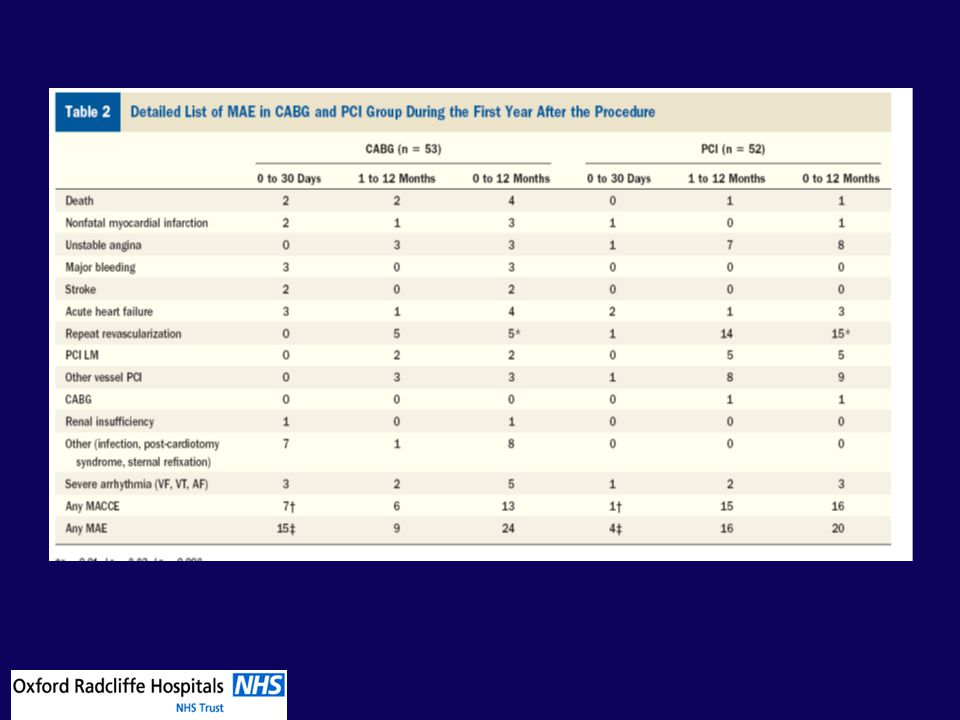
PCI technique Direct stenting preferred if not poss predil with 2 or 2.5 Bifurcation technique Initial stent to LAD then Cullotte or Prov T if necessary No crush stenting IVUS advised DES if diameter < 3.8mm (35%) LeMans study 2008
 LeMans study 2008")
36
Lemans trial 2008 Improved EF with PCI ETT similar by 12 months more angina PCI initially

37
LeMans survival

38
Left Main Disease (isolated, +1, +2 or +3 vessels) 3 Vessel Disease (revasc all 3 vascular territories) SYNTAX Eligible Patients De novo disease Limited Exclusion Criteria Previous interventions Acute MI with CPK>2x Concomitant cardiac surgery
 3 Vessel Disease (revasc all 3 vascular territories) SYNTAX Eligible Patients De novo disease Limited Exclusion Criteria Previous interventions Acute MI with CPK>2x Concomitant cardiac surgery")
39
Syntax Lemans (reports PCR 09) All left main pts in the randomised Syntax n=710 Follow up angio at 15 months Asses late angio outcomes with clinical outcomes Asses utility of angio follow up Stats –Surgery occlusion rate rate 5-12% 100 surgery pts 95% confidence interval (+/-0.043) if occlusion is 5% or (+/-0.043) if occlusion is 12% –PCI Expected Patency rate 74-97% 100 PCI pts 95% confidence interval (+/-0.078) if patency is 80% –Expected attrition 30%
 All left main pts in the randomised Syntax n=710 Follow up angio at 15 months Asses late angio outcomes with clinical outcomes Asses utility of angio follow up Stats –Surgery occlusion rate rate 5-12% 100 surgery pts 95% confidence interval (+/-0.043) if occlusion is 5% or (+/-0.043) if occlusion is 12% –PCI Expected Patency rate 74-97% 100 PCI pts 95% confidence interval (+/-0.078) if patency is 80% –Expected attrition 30%")
40
12 Month LM Subgroup MACCE Rates CABGTAXUS Left Main Isolated Left Main + 3VD Left Main + 2VD Left Main + 1VD N=258 (37%) N=218 (31%) N=138 (20%) N=91 (13%) All LM N=705 Patients (%)
 N=218 (31%) N=138 (20%) N=91 (13%) All LM N=705 Patients (%)")
41
12 Month Subgroup MACCE Rates All LM N=705 LM+1VD N=138 LM isolated N=91 LM+2VD N=218 LM+3VD N=258 Patients (%) 3VD (All) N=1095 CABGTAXUS
 3VD (All) N=1095 CABGTAXUS")
42
So why is the left main special? The left main is unforgiving during PCI –Because large volumes of myocardium are at risk –Large volumes of plaque may move –Calcification is restrictive to stent expansion –loss of “branches” will have immediate and profound haemodynamic consequences The left main is unforgiving in the long term –All ostial disease has a very high restenosis rate (particularly if the stent is incompletely expanded).
..")
43
What do we know about left main PCI? Procedural risk fallen from 10-20% to <1% (in all but shock cases) Ostial and shaft disease is different to terminal disease of the main Left main PCI should be definitely considered in all emerg ency cases and many urgent cases
 Ostial and shaft disease is different to terminal disease of the main Left main PCI should be definitely considered in all emerg ency cases and many urgent cases.")
44
What do we know about left main PCI in 2008? DES are almost certainly better than BMS Risks of treating left main disease with PCI or surgery are probably the same Long term results of DES in elective ostial and shaft disease are very encouraging –Those cases treatable with one properly expanded stent

45
What do we know about left main PCI in 2008? However –How do we treat distal bifurcation disease best? Perhaps the cullotte? Not the crush for me LMS + 2VD / 3VD –surgery still has lower rates of TVR particularly in diabetics

46
OSTIUMBODY DISTAL 1 STENT DISTAL 2 STENT CABG UNSUITABLE URGENT ELECTIVE Isolated left main stenting in 2008…

Similar presentations