Download presentation
Presentation is loading. Please wait.

1
April 2010 UTILIZATION REVIEW HOW TO GET PAID (CORRECTLY) FOR PROVIDING CARE AND SERVICE
 FOR PROVIDING CARE AND SERVICE")
2
April 2010 OVERVIEW UR Plan Tasks Patient Status Patient Rights Notices Tools References

3
April 2010 PLAN Committee Scope and frequency of review Staffing Criteria Determinations regarding admissions or continued stays Extended stay review Performance improvement

4
April 2010 TASKS Observation Payer source UR line Criteria Length of stay Quality CMS measures Present on admission Hospital-acquired infections

5
April 2010 OBSERVATION Observation care is a well-defined set of specific, clinically appropriate services, which include ongoing short term treatment, assessment, and reassessment before a decision can be made regarding whether patients will require further treatment as hospital inpatients or if they are able to be discharged from the hospital. Postop amb surg: 4-6 hours of recovery, unplanned outcome or exacerbation of a condition; other wise extended recovery

6
April 2010 INPATIENT The physician is responsible for deciding whether the patient should be admitted as an inpatient; should use a 24-hour period as a benchmark; requires complex medical judgment and consideration of a number of factors Severity of illness and intensity of service Benefit period: 60F + 30C > 60O (+ 60L)
")
7
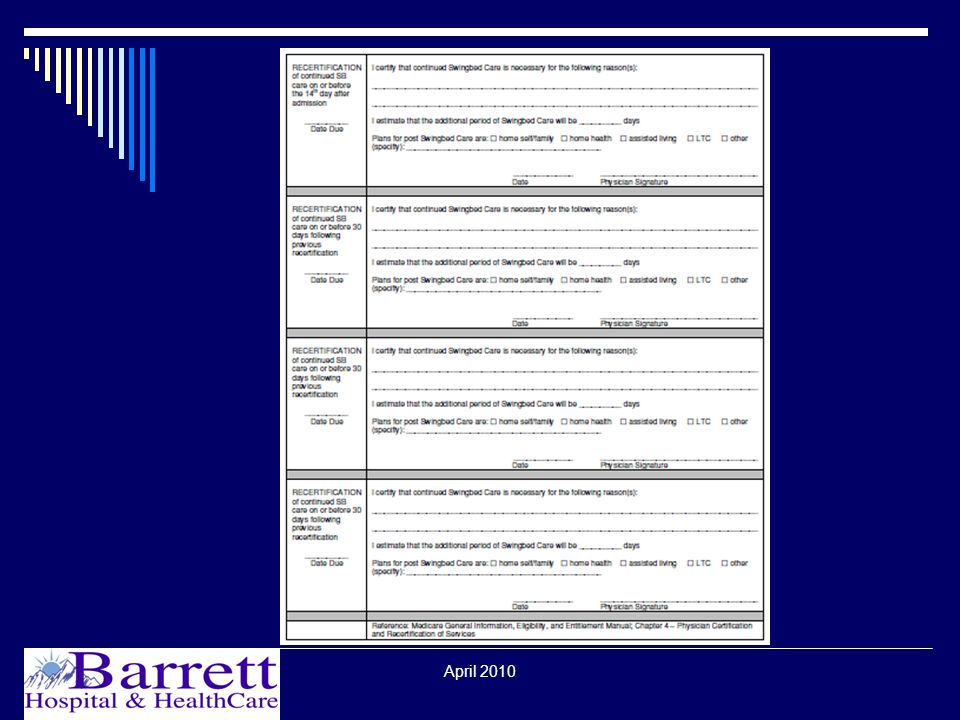
April 2010 SWING BED 3 day qualifying stay 30 day window Benefit period: 20F +80C > 60O Physician certification on admission Recertification day 14, day 44, day 74 Related condition, daily skilled need, inpatient setting, reasonable & necessary

