Download presentation
Presentation is loading. Please wait.

1
November 2012 Updates…… Curriculum WPBAs Recruitment QI: Learning To Make A Difference Programme

2
curriculum updates All CMT trainees (CT1 and CT2) are now using the same ‘live’ Curriculum apart from the few who started CMT before August 2011. All trainees using the 2012 amended Curriculum are using the 2012 ARCP Decision aid. Common Competencies and Emergency Presentations are unchanged. The Top 20 presentations have changed to “The Top Presentations – Common Medical Presentations”.

3
curriculum updates List of Top presentations is now 22 with new additions “Acute Kidney Injury and Chronic Kidney disease” “Management of patients requiring Palliative and end of Life Care”. Increased emphasis in existing grids for other topics: patient safety dementia back to work bioethics transitional care domestic violence obesity

4
CMT procedures from Aug 2011 essential, clinical independence mandatory (5) –CPR; LP; ascitic tap; pleural aspiration; NG tube essential, clinical independence desirable (3) –CV cannulation; DCCV; chest drain insertion using Seldinger technique with ultrasound guidance where appropriate desirable –abdominal paracentesis; knee aspiration; skin biopsy –(arterial lines; long lines; joint injections; temp pacing)
 –CPR; LP; ascitic tap; pleural aspiration; NG tube essential, clinical independence desirable (3) –CV cannulation; DCCV; chest drain insertion using Seldinger technique with ultrasound guidance where appropriate desirable –abdominal paracentesis; knee aspiration; skin biopsy –(arterial lines; long lines; joint injections; temp pacing)")
5
Procedures documentation from August ’12: stronger wording re competence and maintaining competence DOPS forms adjusted to clarify formative OR summative 2 (minimum) summative DOPS from separate assessors to confirm independence for life-threatening procedures new DOPS form for CV cannulation specialty DOPS forms to be more widely available (chest drain, DCCV, temporary pacing)
 summative DOPS from separate assessors to confirm independence for life-threatening procedures new DOPS form for CV cannulation specialty DOPS forms to be more widely available (chest drain, DCCV, temporary pacing)")
6
ARCP DA updates from Aug ’12 fewer WPBAs (CbD, mini-CEX, ACAT) –reduced to 10 pa (must include 4 ACATs) from 13.5 pa ‘evidence of engagement’ with curriculum all emergency and top presentations most common and other important presentations WPBAs, reflection, courses etc ‘evidence of engagement’ document - allow ‘group sign-off’ for common and other important
 –reduced to 10 pa (must include 4 ACATs) from 13.5 pa ‘evidence of engagement’ with curriculum all emergency and top presentations most common and other important presentations WPBAs, reflection, courses etc ‘evidence of engagement’ document - allow ‘group sign-off’ for common and other important")
7
‘evidence of engagement’ document CMT Year 1CMT Year 2 Common competencies These competencies require a minimum of 2 pieces of satisfactory evidence linked. WPBA can be included but reflection on clinical/learning events, teaching attendance, e- learning is acceptable. 50% ie >12 with this level of evidence indicates satisfactory progress in CT1. These competencies require a minimum of 2 pieces of satisfactory evidence linked. WPBA can be included but reflection on clinical/learning events, teaching attendance, e- learning is acceptable. 80% ie 20 with this level of evidence indicates satisfactory progress for CMT completion. Emergency presentations Each of these competencies require a minimum of 2 pieces of satisfactory evidence linked, at least 1 of which must be a WPBA. Each must then be signed off individually by the educational supervisor. Note Decision aid advice re anaphylaxis. All 4 to be achieved in CT1. Top PresentationsEach of these competencies require a minimum of 2 pieces of satisfactory evidence linked, at least 1 of which must be a WPBA. Each must then be signed off individually by the educational supervisor. 11 to be achieved in CT1. Each of these competencies require a minimum of 2 pieces of satisfactory evidence linked, at least 1 of which must be a WPBA. Each must then be signed off individually by the educational supervisor. All 22 to be achieved by the end of CT2. Other Important Presentations These competencies require a minimum of 2 pieces of satisfactory evidence linked. WPBA can be included but reflection on clinical/learning events, teaching attendance, e- learning is acceptable. 15 with this level of evidence indicates satisfactory progress in CT1. These competencies require a minimum of 2 pieces of satisfactory evidence linked. WPBA can be included but reflection on clinical/learning events, teaching attendance, e- learning is acceptable. 30 with this level of evidence indicates satisfactory progress for CMT completion.

