Download presentation
Presentation is loading. Please wait.

1
HIGHLIGHTS FROM THE MN HIV SURVEILLANCE REPORT 2013 Minnesota Department of Health HIV/AIDS Surveillance System

3
Estimated Number of Persons Living with HIV/AIDS in Minnesota As of December 31, 2013, 7,723* persons are assumed alive and living in Minnesota with HIV/AIDS 4,095 living with HIV infection (non-AIDS) 3,628 living with AIDS * This number includes persons who reported Minnesota as their current state of residence, regardless of residence at time of diagnosis. Includes state prisoners and refugees arriving through the HIV+ Refugee Resettlement Program, as well as HIV+ refugee/immigrants arriving through other programs.

36
Minnesota HIV Treatment Cascade

37
Percentage of persons diagnosed with HIV engaged in selected stages of the continuum of care – Minnesota

38
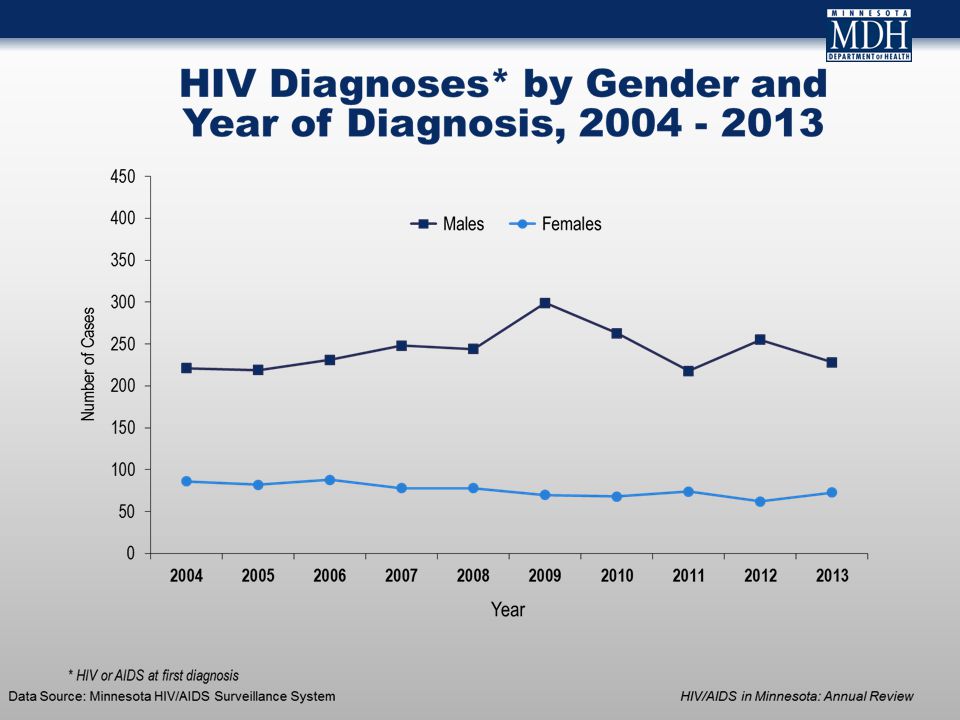
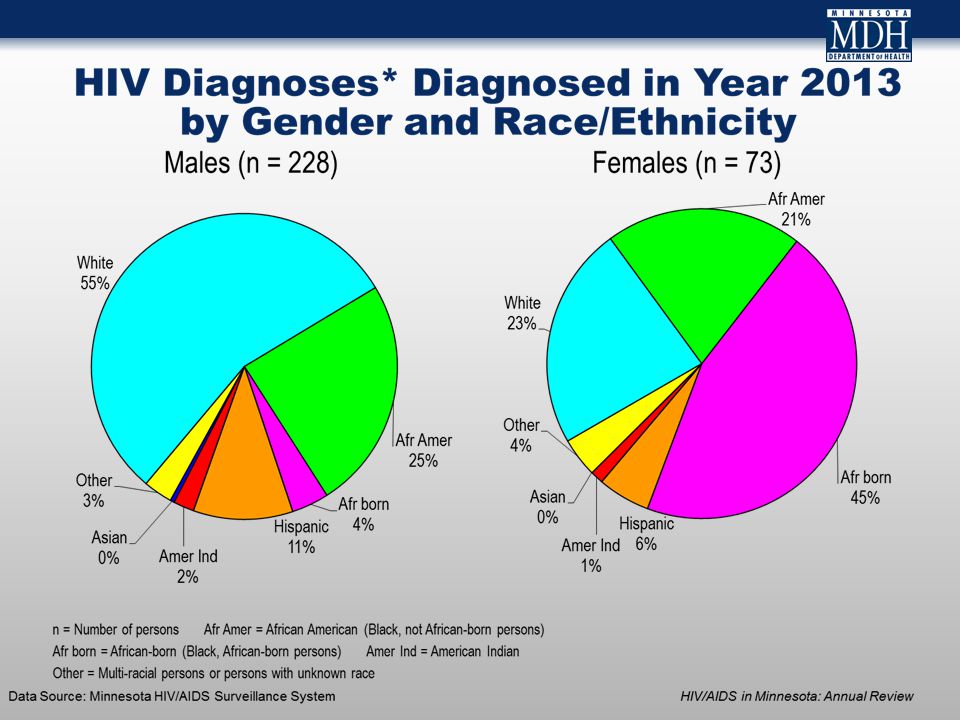
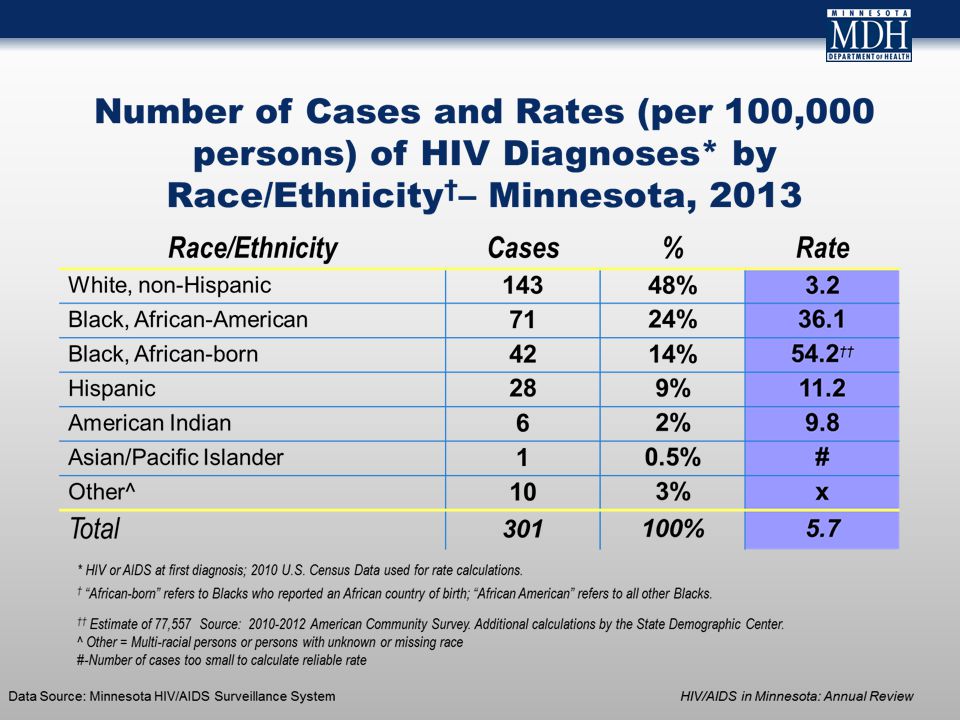
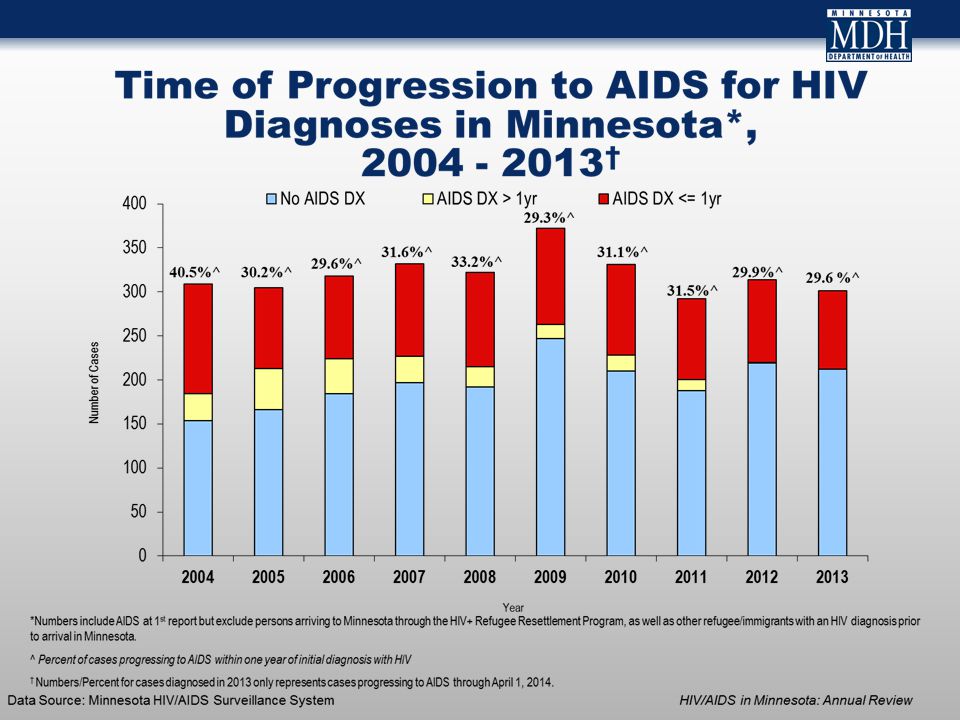
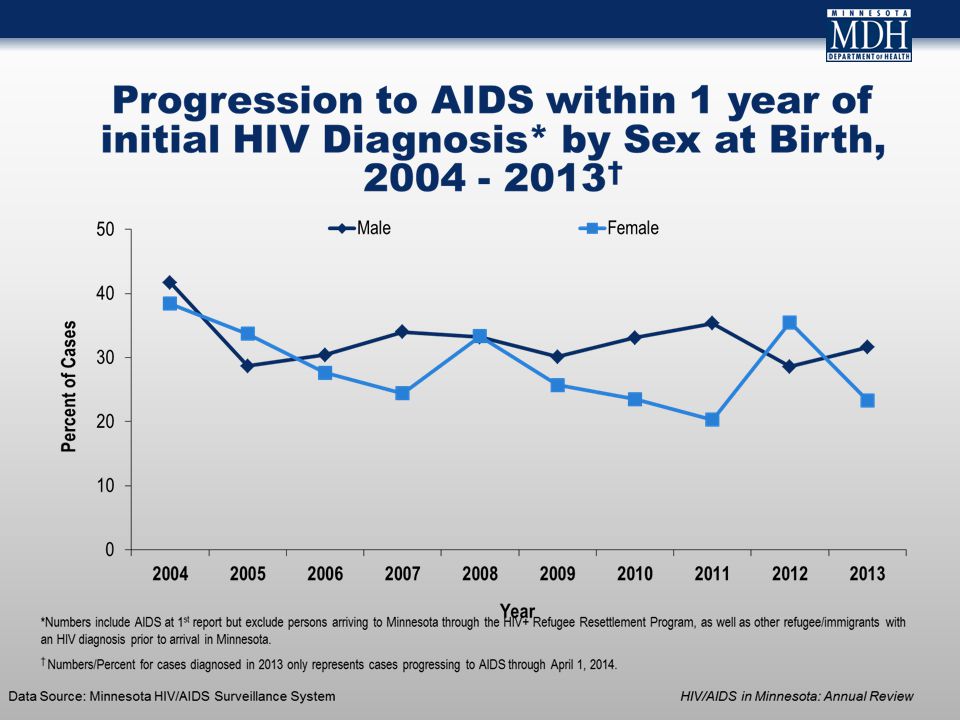
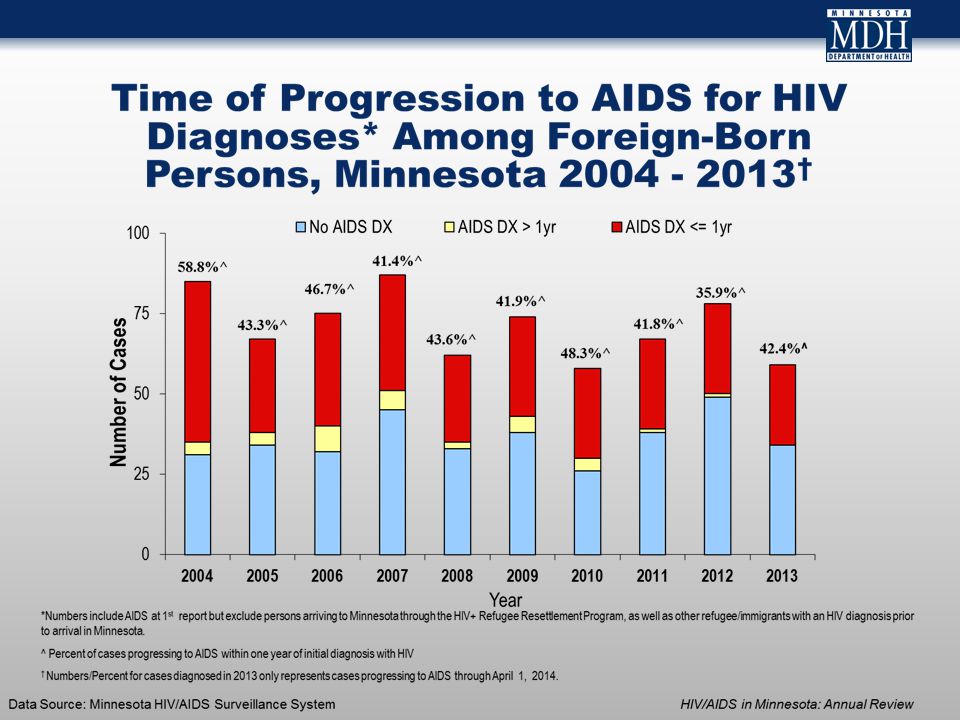
Conclusions There were 301 new HIV diagnoses reported in Minnesota in 2013, a decrease of 4% from 2012 Great disparities in HIV diagnoses persist among populations of color and American Indians living in Minnesota Male-to-male sex remains the leading risk factor for acquiring HIV/AIDS in Minnesota New HIV diagnoses remain concentrated in the Twin Cities seven-county metro area (82% of new diagnoses in 2013) Foreign-born persons made up nearly 1 in 5 of new HIV diagnoses in 2013, and progress from HIV to AIDS more quickly than U.S. born persons living with HIV in Minnesota