8
April 2010 SWING BED – examples of skilled services Nursing Management & evaluation of a patient care plan – require the involvement of skilled personnel to meet patient needs Observation & assessment of patient’s condition – when there is a likelihood of change in patient condition Teaching & training activities – injections, new diabetic, care of dressings or skin treatments, care for central lines, self-catheterization, colostomy care, gastrostomy feedings, prosthesis care Direct skilled nursing – IV therapy, Stage 3 or > pressure ulcer treatments, dressings involving aseptic technique Therapy Based on eval by qualified PT; require judgment, knowledge, skills of PT; potential for patient improvement over reasonable period of time; specific & effective for patient condition; reasonable & necessary amount, frequency, & duration Examples: Assessment, therapeutic exercises, gait training, range of motion, maintenance therapy, Ultrasound, shortwave, and microwave diathermy treatments, Hot packs, Infra-Red Treatments, Paraffin Baths, and Whirlpool Baths, Speech-Language Pathology, Occupational Therapy

9
April 2010 SWING BED – Medicaid If MA is primary or secondary, prior authorization is required Must transfer to NH unless no skilled NH bed available within 25 miles OR physician may request waiver in writing if: Transfer would endanger patient OR Life expectancy is 6 months or less Level of Care & Level I forms to MPQH Waiver request to Senior & LTC Division

10
April 2010 MEDICAID – Mental Health Verify MA eligibility (Mental Health Access Program does not cover – 72 hr presumptive eligibility program available if no pay source) Notify First Health Services (https://montana.fhsc.com) – prior authorization request form within 1 business dayhttps://montana.fhsc.com Under age 21: Certificate of Need within 14 days Discharge form within 5 business days after discharge
 Notify First Health Services ( – prior authorization request form within 1 business dayhttps://montana.fhsc.com Under age 21: Certificate of Need within 14 days Discharge form within 5 business days after discharge")
11
April 2010 MEDICAID – Alcohol & Drug Detox Limited to 4 days unless necessary adjunct to treatment of a concomitant condition Obtain authorization by contacting DPHHS RN Case Manager

12
April 2010 COMMERCIAL PAYERS “Swing Bed” rates can be negotiated with some commercial payers Patient’s policy needs to cover skilled care services No prior authorization is required in connection with childbirth for a mother and her newborn; 48 hour postpartum vaginal delivery; 96 hour postpartum c- section

13
April 2010 INPATIENT HOSPICE Respite Care - short-term inpatient care to relieve caregivers at home - only on an occasional basis - no more than 5 consecutive days at a time General Inpatient Care – may be required for procedures necessary for pain control or acute or chronic symptom management that cannot feasibly be provided in other settings

14
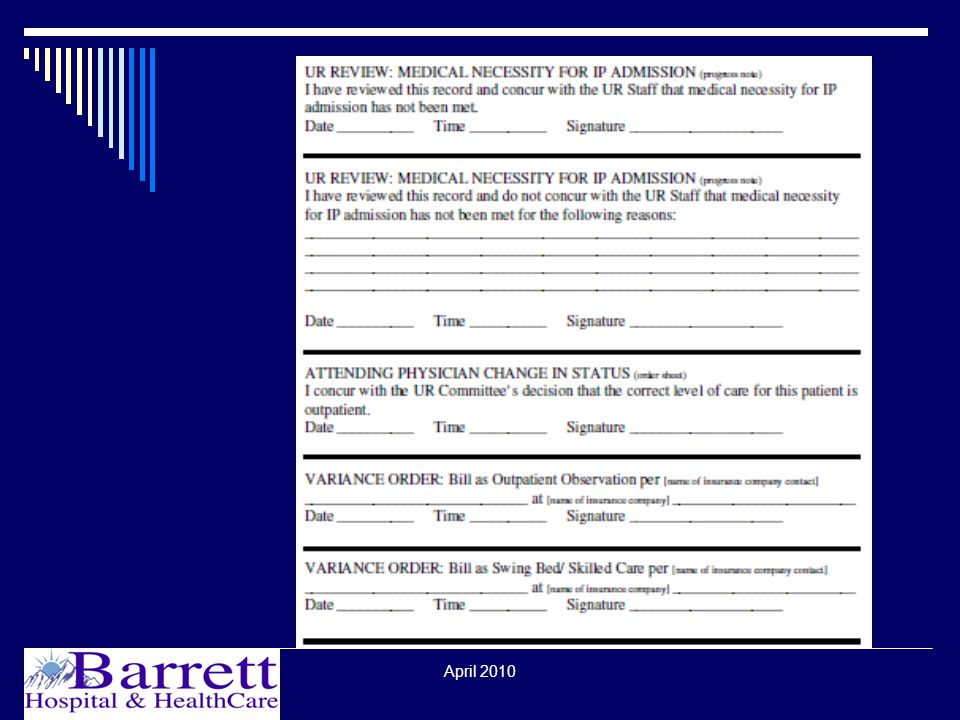
April 2010 CHANGING PATIENT STATUS IP to Observation Medicare: prior to discharge, no claim submitted, physician concurs, concurrence is documented Can only bill from the time the observation orders are written (condition code 44) Must notify patient Commercial: variance order Observation to IP Precertification required for commercial IP stay
 Must notify patient Commercial: variance order Observation to IP Precertification required for commercial IP stay")
15
April 2010 MEDICARE DISCHARGE APPEAL RIGHTS “Important Message from Medicare” Within 2 days of admission AND discharge Signed original to patient, copy to record May use same notice for initials at discharge “Detailed Notice of Discharge” Deliver to patient no later than noon of the day after the QIO notification to the hospital

