Download presentation
Presentation is loading. Please wait.

1
Beware of Registries for their Biases Hasan Yazici University of Istanbul

2
Disclosures Pfizer (Turkey) – travel support & speaker’s fees Merck (Turkey) – travel support & speaker’s fees
 – travel support & speaker’s fees Merck (Turkey) – travel support & speaker’s fees")
3
Beware of Observational Studies based on Registries for their Biases Hasan Yazici University of Istanbul

4
Plan For and against observational studies Few historical notes A summary of important biases in observational studies based on registries and administrative data bases The bias of determining cancer incidence in registries - a recent example Some naive arithmetic What to do? In brief

5
Observational Studies Advantages Real life data Relatively cheap Potential to observe multiple outcomes Ability to assess cause – effect relations Long term observations

6
Observational Studies Problems Many are cross sectional or retrospective. Selection bias including completeness of recruitment Confounders Uniformity of assessment Control groups

7
RCTs vs Observational studies Efficacy : RCT superior Harm: Observational study superior Biomarkers: Observational study superior JP Vandenbroucke BMJ, 2011

8
RCTs vs Observational studies Efficacy : RCT superior ? Harm: Observational study superior Biomarkers: Observational study superior JP Vandenbroucke BMJ, 2011

11
The DES* Drama DES began to be used for threatened abortion (1949) Efficacy could not be shown in a double blind, placebo controlled study at University of Chicago (1958) An “epidemic” of vaginal cancer among girls in Boston (1971) Among 8 patients with vaginal cancer 7 were daughters of mothers who had used DES during pregnancy. This contrasted with mothers of 32 healthy girls (born in the same hospital within a day or two) among whom there were no DES users. * diethylstilbestrol
 among whom there were no DES users. * diethylstilbestrol.")
13
The DES* Drama DES began to be used for threatened abortion (1949) Efficacy could not be shown in a double blind, placebo controlled study at University of Chicago (1958) An “Epidemic” of vaginal cancer among girls in Boston (1971) Among 8 patients with vaginal cancer 7 were daughters of mothers who had used DES during pregnancy. This contrasted with mothers of 32 healthy girls (born in the same hospital within a day or two) among whom there were no DES users. FDA banned DES in pregnancy (1971). A study (Mayo Clinic) in mid 70’s among 800 young women with a mother who had used DES during pregnancy did not reveal any cases of vaginal cancer. No surprise. Since frequency of vaginal cancer: <1/1000 users. A further case control study from NY State Tumor Registry confirmed the association. * diethylstilbestrol
 among whom there were no DES users. FDA banned DES in pregnancy (1971). A study (Mayo Clinic) in mid 70’s among 800 young women with a mother who had used DES during pregnancy did not reveal any cases of vaginal cancer. No surprise. Since frequency of vaginal cancer: <1/1000 users. A further case control study from NY State Tumor Registry confirmed the association. * diethylstilbestrol.")
14
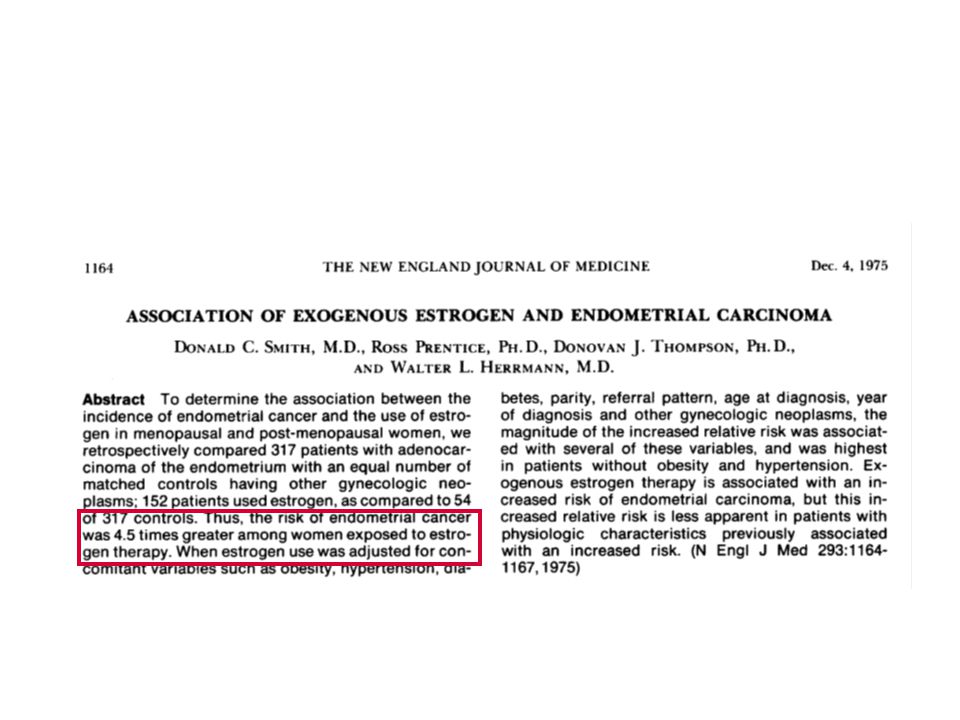
The Estrone Drama “Like a gallant knight (the author of Feminine Forever) has come to rescue his fair lady not at the time of her bloom and flowering but in her desparing years; at a time of life when the preservation and prolongation of her femaleness are so paramount…By throwing down his gauntlet, he challanges the reluctant physician to follow him in providing the hormones that may allow for a smoother transition to the menopausal years ahead. Women will be emancipated only when the shackles of hormonal deprevation are loosed.” in Investigating Disease Patterns, Stolley&Lasky, 1995