39
Thank You! For more information, please contact: Jessica Brehmer, HIV/AIDS Epidemiologist jessica.brehmer@state.mn.us (651) 201-5624
")
40
“The place where two discriminations exist is a dangerous place to live.” - Richard (Anguksuar) LaFortune Using Public Health Programming to Mitigate Disease and Death from Opiate Drug Use Sarah Gordon, MPH, NREMT-B
 LaFortune Using Public Health Programming to Mitigate Disease and Death from Opiate Drug Use Sarah Gordon, MPH, NREMT-B")
41
The issue is not simple…. disease, heroin, death, stigma, addiction, war on drugs, healthcare access, harm reduction Injection drug use is a well-known route of transmission of blood borne infections, particularly HIV and hepatitis B and C. Use of illicit drugs is associated with increased rates of TB and STDs. Recommended approaches, immunizations and screening, can protect the health of a person who uses drugs through medical interventions, while evidence-based behavioral interventions help prevent sexual and injection transmission by addressing risky behaviors.

42
Increase in Opiate Use In Minnesota 2005 - 2011 TwinCities.com DATA 2014 Maps show grams per 10,000 people of prescriptions for painkiller opiates (such as oxycodone, hydrocodone, codeine, morphine) in each three-digit ZIP code area. Source: Drug Enforcement Administration.

43
Heroin Influx in Midwest Courtesy Carol Falkowski Drug Abuse Trends June 2013, Drug Abuse Dialogues

44
Twin Cities has the cheapest and strongest heroin in the country, officials say By Aaron Rupar Thu., Jun. 6 2013 at 1:04 PMAaron Rupar At the newser, a doctor said there were four heroin-related deaths reported in Hennepin County in 2008. Last year, that number shot up to 37, and Hennepin County Sheriff Rich Stanek said the county is on pace to set a new record this year. Stanek also said the heroin he's seeing these days in Hennepin County is the cheapest and strongest in the country, a combination he characterized as particularly deadly. His comments reiterated what law enforcement officials said at a similar news conference last year. Then, they referenced an analysis showing that some heroin found on Twin Cities' streets was up to 93 percent pure, whereas typical American street heroin has a purity of about 35 percent. "A heroin user in the Twin Cities has a greater chance of accidental overdose because the purity of that heroin is so high," Stanek said during that news conference. At today's newser, officials pointed out the role prescription drugs play as a gateway to heroin. According to the Star Tribune, data showed that heroin and prescription drug abuse in the Twin Cities reached an all-time high last year. The two accounted for 21 percent of all addiction treatments in the state, with only alcohol abuse accounting for a higher share.what law enforcement officials said at a similar news conference last yearAccording to the Star Tribune

45
Courtesy Carol Falkowski, Drug Abuse Trends June 2012, Drug Abuse Dialogues

46
Heroin vs. other opiate treatment admission 1998-2013 Source: DAANES, PMQI, MN DHS 2014 Slide courtesy Rick Moldenhauer, DHS

