Download presentation
Presentation is loading. Please wait.

1
A Review of Mental Health Acute Admissions
Dr R Belgamwar, Mrs L Wrench, Mrs R Purkayastha, Dr R Johnston and Dr J Christie - GP Trainees, Dr M Abdelrahman -F1 Trainee 1. National Service Framework for Mental Health: Department of Health, September 1999.

2
‘Acute inpatient care is a core and integral component of the National Service Framework for mental Health to which all the NSF standards are relevant…reshaping the organisation of inpatient services to provide a more effective, safe and therapeutic inpatient experience built around the needs of the service users, their families and carers is a NSF priority’ 1

3
Background According to the Mental Health Policy Implementation Guide, it has been reported by service users that admission to acute inpatient care is in itself distressing and demeaning, therefore it is paramount that assessment, care delivery and discharge planning should be wholly focused around the service user.

4
Locally major changes have taken place e.g.
The abolition of inpatient services in two mental health resource centres Reconfiguration and reduction of beds within Harplands Hospital The changes to single sex ward environment. Increase in the multidisciplinary therapy and activities provision Role of crisis/HT team in gate keeping admissions Providing named care-coordinator 7 day follow up in the community The ward changes have occurred via a phased approach starting from October 2005

5
Aim To evaluate the new service model with a view to improving Acute Adult Mental Health Care. Objectives To compare NSCHT adult mental health inpatient statistics against national performance indicators and statistics. To ascertain the current level of service provided to adult mental health inpatients.

6
Method Part 1 Electronic Reporting Comparison of Before and After Ward Restructuring The following samples were identified by the North Staffordshire Health Intelligence Service (HIS) using the Combined Healthcare Hospital Information Processing System. All patients discharged from Harplands wards and resource centres between 1st January 05 to 30th June 05 1st December 06 to 31st May 07 1st September 2007 and 29th February 2008 Data included: General demographic details Length of stay (episode) Number of occupied bed days Admission rate Type of patient (formal / informal) Referral source Discharge diagnosis Readmissions within 28 days No of incidents for the period
 using the Combined Healthcare Hospital Information Processing System. All patients discharged from Harplands wards and resource centres between. 1st January 05 to 30th June 05. 1st December 06 to 31st May 07. 1st September 2007 and 29th February Data included: General demographic details. Length of stay (episode) Number of occupied bed days. Admission rate. Type of patient (formal / informal) Referral source. Discharge diagnosis. Readmissions within 28 days. No of incidents for the period.")
7
Method Part 2 Review of Acute Admissions and Assessments
All patients discharged from the following locations between 1st September 2007 and 29th February 2008 (inclusive) Harplands Wards 1,2 and 3 County Resource Centres (Ashcombe and Lymebrook) City Resource Centres (Sutherland and Bennett) A random sample of 50 patients was selected from the Harplands Wards (1, 2 and 3) and another 50 patients were selected from the Resource Centres. Casenotes of a final sample of 86 patients were reviewed from admission to discharge.
 Harplands Wards 1,2 and 3. County Resource Centres (Ashcombe and Lymebrook) City Resource Centres (Sutherland and Bennett) A random sample of 50 patients was selected from the Harplands Wards (1, 2 and 3) and another 50 patients were selected from the Resource Centres. Casenotes of a final sample of 86 patients were reviewed from admission to discharge.")
8
In the last 30 years….. The key aim of mental health care has been to support people to live independent lives through better care and treatment in the community E.g. In-patient psychiatric beds has fallen dramatically – 87,396 beds in 1980 to 29,802 beds in Rise in the community services – Includes CMH Teams, assertive outreach teams, crisis teams, community rehabilitation teams, home treatment teams etc.

9
How many inpatient beds?
Depends on several factors including deprivation, other community and support services such as crisis/HT, community houses, day centres/hospitals etc, local drivers and financial provisions. Gate keeping procedures and facilitation early discharge Any report giving an estimates become quickly outdated in view of rapidly changing scenario. Inpatient beds are most expensive component of mental health services Growing Independent and private sector inpatient provision Some reports of increased number of mentally ill people in prison and ?Inversely proportional to the available psychiatric beds.

