Download presentation
Presentation is loading. Please wait.

1
Where Innovation Is Tradition Academic Medicine and Health Reform: InSync or Tissue Rejection? Len M. Nichols, Ph.D., Professor and Director Center for Health Policy Research and Ethics College of Health and Human Services OU Medicine’s Leadership Development Institute Oklahoma City, OK July 19, 2013

2
Where Innovation Is Tradition Overview Key Linkages The Fragile Promise of System Reform Where We Are Now The Race Against Time Special Circumstances of Medical Education The Collaboration and Competition We Need 2

3
Linkages Values Health System Economy 3

4
Family Premium / Median Income 4 Author’s calculations, treating average employer contribution as income

5
What is Reform REALLY About? Elevating population health, and stewardship Signaling that “Business As Usual” is over Changing obsolete business models Transparency Incentive Realignment 5

6
Where Innovation Is Tradition Incentive Alignment Is Multi-Dimensional Wellness & Cost Sharing Decision Support Payment Reform PatientEmployer/PayerClinicians Community

7
Where Innovation Is Tradition Cost Containment Theory of PPACA End profitability of risk selection Change insurance business model to value seeking Force transparency and margin limits on insurers Channel competition into socially productive areas Make FFS less attractive in Medicare Develop incentive structures that reward cost reduction, improve quality, and SPREAD 7

8
Where Innovation Is Tradition So we think we know what we want Condition specific, patient acuity adjusted, comprehensive payment, distributed among coordinated clinicians and providers IF we pull this off, win-win-win 8

9
Problem: There is no Scotty! 9

10
This Will Not All Be Smooth Sailing 10

11
Close Up of Not Smooth Sailing 11

12
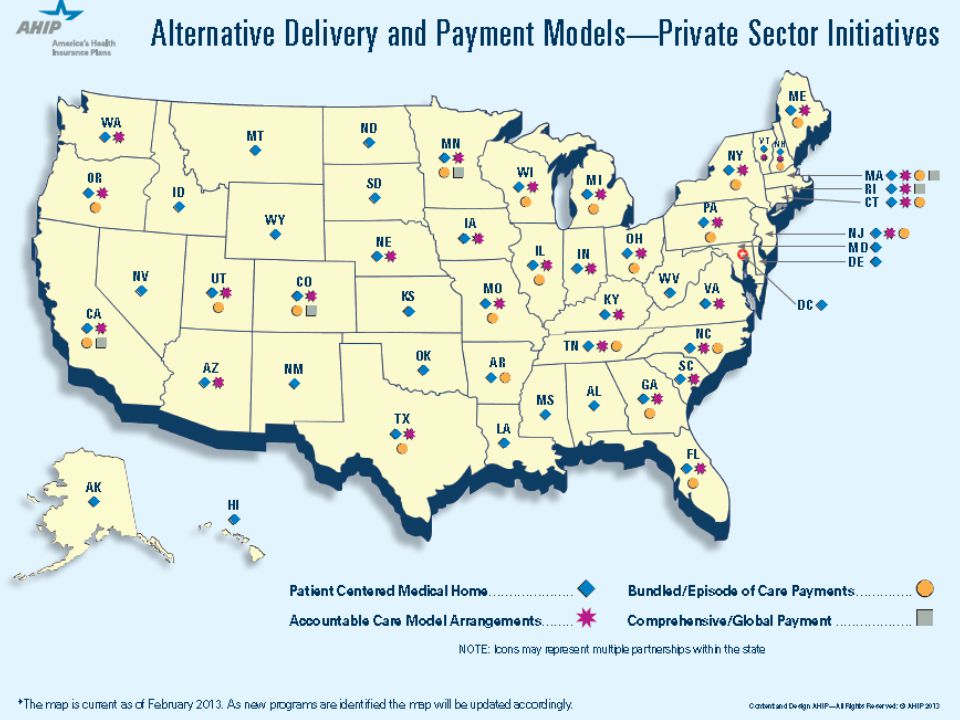
Where Innovation Is Tradition Where are we now? ACA “models” emerging in private sector, too 12