8
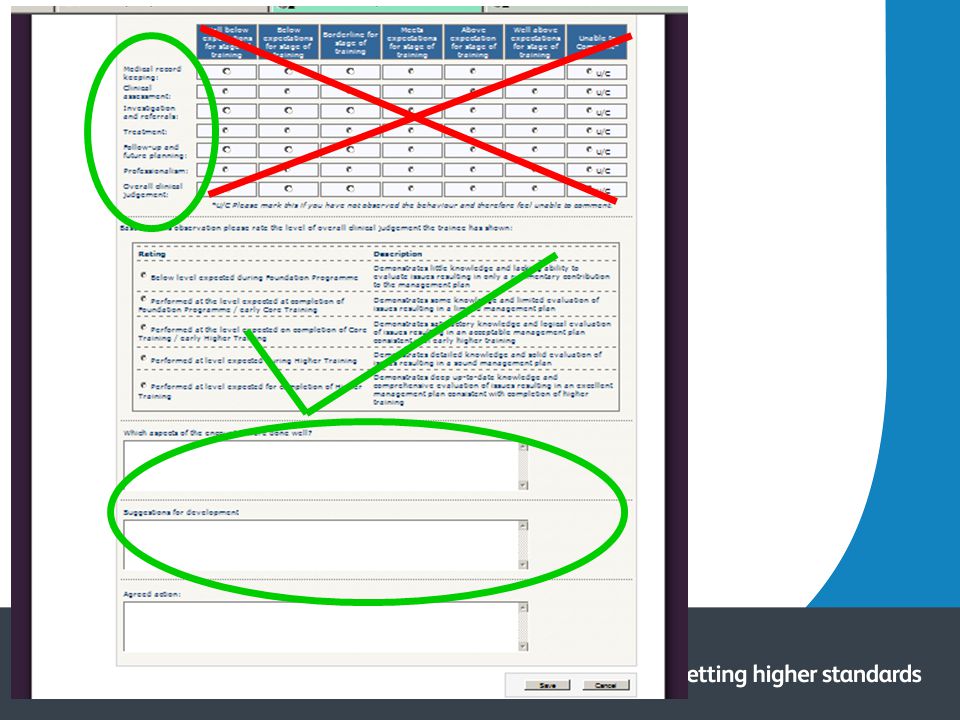
WPBA forms from Aug ’12 fewer but better forms simplified –‘radio buttons’ assessment for each domain removed –but free comments are required constructive feedback mandatory for WPBA to ‘count’ overall rating remains –CMT ratings will differ from HST ratings some forms (eg CV line insertion) remain accessible only from http://www.jrcptb.org.uk/assessment/Pages/WPBA- Documents.aspx http://www.jrcptb.org.uk/assessment/Pages/WPBA- Documents.aspx
 remain accessible only from Documents.aspx Documents.aspx")
10
DOPS form formative or summative (use latter for confirmation of competency) DOPS form for ‘potentially life threatening’ should be used for central line insertion, chest drains etc domain gradings retained but fewer –below, meets, above expectation for stage of training overall rating now includes skills lab competence Unable to perform the procedure Trained and competent in skills lab or course (this does not equate to clinical independence) Able to perform the procedure under direct supervision / assistance Able to perform the procedure with limited supervision / assistance Competent to perform the procedure unsupervised and deal with complications
 DOPS form for ‘potentially life threatening’ should be used for central line insertion, chest drains etc domain gradings retained but fewer –below, meets, above expectation for stage of training overall rating now includes skills lab competence Unable to perform the procedure Trained and competent in skills lab or course (this does not equate to clinical independence) Able to perform the procedure under direct supervision / assistance Able to perform the procedure with limited supervision / assistance Competent to perform the procedure unsupervised and deal with complications")
11
Top tips….. 1Be clear about, and agree, what you and the trainee want to achieve from the workplace-based assessments (WPBAs) at the start: CBD (Case-based Discussion) uses a case to explore the trainee ’ s application of knowledge, clinical reasoning and decision-making, including the ethical and professional aspects of the patient ’ s care. CBD is not just a discussion about an interesting case. ACAT (Acute Care Assessment Tool) is preferably used on an observed take (but may be on a ward round or covering a day's management of admissions and ward work) assessing clinical assessment & management, decision making, team working, time management, record keeping and handover for the whole time period and multiple patients. Any doctor who has been responsible for the supervision of the Acute Medical Take or ward-based shift can be the assessor for an ACAT. mini-CEX (Clinical Evaluation Exercise) is an observed trainee/patient interaction designed to assess clinical skills, attitudes and behaviour of the trainee. DOPS (Direct Observation of Procedural Skills) is assessing competency in a procedure; DOPS assessors need to be competent in the procedural skill that is being assessed. Directly observed procedural skills (DOPS) have been separated into two categories of routine and life-threatening procedures, with a clear differentiation of formative and summative sign off. Formative DOPS for routine and potentially life threatening procedures should be undertaken before doing a summative DOPS and can be undertaken as many times as the trainee and their supervisor feel is necessary. Summative DOPS should be undertaken as follows: 1.Summative sign off for routine procedures to be undertaken on one occasion with one assessor to confirm clinical independence. 2.Summative sign off for potentially life threatening procedures to be undertaken on two occasions with two different assessors (one assessor per occasion). MSF (Multi-source Feedback) provides a sample of attitudes and opinions of colleagues (medical, nursing, AHP & clerical) on the clinical performance and professional behaviour of the trainee; the request to do this WPBA will usually come as an email request from the trainee.