48
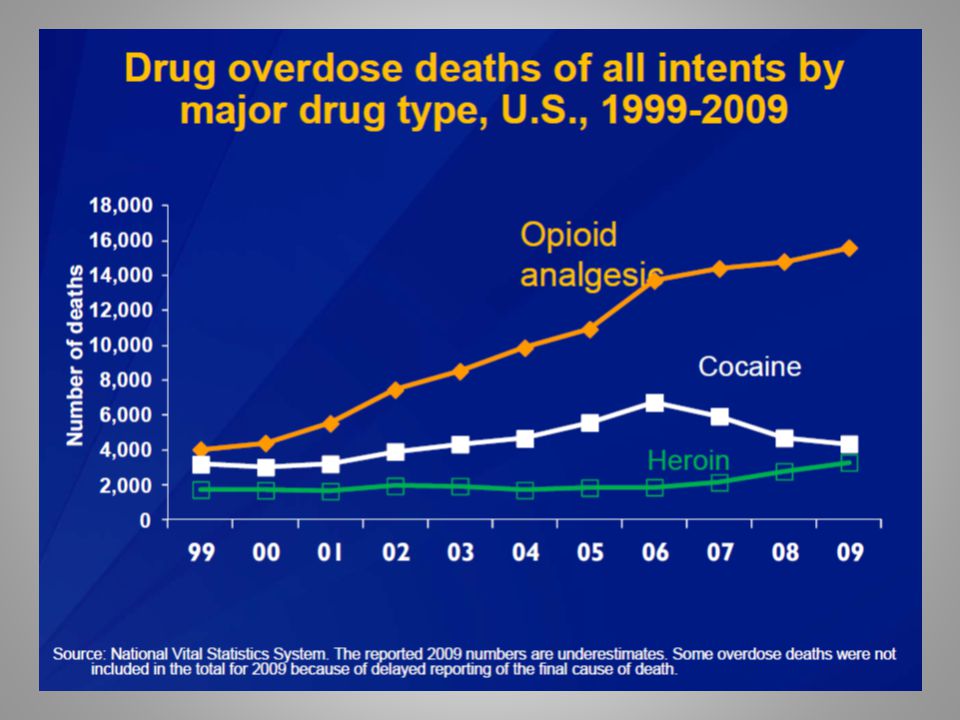
CDC Declares an Epidemic In 2010, overdose death become the leading cause of injury death in the US

50
Local Impact – Hennepin/Ramsey County Drug Deaths Hennepin County Medical Examiner and Ramsey County Medical Examiner, 2013

51
What makes opioid users at particular risk of overdose fatality? Among patients receiving opioid prescriptions for pain, higher opioid doses were associated with increased risk of opioid overdose death. Bohnert, et al. 2011 Poly-drug use Bohnert, et al. 2011 Substance use disorders and co-occuring mental health disorders Hall, et. al., 2008 Purity! Mexican heroin purity in Minneapolis highest in country and sold at lowest cost DEA Domestic Monitoring Program 2009

52
Fear! Fear of police response was the most commonly cited reason for not calling or delaying before calling for help Efforts to equip drug users to manage overdoses effectively, including training in first aid and the provision of naloxone, and the reduction of police involvement at overdose events may have a substantial impact on overdose-related morbidity and mortality. – Tracy, et al. Drug and Alcohol Dependence. 09/2005 What makes opioid users at particular risk of overdose fatality? (continued)
.")
53
Reality of drug use…. Non-fatal overdose in injection drug users – Lifetime prevalence ~ 40% – Of these ~ 70% reversed by naloxone – Lifetime witnesses ~ 90% Fatal – 1-3 hour window for medical intervention Sackoff et al. Ann Int Med, 2006; Ermak et al. 2009

54
The other reality of drug use….

55
Public Health Programming to Prevent Disease

56
Role of Needle Exchange in HIV and Hepatitis C Prevention Efforts The public health approach to disease prevention is to reduce risk of infection whether individual stops the risk behavior or not, which thereby protects the health of the community

57
Syringe Exchange is low-threshold entry point for drug users into prevention services and treatment Exchange participants 5x more likely to enter drug treatment than nonparticipants 67% of all exchange programs offer HCV testing and 87% offer HIV testing and linkage to care Since implementation of exchange programs in the late ’80s, HIV rates in injection drug users decreased overall by 80 %

58
Syringe Exchange Promotes Public Safety Post implementation of syringe exchange programs reduce number of syringes found in public areas…. – 50% drop in Baltimore – 2/3 reduction in Portland, OR Implementation of syringe exchange programs reduces needle-stick injuries to police…. – 2/3 injury reduction for Connecticut law enforcement – 66% reduction for Macon County, NC law enforcement

59
Testing is Prevention! 2 good reasons to get tested for HIV and HCV – If you have HIV and/or HCV, you can get treatment and healthy lifestyle education that may help you live a longer, healthier life. – If you do not have HIV or HCV, you can learn how to stay that way. Studies show persons who are aware of their status decrease behaviors that help transmit infection