13
Innovation Center Portfolio ACO Suite: Shared Savings Program Pioneer ACO Model Advance Payment ACO Model Accelerated and Learning Development Sessions Primary Care Suite Comprehensive Primary Care Initiative (CPCI) Federally Qualified Health Center Advanced Primary Care Practice Demonstration Multi-Payer Advanced Primary Care Practice (MAPCP) Demonstration Independence at Home Medicaid Health Home State Plan Option Bundled Payment Suite Bundled Payment for Care Improvement Dual Eligible Suite: State Demonstration to Integrate care for Dual Eligible Individuals Financial Alignment to Support State Efforts to Integrate Care Demonstration to Reduce Avoidable Hospitalizations of Nursing Facility Residents Medicaid Health Home State Plan Option Diffusion and Scale Suite: Partnership for Patients Million Hearts Campaign Innovation Advisors Program Care Innovations Summit Healthcare Innovation Challenge Rapid Cycle Evaluation and Research Learning and Diffusion 14
 Federally Qualified Health Center Advanced Primary Care Practice Demonstration Multi-Payer Advanced Primary Care Practice (MAPCP) Demonstration Independence at Home Medicaid Health Home State Plan Option Bundled Payment Suite Bundled Payment for Care Improvement Dual Eligible Suite: State Demonstration to Integrate care for Dual Eligible Individuals Financial Alignment to Support State Efforts to Integrate Care Demonstration to Reduce Avoidable Hospitalizations of Nursing Facility Residents Medicaid Health Home State Plan Option Diffusion and Scale Suite: Partnership for Patients Million Hearts Campaign Innovation Advisors Program Care Innovations Summit Healthcare Innovation Challenge Rapid Cycle Evaluation and Research Learning and Diffusion 14")
15
Where Innovation Is Tradition Where are we now? ACA “models” emerging in private sector, too Fiscal pressures cannot be overstated 15

16
16 Allow US to Default ?

17
17

18
Where Innovation Is Tradition Where are we now? ACA “models” emerging in private sector, too Fiscal pressures cannot be overstated Insurance reform implementation “bumpy” 18

19
19

20
20 Scott Walker finds an alternative to Medicaid: Obamacare

21
21 Two states say 2014 Obamacare insurance costs on low side California Active Purchaser Premiums

22
22

23
Where are we now? ACA “models” emerging in private sector, too Fiscal pressures cannot be overstated Insurance implementation “bumpy” Health cost growth slowing 23

24
Where Innovation Is Tradition Total Health Spending Growth 24

25
Where Innovation Is Tradition Relative Health Spending Growth 25

26
The Race Against Time 26

27
Where Innovation Is Tradition The Budget World is Skeptical ACO takeup disappointing relative to hype CABG demo in 1990s not implemented PGP demo results mixed on cost ACE results not out yet AQC results promising; elsewhere…? PCMH evidence to date PCPCC vs. Mathematica Policy Research/AHRQ CMS data woes continue to plague participants 27

28
Two Roads to Fiscal Balance 28 CUTS RE-ALIGN INCENTIVES

29
Where Innovation Is Tradition So What are we really talking about? 29 $/N Time Healthier population Lower Use Lower Prices Higher quality Unsustainable cost growth 2012

30
Targets of Spending Reductions Poor care delivery Unnecessary services$210B8% of NHE Inefficient delivery$130B5% Missed prevention$ 55B2% Excessive Admin Costs$190B8% Prices$105B4% Fraud$ 73B3% TOTAL$765B 31% 30 D. Cutler, Senate Budget Testimony, citing IOM Expls. 1/2

31
31 Break

32
Where Innovation Is Tradition Un-Coordinated Care => Juicy Margins Care Transitions Poly-pharmacy management Integrating behavioral and acute care Managing those with multiple chronic conditions 32

33
High Prices => Juicy Margins Insurers GI+MCR + MLR and Admin simplification PhRMA Advamed Specialists and Hospitals Cardiology, orthopedics, radiology, etc. 33

34
Private Price Variation Large Physician prices vary 3:1 Hospital prices vary 6:1 34 MEDPAC 2011 analysis of 2008 Thompson-Reuters Market Scan Data.

35
35

36
36

37
Hospital Charge Variation 37 SOURCE: CMS MEDPAR charge data, 2011.

38
Where Innovation Is Tradition “Theory” of payment reform Changing the way we pay will so change behavior that total costs will fall AND SOME MDs (plus SOME hospitals) will gain* *(Compared to what? Which baseline?) AND this outcome will be sustained from new incentive structure When is this possible, and when not? 38
 AND this outcome will be sustained from new incentive structure When is this possible, and when not. 38.")
39
Where Innovation Is Tradition Sustainable Payment Reform Intervention Better Performance Savings cover cost of intervention 39 $$$

40
Pre-requisites for shared savings-based payment reform to work ALL must focus on Total Cost of Care Savings must more than cover intervention Payers must share some of the cost savings Cost could be foregone revenue Cost could be new services that must be added Current Baseline temporary reference point 40

41
Challenges Status Quo is very, very good to some Micro math ≠ macro math Reduced admissions => need fewer beds / pop More PC => need fewer specialists / pop We have less time than we’d like Total spend and total cost of care are only cost metrics that matter, only payers have “total” data AND financial + clinically relevant data are NOT linked for most providers and payers now Agreements on respective roles, shares not present 41

42
Roles Once Clear, Distinct PC SPEC H Plan 42

43
Roles Now Evolving, Melding PC SPEC H Plan 43

44
Where Innovation Is Tradition Fundamental Fact of Capitalism Risk bearors keep margins they can protect All others are wage / piece rate employees THEREFORE: your choices are: Earned shared savings, OR Declining FFS prices and/or declining covered access 44