16
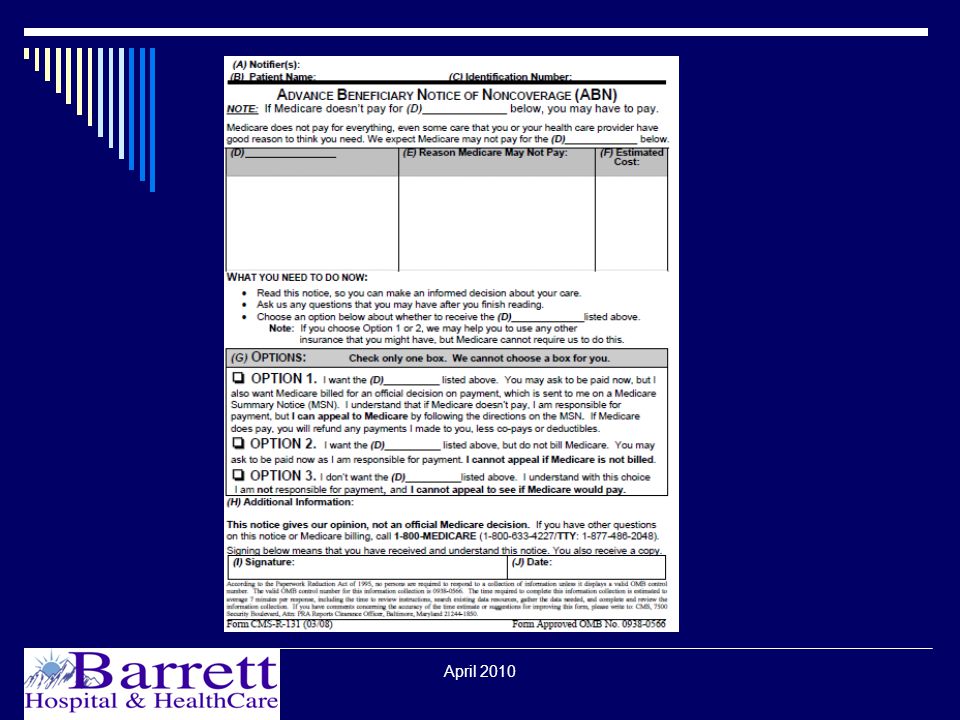
April 2010 MEDICARE NOTICES OBSERVATION When otherwise covered services will be noncovered If services will no longer be reasonable or necessary ABN (Advanced Beneficiary Notice) given prior to service
 given prior to service")
17
April 2010 MEDICARE NOTICES INPATIENT Given when care not medically necessary, not delivered in the most appropriate setting, or is custodial in nature HINN 1 (preadmission/ admission) HINN 10 (Hospital Requested Review – HRR) without physician concurrence HINN 11 (non-covered items or services during an otherwise covered stay) HINN 12 (non-covered continued stay)
 HINN 10 (Hospital Requested Review – HRR) without physician concurrence HINN 11 (non-covered items or services during an otherwise covered stay) HINN 12 (non-covered continued stay)")
18
April 2010 MEDICARE NOTICES SWING BED “Notice of Medicare Provider Non-Coverage” – at least 2 days prior to discharge “Detailed Explanation of Non-Coverage” – when QIO review is requested Notice of Exclusions from Medicare Benefits (no qualifying 3 day hospital stay, no days left in benefit period, daily skilled care requirements not met) – HINN or NEMB?
 – HINN or NEMB")
19
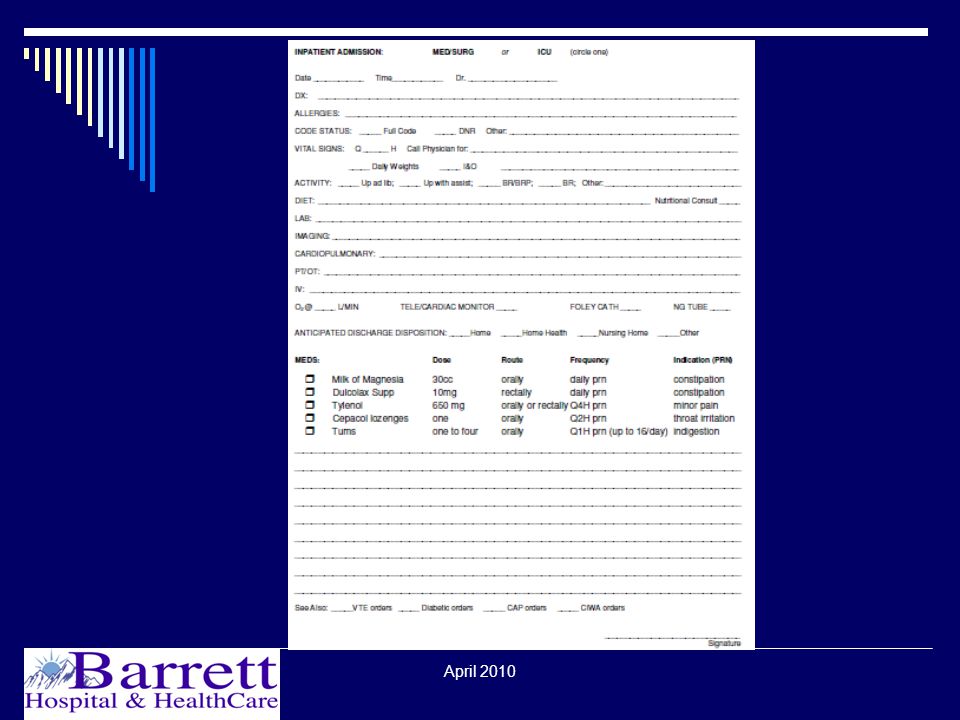
April 2010 DOCUMENTATION - provider Physician: take care of patients and document well Documentation requirements: OP Treatment: Dx, Tx OP Procedure: if pt not ready after 6 hrs routine recovery, order extended recovery or Observation (or IP) Observation: Reason for observation, tests, txs, monitoring parameters, decision point (intervene -> assess -> discharge or IP or intervene -> etc) IP: severity of illness, intensity of service SB: response to skilled care Hospice Acute: pain and symptom control
 Observation: Reason for observation, tests, txs, monitoring parameters, decision point (intervene -> assess -> discharge or IP or intervene -> etc) IP: severity of illness, intensity of service SB: response to skilled care Hospice Acute: pain and symptom control")
20
April 2010 DOCUMENTATION - nurse Nurse: take care of patients and document well Documentation requirements: OP Treatment: patient care and responses OP Procedure: if pt not ready after 6 hrs routine recovery, get order for extended recovery or Observation (or IP) Observation: tests, txs, patient response, communication with physician IP: severity of illness, intensity of service SB: response to skilled care Hospice Acute: pain and symptom control
 Observation: tests, txs, patient response, communication with physician IP: severity of illness, intensity of service SB: response to skilled care Hospice Acute: pain and symptom control")
21
April 2010