60
911 Good Samaritan Laws Purpose: increase overdose survival rates by encouraging overdose witnesses to seek medical help through limited immunity from arrest and prosecution for minor drug and alcohol violation Good Sam laws do not protect from arrest for other offenses, such as selling or trafficking, or driving while drugged 15 states and District of Columbia have Good Sam policies – New Mexico, California, Colorado, New Jersey, New York, Rhode Island, Illinois, Florida, Massachusetts, Connecticut, North Carolina, Vermont, Delaware, Georgia, and Washington

61
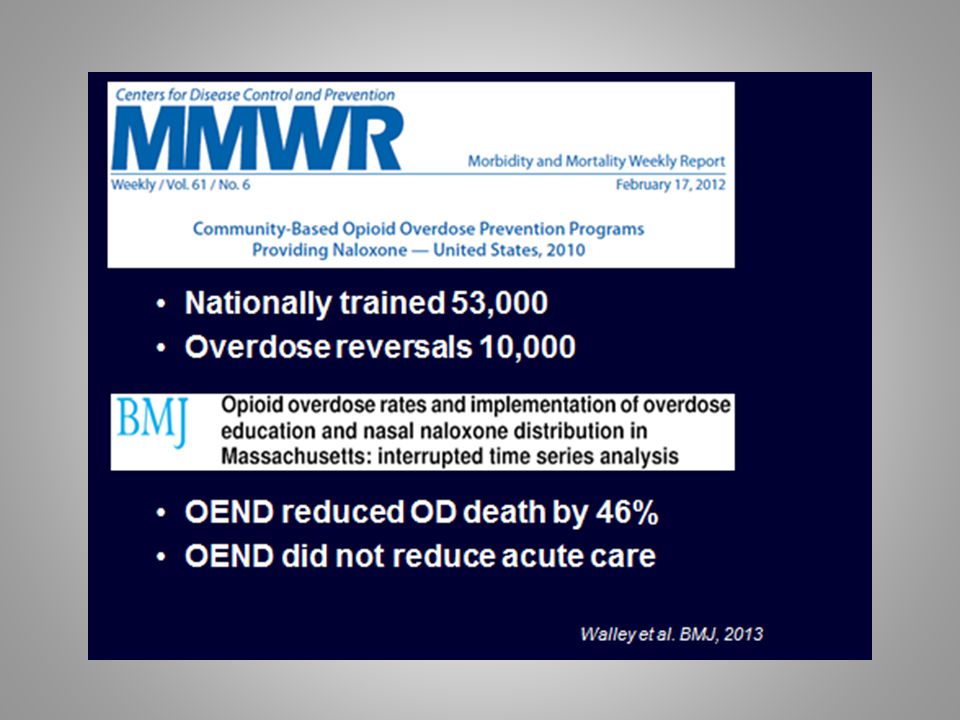
Broadening Naloxone Access Broader naloxone access policies puts overdose antidote in the hands of witnesses, first responders, community prevention programs – High affinity opioid receptor antagonist – Rapidly absorbed via IV, IM, SC, IN routes – Half-life ~ 40 minutes – Non-abusable – Adverse effect – withdrawal – Shelf-life – 3 years

62
What is the Overdose Antidote?

63
An Opiate Antagonist

65
What’s coming in MN? Steve's Law (HF2307 / SF1900) https://www.facebook.com/#!/911GoodSamar itanNaloxoneCampaign
 itanNaloxoneCampaign.")
66
Thank you!! For more information, please contact: Sarah Gordon, MPH Coordinator, HIV Testing and Syringe Services Programs Minnesota Department of Health 651-201-4011 sarah.gordon@state.mn.us

67
Hepatitis A, B & C in Minnesota, 2013 Minnesota Department of Health Hepatitis Surveillance System Minnesota Department of Health Hepatitis Surveillance System

68
Minnesota Hepatitis Surveillance System Hepatitis B reportable since 1987 Hepatitis C reportable since 1998 Passive data collection

69
Viral Hepatitis Overview

70
Data Source: Minnesota Viral Hepatitis Surveillance System Introduction Data in this presentation are current through 2013 Definitions: Acute case: Infected within the last six months Symptomatic OR negative test in six months before diagnosis Chronic case: Infected for over six months Asymptomatic or symptomatic Resolved cases: No evidence of current infection Evidence of past infection

71
Data Source: Minnesota Viral Hepatitis Surveillance System Data limitations The slides rely on data from HCV and HBV cases diagnosed through 2013 and reported to the Minnesota Department of Health (MDH) Hepatitis Surveillance System. Some limitations of surveillance data: Data do not include hepatitis-infected persons who have not been tested Data do not include persons whose positive test results have not been reported to the MDH Persons are assumed to be alive unless the MDH has knowledge of their death. Persons whose most recently reported state of residence was Minnesota are assumed to be currently residing in Minnesota unless the MDH has knowledge of their relocation.