19
....I think this is rather misleading. Of the 26 lymphomas they refer to in the main text, 14 occurred within 2 months of TNF antagonist use. Thus, a more realistic comparator would be a deduced (from the annual rates) 2-month incidence of lymphoma in the general population.... H Yazici Arthritis Rheum 2003
 2-month incidence of lymphoma in the general population.... H Yazici Arthritis Rheum")
20
Time to Neoplasia Based on T Bongartz et al. JAMA 2006

21
The Wandering Comparison of Risk (Lymphoma) M. Hudson & S. Suissa Arthritis Care and Res, 2010
 M. Hudson & S. Suissa Arthritis Care and Res, 2010")
22
The Wandering Comparison of Risk (Lymphoma) M. Hudson & S. Suissa Arthritis Care and Res, 2010
 M. Hudson & S. Suissa Arthritis Care and Res, 2010")
24
The Wandering Comparison of Risk (Infections)
")
26
Channeling Bias (in an administrative data base)
")
29
The Immortal Time Bias..arises in a cohort study where an outcome can hinder, totally or partially, the realization of the exposure.

30
The Immortal Time Bias Hydroxychloroquine decreases cancer in SLE by 85% G. Ruiz Irastorza et al. Ann Rheum Dis, 2007 Statins decrease lung cancer by 45%. V. Khuarana et al. Chest, 2007 LE Levesque et al. Br Med J, 2010

32
References Eur Respir J (4) Arch Intern Med (2) Am J Med (2) Am J Respir Crit Care Med (2) Lancet (2) JAMA (1) Am J Respir Med (1) J Allergy Clinical Immunol (1) Ann Allergy Asthma Immunol (1) Thorax (1) Pediatrics (1) Ann Pharmacother (1) Diabet Med (1)
 Arch Intern Med (2) Am J Med (2) Am J Respir Crit Care Med (2) Lancet (2) JAMA (1) Am J Respir Med (1) J Allergy Clinical Immunol (1) Ann Allergy Asthma Immunol (1) Thorax (1) Pediatrics (1) Ann Pharmacother (1) Diabet Med (1)")
35
Misclassified Immortal Time The authors study a complete registry of SLE patients between 2 time points. The exposed group consists of patients who had ever used hydroxychlorquine. The non – exposed group consists of patients who have never used hydroxychloroquine. The authors find significantly less cancers in the “exposed = ever used” group.

36
OR for death = Odds of death in the exposed Odds of death in the non-exposed

38
What is wrong? In the numerator those patients who had died due to malignancy could not have been prescribed hydroxychloroqine. Thus the duration of follow up time that can lead to malignancy in the numerator is actually shorter and this decreases the odds for a malignancy in the numerator making it lower than what is said.