10
Nick Nalladori, a carer In 2005/2006, more than two-thirds of the NHS budget for clinical mental health services in England was spent on in-patient psychiatric hospital care. However, in England, there are fewer in-patient beds now than at any other time. The Mental Health Act Commission found that between 2005 and 2007, 37% of all wards they visited were running at over 100% bed occupancy. Crisis resolution teams are intended to reduce the need for hospitalisation. However, as yet, they do not have sufficient staff to meet this aim. High bed occupancy does not arise only because the numbers of in-patient beds has been reduced but also because of ‘bed blocking’. References The Mental Health Act Commission (2008) Risk, Rights and Recovery. Twelfth Biennial Report 2005–2007. TSO (The Stationery Office). National Audit Office (2007) Helping People Through Mental Health Crisis: The Role of Crisis Resolution and Home Treatment Services. TSO (The Stationery Office).
 Risk, Rights and Recovery. Twelfth Biennial Report 2005–2007. TSO (The Stationery Office). National Audit Office (2007) Helping People Through Mental Health Crisis: The Role of Crisis Resolution and Home Treatment Services. TSO (The Stationery Office).")
11
Local factors Deprivation above average High unemployment
High mortality rate – Sentinel report dt: 01/12/2009- Stoke 204, North Staffs 170, South Staffs 171, Central Cheshire 161 (Per 100,000)
")
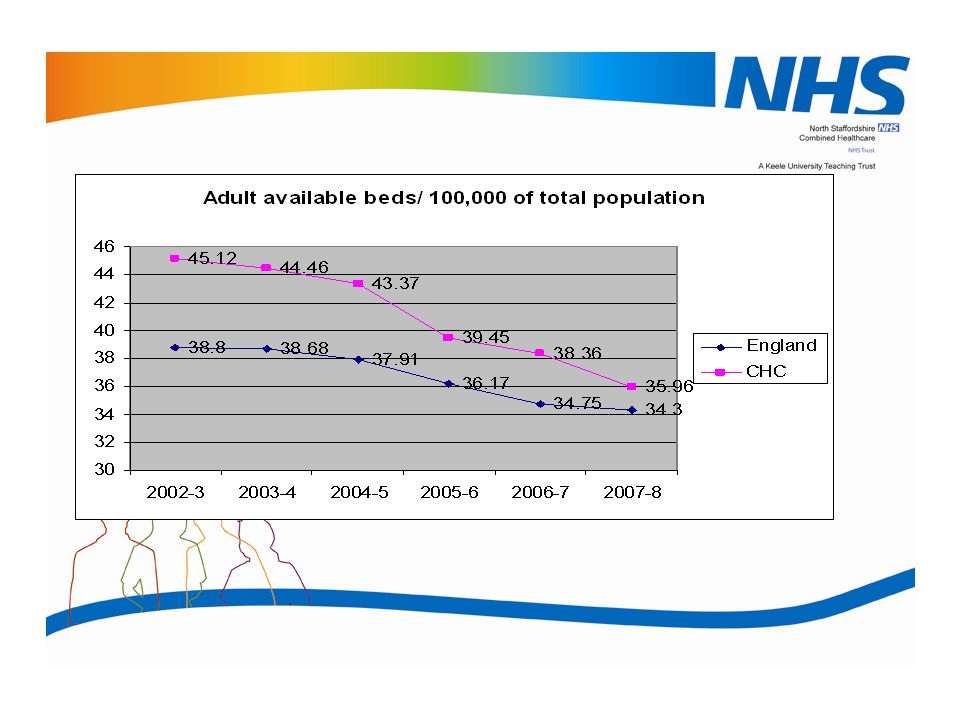
13
Current bed availability: 35.96/100,000
Excluding Rehab/Neuropsychiatry: 24.41/100,000 Excluding Community beds: 17.44/100,000 (Harplands and EMU) (England Reference 34.3/100,000)
 (England Reference 34.3/100,000)")
14
Bed availability 2007/8 Derbyshire MHT- 233 beds
South Staffordshire FT – 292 beds North Staffordshire – 165 beds Cheshire and Wirral – 194 beds Birmingham and Solihull beds Birmingham – 26% forensic beds South Staffordshire – 15% forens ic beds