72
Acute Viral Hepatitis Acute case: Infected within the last six months Symptomatic OR negative test within 6 months before diagnosis

73
Reported rate per 100,000 population of acute viral hepatitis United States, 1998-2011 Data Source: Viral Hepatitis Statistics & Surveillance at www.cdc.gov/hepatitis/Statistics/2011Surveillance/index.htm

74
Number of Acute* Cases per year Minnesota, 1998-2013 Data Source: MN Viral Hepatitis Surveillance System*Acute cases include seroconverters for all years for HBV and HCV

75
Chronic Viral Hepatitis

76
Overview of Chronic HBV in MN Chronic case: Infected for over six months Includes cases with no evidence of recent infection Asymptomatic or symptomatic

77
Reported Number of Persons with Chronic HBV in MN As of December 31, 2013, 21,585* persons are assumed alive and living in MN with chronic HBV *Includes persons with unknown city of residence Note: Includes all chronic, and probable chronic cases. Data Source: MN Viral Hepatitis Surveillance System

78
Persons Living with HBV in MN by Current Residence, 2013 Metro = Seven-county metro area including Anoka, Carver, Dakota, Hennepin, Ramsey, Scott, and Washington counties. Greater MN = All other Minnesota counties, outside the seven-county metro area. Total number with residence information = 21,242 (343 missing residence information) Data Source: MN Viral Hepatitis Surveillance System
 Data Source: MN Viral Hepatitis Surveillance System.")
79
Persons with Chronic HBV in MN by Age, 2013 Median Age: 43 Data Source: MN Viral Hepatitis Surveillance System

80
Chronic HBV in MN by Gender, 2013 Data Source: MN Viral Hepatitis Surveillance System

81
Persons Living with Chronic HBV in Minnesota by Race, 2013 Persons with unknown race=3,365 Afr Amer = African American /Black Asian=Asian or Pacific Islander Amer Ind = American Indian Other = Multi-racial persons or persons with other race Data Source: MN Viral Hepatitis Surveillance System

82
Persons Living with Chronic HBV in Minnesota by Race rates (per 100,000 persons*), 2013 *Rates calculated using 2010 U.S. Census data Excludes 3,396 cases with multiple races and unknown race Data Source: MN Viral Hepatitis Surveillance System

83
Overview of HCV in Minnesota A hepatitis C case is defined as current or past infection with hepatitis C and includes: Acute cases: Infected within the last six months Symptomatic Chronic cases: Infected for over six months Resolved cases: No evidence of current infection Evidence of past infection

84
Reported Number of Persons Living with HCV in MN As of December 31, 2013, 40,943* persons are assumed alive and living in MN with HCV *Includes persons with unknown city of residence Note: Includes all acute, chronic, probable chronic, and resolved cases. Data Source: MN Viral Hepatitis Surveillance System

85
HCV Infected Persons Identified through Passive Surveillance in MN through 2013 **http://www.cdc.gov/ncidod/diseases/hepatitis/c/fact.htm *Includes all acute, chronic, probable chronic, and resolved cases. HCV infected persons* identified through passive surveillance Estimated unidentified HCV infected persons 40,943 43,920 N=84,863** Data Source: MN Viral Hepatitis Surveillance System

86
Persons Living with HCV in MN by Current Residence, 2013 Suburban = Seven-county metro area including Anoka, Carver, Dakota, Hennepin (except Minneapolis), Ramsey (except St. Paul), Scott, and Washington counties including those in Hennepin County or Ramsey County with unknown city. Greater MN = All other Minnesota counties, outside the seven-county metro area. Total number with residence information= 40,033 (1,271 missing residence information) Data Source: MN Viral Hepatitis Surveillance System
, Scott, and Washington counties including those in Hennepin County or Ramsey County with unknown city. Greater MN = All other Minnesota counties, outside the seven-county metro area. Total number with residence information= 40,033 (1,271 missing residence information) Data Source: MN Viral Hepatitis Surveillance System.")
87
Persons Living with HCV in MN by Age, 2013 Median Age: 56 Data Source: MN Viral Hepatitis Surveillance System

88
*Includes anonymous methadone patients Persons Living with HCV in MN by Gender*, 2013 Data Source: MN Viral Hepatitis Surveillance System

89
Persons Living with Chronic HCV in Minnesota by Race, 2013 Afr Amer = African American /Black Asian=Asian or Pacific Islander Amer Ind = American Indian Other = Multi-racial persons or persons with other race

90
Persons Living with HCV in Minnesota rates (per 100,000 persons*), 2013 *Rates calculated using 2010 U.S. Census data Excludes persons with multiple races or unknown race Data Source: MN Viral Hepatitis Surveillance System

91
Hepatitis C in Populations of Interest

92
Hepatitis C in young adults under age 30

93
Data Source: Minnesota Viral Hepatitis Surveillance System Reported Number of Persons <30 Living with HCV in MN As of December 31, 2013, 1,764* persons under the age of 30 are assumed alive and living in MN with HCV *Includes persons with unknown city of residence Note: Includes all acute, chronic, probable chronic, and resolved cases.