 at the start: CBD (Case-based Discussion) uses a case to explore the trainee ’ s application of knowledge, clinical reasoning and decision-making, including the ethical and professional aspects of the patient ’ s care. CBD is not just a discussion about an interesting case. ACAT (Acute Care Assessment Tool) is preferably used on an observed take (but may be on a ward round or covering a day s management of admissions and ward work) assessing clinical assessment & management, decision making, team working, time management, record keeping and handover for the whole time period and multiple patients. Any doctor who has been responsible for the supervision of the Acute Medical Take or ward-based shift can be the assessor for an ACAT. mini-CEX (Clinical Evaluation Exercise) is an observed trainee/patient interaction designed to assess clinical skills, attitudes and behaviour of the trainee. DOPS (Direct Observation of Procedural Skills) is assessing competency in a procedure; DOPS assessors need to be competent in the procedural skill that is being assessed. Directly observed procedural skills (DOPS) have been separated into two categories of routine and life-threatening procedures, with a clear differentiation of formative and summative sign off. Formative DOPS for routine and potentially life threatening procedures should be undertaken before doing a summative DOPS and can be undertaken as many times as the trainee and their supervisor feel is necessary. Summative DOPS should be undertaken as follows: 1.Summative sign off for routine procedures to be undertaken on one occasion with one assessor to confirm clinical independence. 2.Summative sign off for potentially life threatening procedures to be undertaken on two occasions with two different assessors (one assessor per occasion). MSF (Multi-source Feedback) provides a sample of attitudes and opinions of colleagues (medical, nursing, AHP & clerical) on the clinical performance and professional behaviour of the trainee; the request to do this WPBA will usually come as an request from the trainee..")
12
Top tips…. 2 Make the WPBA a positive learning experience – this is what it is all about and what trainees value the most. 3 Do the WPBA real-time and face-to-face – this makes it as close as possible to a real situation in which the trainee works. 4 Make time to do the WPBA – expect it to take 10-15 minutes of your time. 5Give constructive face-to-face verbal feedback immediately after the WPBA is completed as this enhances the process, increases the learning potential, and encourages immediate trainee reflection. 6Complete the necessary form on the ePortfolio at the time of the WPBA with a description of the case(s) and written feedback in the white space – it is easy to forget very quickly what was agreed.
 and written feedback in the white space – it is easy to forget very quickly what was agreed..")
13
educational supervisors form enhanced to improve feedback and cover more areas expanded summary of clinical skills: –has the trainee participated in appropriate clinical activity –comment on the range of in-patient and outpatient activity –has the trainee demonstrated appropriate K, S B –comment on clinical reasoning, diagnostic & decision- making skills etc reflection and study Quality Improvement added to audit section exam progress