39
The RDPR Study We hypothesize that topical antifungals (TA) decrease mortality. In the Registryville Drug Prescriptions Registry (RDPR) between January 1, 2009 and ending on March 31st, 2009 we identify 1000 patients with an ever prescription for TA. We follow all patients fom the time of prescription to December 31st 2010, for emerging death. We use the RMR (Registryville Mortality Registry) to confirm the deaths. From RDPR we also randomize a 1000 sample of age, gender and practically everything else matched individuals AND also follow them for the same outcome up to December 31st. 2010. Exposed group: patients with a prescription for a TA Non- exposed group: patients with other prescriptions Outcome: death
 between January 1, 2009 and ending on March 31st, 2009 we identify 1000 patients with an ever prescription for TA. We follow all patients fom the time of prescription to December 31st 2010, for emerging death. We use the RMR (Registryville Mortality Registry) to confirm the deaths. From RDPR we also randomize a 1000 sample of age, gender and practically everything else matched individuals AND also follow them for the same outcome up to December 31st Exposed group: patients with a prescription for a TA Non- exposed group: patients with other prescriptions Outcome: death.")
40
The RDPR Study At the end of the study we compare: OR (exposed)/OR (non-exposed) 30 people (30/732 pt. yrs.) in the exposed group; 60 people (60/950 pt. yrs.) in the non- exposed group have dies. TA significantly lessens mortality OR=0.50; p= 0.009
 in the exposed group; 60 people (60/950 pt. yrs.) in the non- exposed group have dies. TA significantly lessens mortality OR=0.50; p=")
41
Excluded Immortal Time We correctly exclude from the numerator the follow up of those patients before they were prescribed the exposure drug. This is the immortal time and, again, deaths can only happen after the exposure (the prescription).
..")
42
Excluded Immortal Time We correctly exclude from the numerator the follow up of those patients before they were prescribed the exposure drug. This is the immortal time and, again, deaths can only happen after the exposure (the prescription). However this is not enough. This time period should be added to the denominator.
. However this is not enough. This time period should be added to the denominator..")
43
Exposed

44
Entry

45
Exposed Calendar Age Birth date Disease onset Diagnosis Registration in a clinic Registration in a database Entry

46
Exposed Calendar Age Birth date Disease onset Diagnosis Registration in a clinic Registration in a database Entry Exposure ie prescription

47
Exposed Calendar Age Birth date Disease onset Diagnosis Registration in a clinic Registration in a database Entry Exposure ie prescription Observation ends

48
Exposed Unexposed Calendar Age Birth date Disease onset Diagnosis Registration in a clinic Registration in a database Entry Exposure ie prescription Observation ends

49
Exposed Unexposed Calendar Age Birth date Disease onset Diagnosis Registration in a clinic Registration in a database Entry Exposure ie prescription Observation ends Entry Observation ends

50
Exposed Unexposed Calendar Age Birth date Disease onset Diagnosis Registration in a clinic Registration in a database Entry Exposure ie prescription Observation ends immortal time Entry Observation ends

51
Exposed Unexposed Calendar Age Birth date Disease onset Diagnosis Registration in a clinic Registration in a database Entry Exposure ie prescription Observation ends immortal time Entry Observation ends

52
Exposed Unexposed Calendar Age Birth date Disease onset Diagnosis Registration in a clinic Registration in a database Entry Exposure ie prescription Observation ends immortal time Entry Observation should end

53
Exposed Unexposed Calendar Age Birth date Disease onset Diagnosis Registration in a clinic Registration in a database Entry Exposure ie prescription Observation ends immortal time Entry Observation should end outcome free!

54
Remedy (s) There might be none especially when we are unclear about the entry, hence the observation time. Always include the “immortal time” to the duration of follow up in the non-exposed.

55
The RDPR Study At the end of the study we compare: OR (exposed)/OR (non-exposed) 30 people (30/732 pt. yrs.) in the exposed group; 60 people (60/950 pt. yrs.) in the non- exposed group have died. TA significantly lessens mortality OR=0.50; p= 0.009
 in the exposed group; 60 people (60/950 pt. yrs.) in the non- exposed group have died. TA significantly lessens mortality OR=0.50; p=")
56
The RDPR Study At the end of the study we compare: OR (exposed)/OR (non-exposed) 30 people (30/732 pt. yrs.) in the exposed group; 60 people (60/ 1200 pt. yrs.) in the non- exposed group have died. TA does nothing to the mortality, OR=0.98
 in the exposed group; 60 people (60/ 1200 pt. yrs.) in the non- exposed group have died. TA does nothing to the mortality, OR=0.98.")
57
S Suissa Pharmacoepidemiol Drug Saf, 2007

58
… which includes adding the immortal time to the none- exposed arms in either type of immortal time bias - HY