94
Data Source: Minnesota Viral Hepatitis Surveillance System Persons <30 Living with HCV in MN by Current Residence, 2013 Suburban = Seven-county metro area including Anoka, Carver, Dakota, Hennepin (except Minneapolis), Ramsey (except St. Paul), Scott, and Washington counties including those in Hennepin County or Ramsey County with unknown city. Greater MN = All other Minnesota counties, outside the seven-county metro area. Total number with residence information= 1,745 MN Overall MN Age Under 30 years Total number with residence information= 40,333
, Scott, and Washington counties including those in Hennepin County or Ramsey County with unknown city. Greater MN = All other Minnesota counties, outside the seven-county metro area. Total number with residence information= 1,745 MN Overall MN Age Under 30 years Total number with residence information= 40,333.")
95
Data Source: Minnesota Viral Hepatitis Surveillance System *Includes anonymous methadone patients Persons <30 Living with HCV in MN by Gender*, 2013 MN Overall MN Age Under 30 years

96
Data Source: Minnesota Viral Hepatitis Surveillance System Persons <30 Living with HCV in MN by Race, 2013 Suburban = Seven-county metro area including Anoka, Carver, Dakota, Hennepin (except Minneapolis), Ramsey (except St. Paul), Scott, and Washington counties including those in Hennepin County or Ramsey County with unknown city. Greater MN = All other Minnesota counties, outside the seven-county metro area. MN Overall MN Age Under 30 years
, Scott, and Washington counties including those in Hennepin County or Ramsey County with unknown city. Greater MN = All other Minnesota counties, outside the seven-county metro area. MN Overall MN Age Under 30 years.")
97
Hepatitis C in American Indians

98
Data Source: Minnesota Viral Hepatitis Surveillance System Reported Number of American Indian Persons Living with HCV in MN As of December 31, 2013, 2,073 * persons who identify as American Indian are assumed alive and living in MN with HCV *Includes persons with unknown city of residence Note: Includes all acute, chronic, probable chronic, and resolved cases.

99
Data Source: Minnesota Viral Hepatitis Surveillance System American Indian Persons Living with HCV in MN by Current Residence, 2013 Suburban = Seven-county metro area including Anoka, Carver, Dakota, Hennepin (except Minneapolis), Ramsey (except St. Paul), Scott, and Washington counties including those in Hennepin County or Ramsey County with unknown city. Greater MN = All other Minnesota counties, outside the seven-county metro area. Total number with residence information= 2,058 MN Overall MN American Indian Total number with residence information= 40,333
, Scott, and Washington counties including those in Hennepin County or Ramsey County with unknown city. Greater MN = All other Minnesota counties, outside the seven-county metro area. Total number with residence information= 2,058 MN Overall MN American Indian Total number with residence information= 40,333.")
100
Data Source: Minnesota Viral Hepatitis Surveillance System American Indian Persons Living with HCV in MN by Age, 2013 Median Age: 51

101
Data Source: Minnesota Viral Hepatitis Surveillance System *Includes anonymous methadone patients Persons Living HCV in MN by Gender*, 2013 MN Overall MN American Indian

102
Hepatitis C Treatment

103
Hepatitis C Treatment Changes Direct acting antiviral agents approved in the U.S. Improved rates of sustained virologic response Rapidly changing recommendations hcvguidelines.org

104
Thank you! For more information please contact: Kristin Sweet 651.201.4888 kristin.sweet@state.mn.us

105
QUESTIONS? Jessica Brehmer, MPH, HIV Epidemiologist, MDH 651-201-5624, jessica.brehmer@state.mn.usjessica.brehmer@state.mn.us Sarah Gordon, MPH, Coordinator, HIV Testing and Syringe Services Programs, MDH 651-201-4011, sarah.gordon@state.mn.ussarah.gordon@state.mn.us Kristin Sweet, MPH, Hepatitis Epidemiologist, MDH 651-201-4888, kristin.sweet@state.mn.uskristin.sweet@state.mn.us

Similar presentations


























 Surveillance Report, 2010>")







 201-5414 Tuberculosis surveillance data for Minnesota are available on.>")