14
for more information and FAQs re curriculum, documentation & ePortfolio updates see http://www.jrcptb.org.uk/trainingandcert/Pages/Chang estoCMTandGIMcurriculum2012.aspx

15
November 2012 Recruitment Update

16
Specialty Recruitment RCP-SRO coordinating recruitment since 2008 CMT & ACCS-acute at CT1 level 16 specialties at ST3 level Incorporates: –England –Northern Ireland (CT1 only) –Wales –Scotland (starting from 2013 recruitment).
 –Wales –Scotland (starting from 2013 recruitment).")
17
2012 - overview 98.5% fill rate (100% for ACCS-AM) Visiting assessor and poor performer pilots undertaken Process aligned with Scotland Scoring system made fully transparent Generally very positive feedback from all stakeholders Predictable process
 Visiting assessor and poor performer pilots undertaken Process aligned with Scotland Scoring system made fully transparent Generally very positive feedback from all stakeholders Predictable process")
18
2012 – deanery fill rates CMT postsACCS postsTotal posts Total CMT posts filled Total ACCS posts filled % CMT filled % ACCS filled % Total posts filled East Midlands North 49251492100.0% East Midlands South 31334313100.0% East of England 11491231149100.0% KSS 66470664100.0% London 2571226925712100.0% Mersey 630 0100.0%N/A100.0% North Western 9359890596.8%100.0%96.9% Northern 70575705100.0% Northern Ireland 660 64097.0%N/A97.0% Oxford 33336333100.0% Peninsula 4124340297.6%100.0%97.7% Severn 55762557100.0% Wales 7227457279.2%100.0%79.7% Wessex 51253512100.0% West Midlands 10021021002100.0% Yorkshire & Humber 15221541522100.0% Total 131360137312926098.4%100.0%98.5%

19
CT1 – timeline TimescaleActivity 15 Nov – 5 Dec Application period applications now open – approx 2800 expected for 1400 posts until 9 Jan Long & short-listing 90% will get first choice, virtually all will get an invite 21 Jan – 15 Feb Interview period interview format unchanged from previous years 1 MarchDeadline for first offers all CT/ST1 specialties must have released first set of offers. Recycling of offers will continue into March from 19 March Round 2approx half of deaneries will enter R2 for unfilled posts

20
CT1 - developments visiting assessors incorporated into CT1 process interview question bank fully reviewed data analysis to understand differences between deanery assessments

21
ST3 - update two rounds of recruitment to 16 ST3 specialties (~ 1200 posts, the majority of all ST3 posts) are now completed for posts commencing up until 31st March 2013 the single national centre model used in round 2 worked well, allowing efficiencies of scale and a truly national process – following review, this is likely to be repeated for round 2 recruitment in future years the applicant pool is too low for complete fill – only 734 eligible applications from 506 unique candidates were received for 440 NTN & LAT posts in round 2 recruitment for posts commencing from August 2013 will commence next March; all specialties will use either a single national centre or the single cascadable application system MRCP(UK) & MRCPI will be the only acceptable physician exams in 2013 (with a planned move to MRCP(UK) only in 2014).
 are now completed for posts commencing up until 31st March 2013 the single national centre model used in round 2 worked well, allowing efficiencies of scale and a truly national process – following review, this is likely to be repeated for round 2 recruitment in future years the applicant pool is too low for complete fill – only 734 eligible applications from 506 unique candidates were received for 440 NTN & LAT posts in round 2 recruitment for posts commencing from August 2013 will commence next March; all specialties will use either a single national centre or the single cascadable application system MRCP(UK) & MRCPI will be the only acceptable physician exams in 2013 (with a planned move to MRCP(UK) only in 2014).")
22
Further recruitment updates The UK Offers System (centralised, multi-specialty offers) is on track to be introduced in 2013 there will be a moratorium on CT2 recruitment for some specialties in 2013, but CMT can continue to recruit at this level, to replace trainees ‘lost’ to other specialties and to increase the CMT feed into ST3 there will be a moratorium on LAT recruitment for some specialties in 2013, but at present physician specialties are exempt. Further clarification is awaited, due to the impact that this decision could have on the running of acute hospital care provided by a significant number of our specialties, already running with gaps DH have mandated that all LAT recruitment must be done as part of the national process from 2013. An additional clinical lead for RCP-coordinated recruitment is required - all enquiries to ST3recruitment@rcplondon.ac.uk