62
H Yazici et al Arthritis Rheum, 2011

63
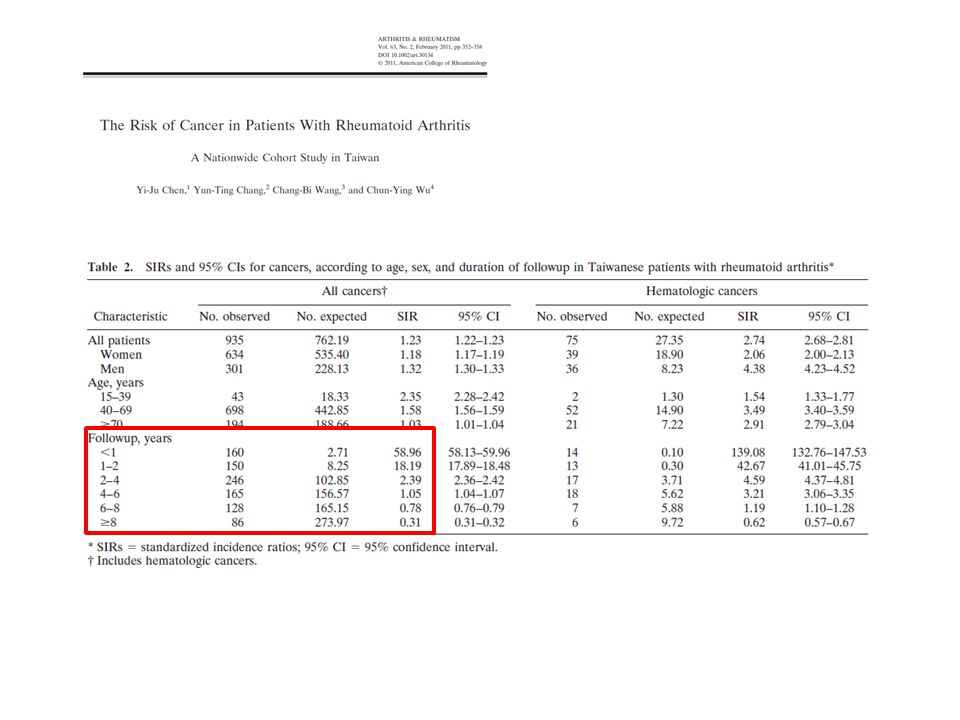
A Possible Source of Error in the Method of Cancer Risk Estimation in Patients with Rheumatoid Arthritis We surveyed the PubMed between years 2001- 2011 Search terms “registry” “cancer” “rheumatoid arthritis” Papers that reported comparative incidence in at least 2 time points were included Change over time was assessed H Yazici et al. ACR, 2011

64
A Possible Source of Error in the Method of Cancer Risk Estimation in Patients with Rheumatoid Arthritis 1274 articles 36 articles retrieved 6 reported incidence comparison at multiple timepoints The last SIR was less than the initial by 40 to 99% H Yazici et al. ACR, 2011

65
A Possible Source of Error in the Method of Cancer Risk Estimation in Patients with Rheumatoid Arthritis H Yazici et al. ACR, 2011 * initial year excluded

66
Some naive arithmetic

67
Cumulative Cancer Prevalence in a Hypothetical RA Registry of Incident Cases of RA Given: There are no biologic associations between RA and cancer Incidence of RA: 1/1000/year Incidence of cancer: 5/1000/year These incidences remain same over time. 1000 new cases of RA enter the registry every year. 2/5 of all cancer patients die at the end 1 year. Of the 2/5 who die 1 dies before and the other dies after developing RA. Another 1/10 of the cancer patients die, in a logarithmically decreasing fashion, at the end of 5 years. * RA does not kill if not associated with cancer. All other causes of death are ignored. * This group is ignored for the purposes of this presentation. Its inclusion would only support our hypothesis.

68
Cumulative Cancer Prevalence in a Hypothetical RA Registry of Incident Cases of RA 1. year: Expected: 5/1000

69
Cumulative Cancer Prevalence in a Hypothetical RA Registry of Incident Cases of RA 1. year: Expected: 5/1000 Observed: 4/1000

70
Cumulative Cancer Prevalence in a Hypothetical RA Registry of Incident Cases of RA 1. year: Expected: 5/1000 Observed: 4/1000 1/5 cancer patients die before having the chance to develop RA.

71
Cumulative Cancer Prevalence in a Hypothetical RA Registry of Incident Cases of RA 1. year: Expected: 5/1000 Observed: 4/1000 O/E: 0.80 1/5 cancer patients die before having the chance to develop RA.

72
Cumulative Cancer Prevalence in a Hypothetical RA Registry of Incident Cases of RA 1. year: Expected: 5/1000 Observed: 4/1000 O/E: 0.80 2. year: Expected: 15/2000 1/5 cancer patients die before having the chance to develop RA.