15
Perinatal Psychiatry, Forensic Psychiatry, Eating disorders
Neuropsychiatry, Addiction, Rehablitation Psychiatry

16
Bed Availability Data source
Population reference - Mid 2006 Estimate: England: (100,000) CHC: (100,000) (North Staffs Stoke 24.76)
 CHC: (100,000) (North Staffs Stoke 24.76)")
17
Where are 181 beds? In 2005-06 we had Total 181 General Adult 109 beds
Rehabilitation 35 beds Neuropsychiatry 25 beds Addiction 12 beds Total 181

18
Changing adult inpatient bed availability
Speciality current 1 General Adult 109 96 2 Rehabilitation 35 28 3 Neuropsychiatry 25 4 Addiction 12 10 Total 181(39.45/100000) 159 (34.66/100000) England population 5076 (10 000); North Staffs population: = (1000): Both Mid 2006 estimates Kh03 Adult – ward classification included as 17 Mental illness: other ages: secure unit; 18 Mental illness: other ages: short stay and; 19 Mental illness: other ages: long stay 1. KH03 returns for 2009 will show 167 available beds (36.4/100000). For EMU we reported 14 beds instead of 10 and for Harplands ward 1( including PICU) we reported 24 beds instead of 20. So we have reported 8 extra beds. 2. KH03 England 2008 data for adult inpatient beds shows 17,411 available beds (34.3/100000)
 159 (34.66/100000) England population 5076 (10 000); North Staffs population: = (1000): Both Mid 2006 estimates. Kh03 Adult – ward classification included as. 17 Mental illness: other ages: secure unit; 18 Mental illness: other ages: short stay and; 19 Mental illness: other ages: long stay. 1. KH03 returns for 2009 will show 167 available beds (36.4/100000). For EMU we reported 14 beds instead of 10 and for Harplands ward 1( including PICU) we reported 24 beds instead of 20. So we have reported 8 extra beds. 2. KH03 England 2008 data for adult inpatient beds shows 17,411 available beds (34.3/100000)")
19
Conclusions In England, the number of available beds are reducing year on year, the trend is likely to continue particularly when significant financial cuts are expected. Over last 5 years, CHC Trust have reduced more beds compared to the average England beds for adult mental Illness. Our area has high rates of mortality, morbidity, deprivation and low life expectancy. In last 5 years, average bed occupancy rate has not significantly altered even with bed reductions. Locally, a third of our adult beds are for rehabilitation and neuropsychiatry services. This is probably much higher to the national average. These beds can be an income source for our Trust if there is an out of area commissioning/interest.

20
Results from electronic data

21
Patient Admissions by Ward and Resource Centre

24
Patient Primary Care Trust

25
Length of stay (days) per finished Consultant Episode
Period 1 Period 2 Period 3 Total FCE Length of Stay (days) 19121 14632 15974 No of FCEs 575 628 550 Average Length of Stay/FCE (days) 33.25 23.30 29.04
 No of FCEs Average Length of Stay/FCE (days)")
27
Readmissions within 28 days of discharge from previous admission
Period1 Period 2 Period 3 Readmissions - count 60 48 46 Readmissions - patients 50 34 37 Patient Analysis: 1 x readmissions 41 28 33 2 x readmissions 8 2 3 x readmissions 1 4 x readmissions 6 x readmissions Total

29
Conclusion – Part 1 The restructuring in provision of adult mental health care has resulted in a number of positive outcomes. There has been a clear reduction in number of patient admissions across all service areas. The length of stay of admitted patients has also reduced and once discharged, the patients have less frequently been readmitted. Clinical outcome measure are not recorded. The introduction of the Home Treatment and Crisis Teams have enabled some patients who may have previously been managed as inpatients, be successfully managed in the community, and have supported inpatients on discharge to prevent relapse and deterioration and subsequent readmission.

30
Conclusion – Part 1 Patient demographics didn’t change much. They are all of similar age, gender and ethnicity as compared to before service reform. The proportion of admissions from each PCT is also comparable, as is the admission source. There is a small variability in primary diagnosis at discharge however, with schizophrenia and delusional disorder being more commonly reported after service reform and mood disorder less so. The changes shows improved use of resources, accommodating bed reductions and bed availability for the more acutely unwell patient have benefits to the patients and clear financial benefits. The success of the ward restructuring at the Harplands is also suggested by the reduced number of reported incidents across. However more incidents were reported in the community inpatient setting early transfer from Harplands.

