Download presentation
Presentation is loading. Please wait.

1
Acute treatment of migraine Mark Weatherall BASH meeting, Hull 2009

3
The intangibles Doctor-patient relationship Realistic expectations Education

4
Triggers Hormonal Dietary Psychological Environmental Sleep Drugs

6
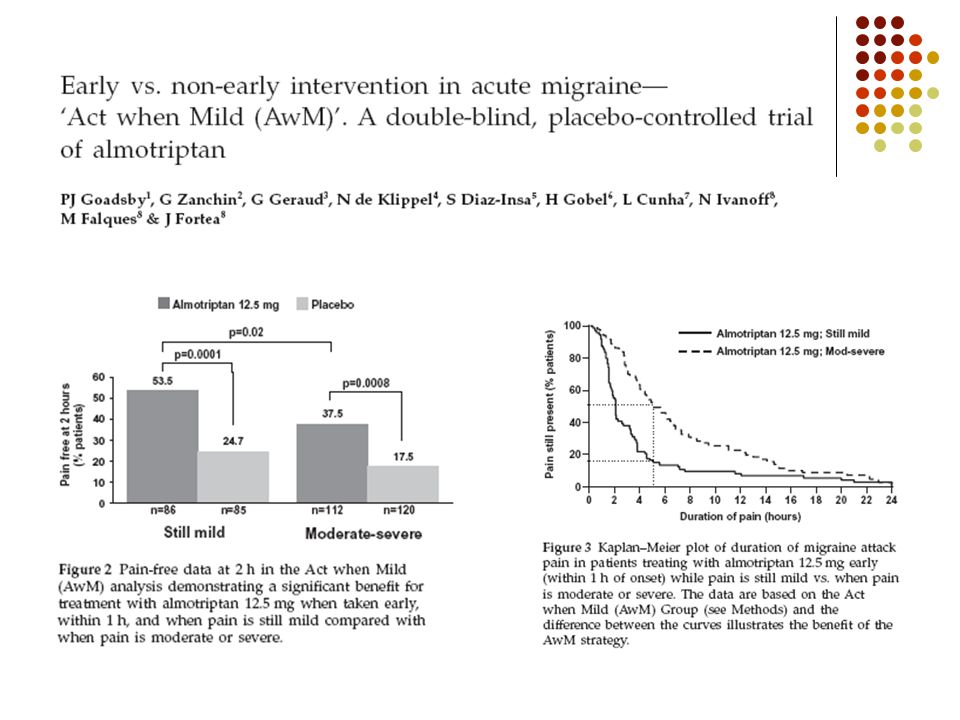
10 steps to success Make the diagnosis Use the right drugs Use effective doses Treat early when the pains mild Treat associated symptoms

7
10 steps to success Choose appropriate route of delivery Observe contraindications Use prior experience to select/reject drugs Avoid drugs with high potential for MOH Combine medications if necessary

9
Where to start? paracetamol 1 g or, aspirin 900 mg or, ibuprofen 600-800 mg +/- domperidone 10-20 mg taken as soon as possible*ª * i.e. as soon as the patient knows that this is a migraine ª if there is aura, take at the start of the headache phase

10
Variations on a theme if early nausea, you can use: soluble aspirin suppositories*: diclofenac 75 mg domperidone 30 mg *be French!

14
Headache response at 2 hr

15
Problems, problems… Not effective dose? timing? route? combination? Contraindications asthma, upper GI problems, renal impairment Side effects GI, CNS

16
This is what patients do next

17
Codeine…? … is NOT a treatment for headache the WHO analgesic ladder should NOT be applied to headache management

18
Triptans 5-HT 1B/1D receptor agonists seven different formulations options for route of delivery oral tablets or melts nasal spray subcutaneous injection taken as soon as possible*ª¹ * i.e. as soon as the patient knows that this is a migraine ª if there is aura, take at the start of the headache phase ¹ this is a race against the development of allodynia