73
Cumulative Cancer Prevalence in a Hypothetical RA Registry of Incident Cases of RA 1. year: Expected: 5/1000 Observed: 4/1000 O/E: 0.80 2. year: Expected: 15/2000 1/5 cancer patients die before having the chance to develop RA. 5 cancer patients are from the 1.year & 10 from the 2. year, from the total of 2000 patients

74
Cumulative Cancer Prevalence in a Hypothetical RA Registry of Incident Cases of RA 1. year: Expected: 5/1000 Observed: 4/1000 O/E: 0.80 2. year: Expected: 15/2000 Observed: 11/2000 1/5 cancer patients die before having the chance to develop RA. 5 cancer patients are from the 1.year & 10 from the total of 2000 patients

75
Cumulative Cancer Prevalence in a Hypothetical RA Registry of Incident Cases of RA 1. year: Expected: 5/1000 Observed: 4/1000 O/E: 0.80 2. year: Expected: 15/2000 Observed: 11/2000 1/5 cancer patients die before having the chance to develop RA. 5 cancer patients are from the 1.year & 10 from the total of 2000 patients 3 cancer patients cases are from the 1. year. We expect 10 incident cancer cases in the 2. year. 2/10 of these die before they get the chance to develop RA. The remaining 8 new cases plus the 3 from the 1. year make up 11 prevalent cases at the end of 2 years.

76
Cumulative Cancer Prevalence in a Hypothetical RA Registry of Incident Cases of RA 1. year: Expected: 5/1000 Observed: 4/1000 O/E: 0.80 2. year: Expected: 15/2000 Observed: 11/2000 O/E: 0.73 1/5 cancer patients die before having the chance to develop RA. 5 prevalent cases are from the 1.year & 10 from the total of 2000 patients 3 cancer patients cases are from the 1. year. We expect 10 incident cancer cases in the 2. year. 2/10 of these die before they get the chance to develop RA. The remaining 8 new cases plus the 3 from the 1. year make up 11 prevalent cases at the end of 2 years.

77
Cumulative Cancer Prevalence in a Hypothetical RA Registry of Incident Cases of RA 1. year: Expected: 5/1000 Observed: 4/1000 O/E: 0.80 2. year: Expected: 15/2000 Observed: 11/2000 O/E: 0.73 3. year: Expected: 30/2000 1/5 cancer patients die before having the chance to develop RA. 5 cancer patients cases are from the 1.year & 10 from the total of 2000 patients 3 cancer patients cases are from the 1. year. We expect 10 incident cancer cases in the 2. year. 2/10 of these die before they get the chance to develop RA. The remaining 8 new cases plus the 3 from the 1. year make up 11 prevalent cases at the end of 2 years.

78
Cumulative Cancer Prevalence in a Hypothetical RA Registry of Incident Cases of RA 1. year: Expected: 5/1000 Observed: 4/1000 O/E: 0.80 2. year: Expected: 15/2000 Observed: 11/2000 O/E: 0.73 3. year: Expected: 30/2000 Observed: 15/3000 1/5 cancer patients die before having the chance to develop RA. 5 cancer patients are from the 1.year & 10 from the total of 2000 patients 3 cancer patients cases are from the 1. year. We expect 10 incident cancer cases in the 2. year. 2/10 of these die before they get the chance to develop RA. The remaining 8 new cases plus the 3 from the 1. year make up 11 prevalent cases at the end of 2 years.

79
Cumulative Cancer Prevalence in a Hypothetical RA Registry of Incident Cases of RA 1. year: Expected: 5/1000 Observed: 4/1000 O/E: 0.80 2. year: Expected: 15/2000 Observed: 11/2000 O/E: 0.73 3. year: Expected: 30/2000 Observed: 15/3000 O/E: 0.50 1/5 cancer patients die before having the chance to develop RA. 5 cancer patients are from the 1.year & 10 from the total of 2000 patients 3 cancer patients are from the 1. year. We expect 10 incident cancer cases in the 2. year. 2/10 of these die before they get the chance to develop RA. The remaining 8 new cases plus the 3 from the 1. year make up 11 prevalent cases at the end of 2 years.

80
What to do? Be careful when comparing the frequency of a condition in a registry with the frequency of the same condition in the population from which that registry comes from; because of the selection bias. Give more importance to comparing like with like- attention to observation times, propensity scoring etc. Also give importance to comparing like with alike as we try to falcify our hypothesis – control groups with other diseases/conditions Proper case control studies starting from the hypothesized outcome – i.e looking for RA among neoplasms

81
CR Meier et al. JAMA, 2000

83
In brief Caveat lector !

85
In brief Caveat lector ! “Aye, there is the rub !”

86
In brief Caveat lector ! “Aye, there is the rub!” Do not go for a grand slam with 10 points at hand !

Similar presentations




























. What is a cohort?>")