45
Why transitions are possible but complex Actuarial expertise moves from insurers to providers Care coordination and financial alignment templates are public goods Education and research and last resort uncompensated care are public goods, too Who Is Willing to Pay for Them Today? 45

46
The Time Has Come… 46 "The time has come," the Walrus said, "To talk of many things: Of shoes—and ships—and sealing-wax— Of cabbages—and kings— And why the sea is boiling hot— And whether pigs have wings." —Through the Looking-Glass

47
47

48
48

49
Where Innovation Is Tradition The Time Has Come… Juicy Margins are hard to protect in transparent and competitive world Original BCBS community rating unraveled because employers refused to pay big margins on their workers, for-profit insurers arose, ERISA followed soon enough Cost-shift = high minded margin protection ME margins are particularly hard to protect 49

50
Why ME margins hard to protect Opaque so long => credibility gap High FPP and AHC prices hide noble goals Tertiary, experimental, uncompensated care Research Teaching Caught in larger public budget debate: Are these goals efficiently priced? Who should pay? Taxpayers or privately insured? Relative income realities 50

51
So What Is To Be Done? Get your accounting acts together PROVE your public goods’ value To yourselves To private payers To public financiers To local communities Build sustainable business models Expand awareness of TCC, value in communities Be ever mindful of local ability to pay Force rigorous “make or buy” ROI calculus 51

52
Where Innovation Is Tradition Deliver Value Care quality and care improvement (GWOS) TEACH care coordination in teams Science of care delivery + translational research may be as or more important than basic/clinical for next 10 years Develop and GIVE AWAY coordination protocols Develop and GIVE AWAY incentive contracts 52
 TEACH care coordination in teams Science of care delivery + translational research may be as or more important than basic/clinical for next 10 years Develop and GIVE AWAY coordination protocols Develop and GIVE AWAY incentive contracts 52")
53
Where Innovation Is Tradition ADD to your Mission Statement Stewardship (If you think this is not your problem, it will be, sooner) Consider sobering facts: Since 1960, US has seen 72 % growth in population 278% growth in N of MDs (4 x) 1,500% growth in clinical faculty (21 x) 53
 Consider sobering facts: Since 1960, US has seen 72 % growth in population 278% growth in N of MDs (4 x) 1,500% growth in clinical faculty (21 x) 53")
54
Where Innovation Is Tradition Every Stakeholder is Scared Insurers Drug and Device Companies Hospitals Specialists PCPs Nurses Software vendors 54

55
Where Innovation Is Tradition Scale of Coming Global Cap Cuts 55

56
Where Innovation Is Tradition Health Service Payment Modalities 56

57
Atavistic Competition is Always Possible 57

58
Where Innovation Is Tradition In general, when is Collaboration wise? When economies of scale from necessary investment are large relative to any one player When no one knows exactly how to improve When incentives have to be fundamentally changed to support necessary improvements When basic level of trust exists, or can be cobbled together and maintained with incentives and DATA 58

59
Where Innovation Is Tradition What do Clinicians Need for Collaboration to be Feasible ? DATA Technical assistance, learning pathways Templates for quality measurement, incentive contracts Risk-sharing partners, algorithms 59

60
Where Innovation Is Tradition If health plans won’t share data…. Convince employers to make them Convince consumers/legislators/exchanges to make them Explain to patients what’s at stake 60

61
Where Innovation Is Tradition Stuff to collaborate on Analytic database construction (HIE + APCD) Quality measures Payment STRUCTURE Diagnostic and treatment protocols Risk sharing contract parameters 61
 Quality measures Payment STRUCTURE Diagnostic and treatment protocols Risk sharing contract parameters 61")
62
Where Innovation Is Tradition Stuff to compete on Patient Experience and (risk adjusted) Outcomes Overall cost Quality execution Continuous learning 62
 Outcomes Overall cost Quality execution Continuous learning 62")
63
Where Innovation Is Tradition Equilibrium? Academic Medicine Public Goods Non-Mission Providers 63

64
Where Innovation Is Tradition What if we don’t share cost of Public Goods… We won’t get enough of them Arthur and the Vikings We WILL be sorry Too little research and uncompensated care The people will someday wonder why… 64

65
Where Innovation Is Tradition What if this all pay reform doesn’t work? Independent Payment Advisory Board (IPAB) Price controls Raise taxes Reduce coverage subsidies, repeal law 65
 Price controls Raise taxes Reduce coverage subsidies, repeal law 65.")
66
Hard Things I’m Asking You to Do Collaborate more to compete smarter Develop community-wide payment models Pursue stewardship, not just short-run self-interest Treat successful models as public goods Amend PPACA: malpractice reform and claims adjudication standardization, make Medicare partner Don’t forget why we’re asking you to do this Incentive realignment is only humane way to fiscal sanity 66

67
Where Innovation Is Tradition Stuff to Remember Patients trust you Plans need you Why you went to medical school 67

68
68

69
Where Innovation Is Tradition 69

70
70

Similar presentations













 Grants Chapter 6.>")