23
Contact Any questions, comments, feedback: ct1recruitment@rcplondon.ac.uk st3recruitment@rcplondon.ac.uk

24
August 2012 Dr Emma Vaux – Clinical Lead Dr Katharine Woodall – Project Manager Learning to Make a Difference RCP/ JRCPTB

25
Pilot Study 2010/11 61 Trainees undertook 46 quality improvement projects across 5 deaneries Trainees were enthused by the process Positive participant experience - They felt they made a real difference to patient care at the front line LTMD has demonstrated more evidence of benefit to patients than any of the current workplace based assessments. (Publication Clin Med Dec 2012)
.")
26
From August 2011 Expectation set for CMTs to complete a QI project rather than clinical audit LTMD website and resources Deaneries to implement Variable success

27
April 2012 – Survey Survey sent to College Tutors and Trust Programme Directors Over 80 trainees were undertaking quality improvement projects Where no trainees were doing projects, 80% of respondents were considering introducing quality improvement projects But, often there is no clear process to facilitate quality improvement project implementation.

28
Keys to successful implementation Face to face meetings in each deanery by the clinical lead Further development of LTMD website eportfolio changes QI support

29
FACE TO FACE – DEMYSTIFY PROCESS 15 talks in 13 deaneries this autumn Speaking to trainees and supervisors at induction Disseminating induction packs

30
Website Recently updated: Revised trainee and supervisor packs Powerpoints from last year’s trainees Presentations on QI methods

31
ePORTFOLIO CHANGES Quality Improvement Project Assessment Tool (QIPAT) Quality improvement or clinical audit in curriculum and ARCP Decision Aids Recruitment application forms also recognise equal status QIPs
 Quality improvement or clinical audit in curriculum and ARCP Decision Aids Recruitment application forms also recognise equal status QIPs")
32
QI Champions A network of QI champions at Trust Level is being identified Support supervisors and trainees by acting as a knowledge resource Currently about 30 QI champions spread across UK

33
Developing networks London Deanery - QI training trainees & consultants Faculty for Medical Leadership NHSIII MEE/HEE Better Training Better Care Royal Berkshire Foundation Trust awarded 100K to implement LTMD approach across all specialties and grades LTMD programme £75K November 2012

34
Moving forward LTMD is no longer a pilot but expected practice LTMD programme enables training in improvement methodology for the development of new skills relevant to being a physician in the 21 st century Embed improvement methodology in CMT training Partnership working with other agencies to facilitate delivery Develop networks to support this process

35
What does this mean in practice for the trainee? AimHow?Time- frame All core medical trainees to do a QIP Provided with resources and supported by a supervisor 2012- 2013 Each trainee to think of a potential improvement idea (work on own, in small group) Think about what frustrates you, what is bothersome, what is your department where you are working or the trust ’ s quality agenda Multi-disciplinary team approach Sept/Oct 2012 Each trainee to start to develop an understanding of the framework Read the LTMD tool kits, review the website and learn about QI projects already done Sept/Oct 2012 Getting startedIdentify your supervisorOct/Nov 2012 Complete project May 2013Present regionally with potential national presentation May/Jun 2013
 Think about what frustrates you, what is bothersome, what is your department where you are working or the trust ’ s quality agenda Multi-disciplinary team approach Sept/Oct 2012 Each trainee to start to develop an understanding of the framework Read the LTMD tool kits, review the website and learn about QI projects already done Sept/Oct 2012 Getting startedIdentify your supervisorOct/Nov 2012 Complete project May 2013Present regionally with potential national presentation May/Jun")
36
What does this mean in practice for the Training Programme Director and College Tutors? Set the expectation and value –The trainee knows this matters to their Trust, training programme and so themselves Involve the College Tutors in helping getting started and maintaining momentum; identification QI champion for further support Set a regional date for all trainees to present May 2013 (Orally/posters) Confirm completion at ARCP (or if not done ensure completed audit cycle)
 Confirm completion at ARCP (or if not done ensure completed audit cycle).")
37
Contact Emma.vaux@royalberkshire.nhs.uk http://www.rcplondon.ac.uk/projects/learning-make-difference-ltmd

Similar presentations
>")

>")













 Changes to specialty trainee assessment and review August 2014 Guidance for Supervisors.>")