31
Acknowledgements for Part 1
Data analysis has been provided with kind support from L J McDermott and L Warrilow, North Staffordshire Combined Healthcare References Information for Health. Department of Health, 1998. Key Statistics Summary Data HSE online

32
Type of admission and Average Length of Stay (n=86)
Harplands 44 days County days City 63 days

33
Professional Recommending Admission (n=86)
Recommending Professional Number (%) Harplands (n=48) County (n=22) City (n=16) Consultant Psychiatrist 18(38%) 5(23%) 3(19%) Psychiatrist 12(25%) 2(9%) 2(12%) Crisis Team 6(13%) Nurse 3(6%) 4(18%) 5(31%) GP 1(7%) Unable to determine 4(8%) Other 2(4%) 3(14%) -
 Harplands. (n=48) County. (n=22) City. (n=16) Consultant Psychiatrist. 18(38%) 5(23%) 3(19%) Psychiatrist. 12(25%) 2(9%) 2(12%) Crisis Team. 6(13%) Nurse. 3(6%) 4(18%) 5(31%) GP. 1(7%) Unable to determine. 4(8%) Other. 2(4%) 3(14%) -")
34
Observation level on admission and Detentions
Number (%) Harplands (n=46) County (n=22) City (n=16) General 28(61%) 21(95%) 15(94%) Constant visual 3(6%) - Close intermittent 15(33%) 1(5%) 1(6%) 29% service users were detained at some point during their admission – most on sections 2 and 3
 Harplands. (n=46) County. (n=22) City. (n=16) General. 28(61%) 21(95%) 15(94%) Constant visual. 3(6%) - Close intermittent. 15(33%) 1(5%) 1(6%) 29% service users were detained at some point during their admission – most on sections 2 and 3.")
35
CPA level on discharge (n=86)
Number (%) Harplands (n=41) County (n=26) City (n=19) Standard 11(27%) 10(39%) 4(21%) Enhanced 27(66%) 16(61%) 14(74%) Not registered at time of discharge 3(7%) - 1(5%) Most common Care Coordinator was the CPN 66/83 (80%) service users had a discharge planning meeting prior to discharge In 39/50 (78%) cases the CC was present at the meeting
 Harplands. (n=41) County. (n=26) City. (n=19) Standard. 11(27%) 10(39%) 4(21%) Enhanced. 27(66%) 16(61%) 14(74%) Not registered at time of discharge. 3(7%) - 1(5%) Most common Care Coordinator was the CPN. 66/83 (80%) service users had a discharge planning meeting prior to discharge. In 39/50 (78%) cases the CC was present at the meeting.")
36
Discharge Letter sent to (n=61)
Discharge Letter (n=86) In 61/86 (71%) cases there was a discharge letter present in the notes In 27/61 (44%) cases the name of the care co-ordinator was present in the letter In 19/61 (31%) cases the contact details of the care co-ordinator was present in the letter Discharge Letter sent to (n=61) Average length of time between date of discharge and date letter sent was 7 days
 In 61/86 (71%) cases there was a discharge letter present in the notes. In 27/61 (44%) cases the name of the care co-ordinator was present in the letter. In 19/61 (31%) cases the contact details of the care co-ordinator was present in the letter. Discharge Letter sent to (n=61) Average length of time between date of discharge and date letter sent was 7 days.")
37
The pathway to recovery
A review of NHS Acute Inpatient Services Provides benchmarking Report published in 2008 with the aim to Support people to live independently in the community Strengthening community services Improvement in the quality of service Emphasis on high quality care and pathways to achieve best possible outcome

38
Health Care Commission Assessment Criteria
1. Effective care pathway To insure appropriate admission and discharge is timely Providing appropriate and safe interventions Workforce development Monitoring and evaluating service e.g. outcome measures 2. Individualised whole person care Focus on personalised care Promotes recovery and inclusion 3. Involvement of service users and cares Users and cares involvement in strategic planning, operational, evaluation and development 4. Safety The safety of service users, staff and visitors

39
THANK YOU and QUESTIONS

Similar presentations





 Program Social Assistance and its delivery through the Veterans Home Care Program 1.>")




 patients Policy.>")