20
Which triptan?

21
Headache response at 2 hr

22
Pain freedom at 2 hr

25
advantagesdisadvantages Sumatriptanwell-established expensive £4.60available OTCpoorly absorbed s/c (£22.10), melt (£4.14), nasal spray (£6.14) Zolmitriptancheaperoccasional confusion £4.00long acting nasal spray (£6.75), melt (£4.00) Naratriptancheaper slow onset £4.09long acting Rizatriptanrapid onsethigh recurrence £4.46melt (£4.46) Almotriptancheaper £3.02low SE incidence Eletriptancheaperpumped out of CNS £3.75long acting Frovatriptancheapestslow onset £2.78longest half-life
, melt (£4.14), nasal spray (£6.14) Zolmitriptancheaperoccasional confusion £4.00long acting nasal spray (£6.75), melt (£4.00) Naratriptancheaper slow onset £4.09long acting Rizatriptanrapid onsethigh recurrence £4.46melt (£4.46) Almotriptancheaper £3.02low SE incidence Eletriptancheaperpumped out of CNS £3.75long acting Frovatriptancheapestslow onset £2.78longest half-life")
26
Problems, problems… Ineffective dose? timing? route? switch? Headache recurrence switch? combination with NSAID? Contraindications HT, IHD SE nausea, GI, CNS, ‘triptan chest’

28
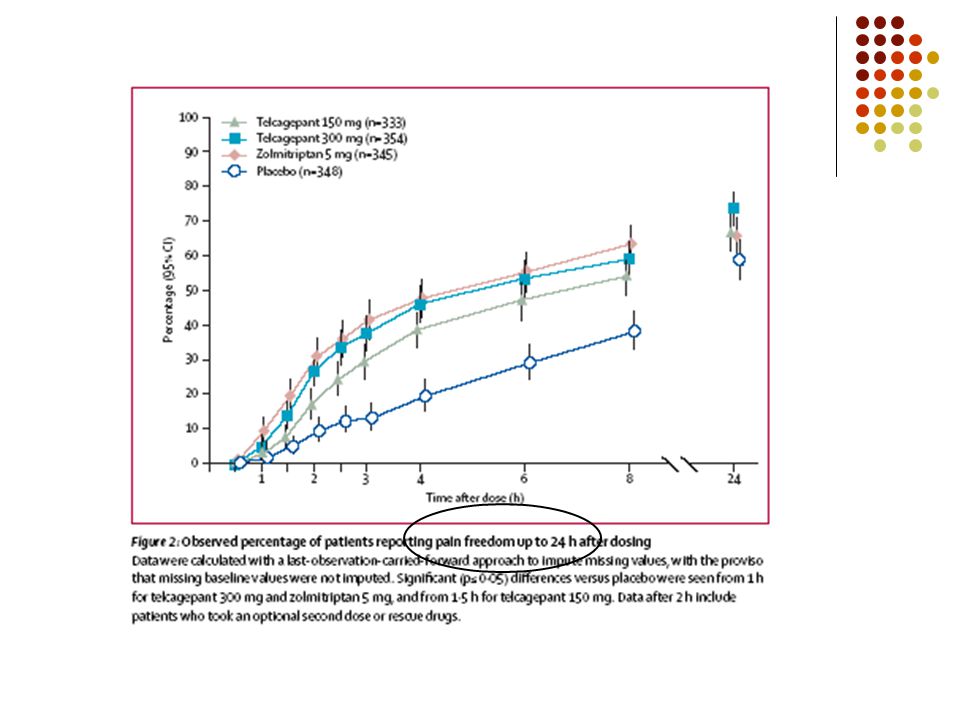
Is the future ‘pants’? CGRP antagonists two with data recently published proof-of-concept trial of intravenous BIBN4096BS (now called olcagepant) was published in NEJM in 2004 phase II study of oral CGRP antagonist MK-0974 (now called telcagepant) presented at IHS 2007 and published in Neurology in 2008
 was published in NEJM in 2004 phase II study of oral CGRP antagonist MK-0974 (now called telcagepant) presented at IHS 2007 and published in Neurology in")
29
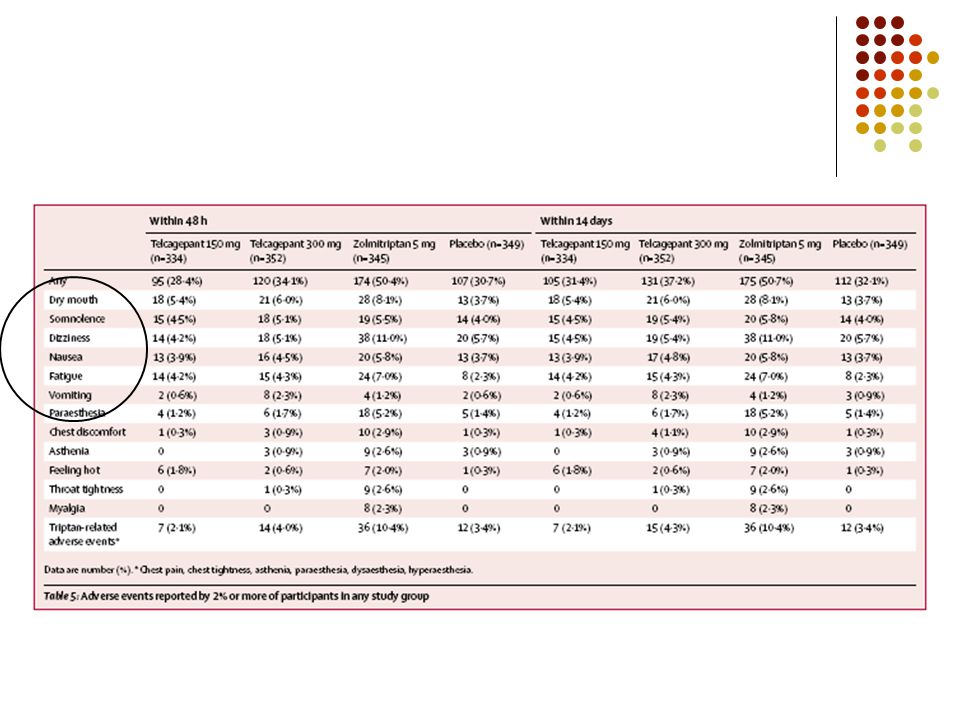
multicentre phase III R-PT-PC-DB-T of oral telcagepant 150 or 300 mg vs zolmitriptan 5 mg and placebo published in The Lancet in last four weeks