37
REFERENCES 42CFR § 482.30 Medicare Conditions of Participation Standards for Hospital Utilization Review http://edocket.access.gpo.gov/cfr_2004/octqtr/pdf/42cfr482.3 0.pdf Medicare Benefit Policy Manual, Chapter 1 - Inpatient Hospital Services Covered Under Part A http://www.cms.hhs.gov/manuals/Downloads/bp102c01.pdf Medicare General Information, Eligibility, and Entitlement, Chapter 4 - Physician Certification and Recertification of Services http://www.cms.hhs.gov/manuals/downloads/ge101c04.pdf

38
April 2010 REFERENCES Medicare Benefit Policy Manual, Chapter 6 - Hospital Services Covered Under Part B http://www.cms.hhs.gov/manuals/Downloads/bp102c06.pdf Medicare Benefit Policy Manual, Chapter 3 - Duration of Covered Inpatient Services http://www.cms.hhs.gov/manuals/Downloads/bp102c03.pdf Medicare Benefit Policy Manual, Chapter 8 - Coverage of Extended Care (SNF/SB) Services Under Hospital Insurance http://www.cms.hhs.gov/manuals/Downloads/bp102c08.pdf
 Services Under Hospital Insurance")
39
April 2010 REFERENCES Medicare General Information, Eligibility, and Entitlement, Chapter 3 - Deductibles, Coinsurance Amounts, and Payment Limitations http://www.cms.hhs.gov/manuals/downloads/ge101c03.pdf ARMs 37.40.4 Swing Beds http://www.mtrules.org/gateway/Subchapterhome.asp?scn= 37%2E40%2E4 Montana Medicaid http://www.dphhs.mt.gov/programsservices/medicaid.shtml

40
April 2010 REFERENCES ARMs 37.88.11 : Medicaid Mental Health Services: Inpatient Psychiatric Services http://www.mtrules.org/gateway/ChapterHome.asp?Chapter =37%2E88 ARMs 37.86.29 Medicaid Primary Care Services: Inpatient Hospital Services http://www.mtrules.org/gateway/Subchapterhome.asp?scn= 37%2E86.29 FHSC Montana Adult Acute Inpatient Provider Manual, Version 2.1, December 1, 2008 https://montana.fhsc.com/Downloads/Adult/manuals/MT_A_ Acute_ProviderManual_2_1-20090506.pdf

41
April 2010 REFERENCES Newborns’ and Mothers’ Health Protection Act http://www.dol.gov/federalregister/HtmlDisplay.aspx?DocId= 21637&AgencyId=8 Medicare Benefit Policy Manual, Chapter 9 - Coverage of Hospice Services Under Hospital Insurance http://www.cms.hhs.gov/manuals/Downloads/bp102c09.pdf Medicare Claims Processing Manual, Chapter 30 - Financial Liability Protections http://www.cms.hhs.gov/manuals/downloads/clm104c30.pdf

42
April 2010 REFERENCES CMS Home > Medicare > Beneficiary Notices Initiative (BNI) > Hospital Discharge Appeal Notices http://www.cms.hhs.gov/BNI/12_HospitalDischargeAppealN otices.asp#TopOfPage CMS Home > Medicare > Beneficiary Notices Initiative (BNI) > Overview http://www.cms.hhs.gov/bni/ CMS Home > Medicare > Beneficiary Notices Initiative (BNI) > FFS Revised ABN http://www.cms.hhs.gov/BNI/02_ABN.asp#TopOfPage
 > Hospital Discharge Appeal Notices otices.asp#TopOfPage CMS Home > Medicare > Beneficiary Notices Initiative (BNI) > Overview CMS Home > Medicare > Beneficiary Notices Initiative (BNI) > FFS Revised ABN")
43
April 2010 REFERENCES CMS Home > Medicare > Beneficiary Notices Initiative (BNI) > FFS HINNs http://www.cms.hhs.gov/BNI/05_HINNs.asp CMS Home > Medicare > Beneficiary Notices Initiative (BNI) > FFS ED Notices http://www.cms.hhs.gov/BNI/06_FFSEDNotices.asp#TopOf Page CMS Home > Medicare > Beneficiary Notices Initiative (BNI) > FFS NEMB SNF http://www.cms.gov/BNI/13_FFS%20NEMB%20SNF.asp#T opOfPage
 > FFS HINNs CMS Home > Medicare > Beneficiary Notices Initiative (BNI) > FFS ED Notices Page CMS Home > Medicare > Beneficiary Notices Initiative (BNI) > FFS NEMB SNF opOfPage")
Similar presentations
















 Changes Iowa Medicaid Enterprise October 14, 2008.>")

 Why Would I Ever Need LTC?>")
>")

 3 Admission Coordinators.>")



 Project PO Webinar July 9, 2014 Part Two – New CMS Chronic Care Code Update 1.>")
 entitles eligible employees to take twelve weeks of unpaid, job protected leave.>")