34
A&E/in-patient options sumatriptan s/c 6 mg alternatively nasal spray 20 mg high dose NSAIDs aspirin 1 g (available as IV formulation – useful as rescue medication in medication withdrawal) indometacin 100 mg (can be given IM)
 indometacin 100 mg (can be given IM)")
35
Refractory migraine dihydroergotamine (DHE) 0.5-1.0 mg iv/im (2 mg nasal spray) anticonvulsants sodium valproate 500 mg iv in 100 mL normal saline over 15 min (? role for SVP infusion in status migrainosus) clonazepam 1 mg/mL slow push
 clonazepam 1 mg/mL slow push.")
36
… or … dopamine antagonists metoclopramide 10-20 mg IV (rpt to 30-60 mg over 2 hrs) droperidol 0.625 mg every 10 mins (average effective dose 3.15 mg) prochlorperazine 10 mg iv over 2 min (may rpt after 30 min) metoclopramide & prochlorperazine can be followed with DHE 0.5-1.0 mg over 10 mins
 droperidol mg every 10 mins (average effective dose 3.15 mg) prochlorperazine 10 mg iv over 2 min (may rpt after 30 min) metoclopramide & prochlorperazine can be followed with DHE mg over 10 mins")
37
… or … magnesium sulphate 1 g iv over 15 min dexametasone 8-20 mg iv over 5-10 min; hydrocortisone 100-250 mg iv over 10 min, every 8-12 hrs for 24 hours (again, useful in status) ketorolac 30-60 mg iv/im
 ketorolac mg iv/im")
38
A final thought: listening is therapy in itself … and you’ve listened long enough!

Similar presentations