Download presentation
Presentation is loading. Please wait.

1
BASIC PATHOLOGICAL ASPECTS OF NERVOUS SYSTEM PATHOLOGY
Esti D. S. Soetrisno B. Rino Pattiata Departement Anatomic Pathology Faculty of Medicine University of Indonesia

2
BASIC PATHOLOGICAL MANIFESTATION OF SOME DISTURBANCES
DYS – NEURO EMBRYOGENESIS ABORTION / INTRA-UTERINE FETAL DEATH (IUFD) ABNORMALITIES : TERATOGENIC, MONSTER, CONGENITAL ANOMALY AGENESIS : There is no processus (anlage) of all or partial part of NS No formation of NS IUFD APLASIA : There is only NS Streak Formation abortion HYPOPLASIA : Failure to growth of all or partial part of NS Hypotrophy (Micro Insize) Hypofunction / Fatal e.g Microensephaly, Arnold – Chiary Syndrome
 ABNORMALITIES : TERATOGENIC, MONSTER, CONGENITAL ANOMALY. AGENESIS : There is no processus (anlage) of all or partial part of NS. No formation of NS IUFD. APLASIA : There is only NS Streak Formation. abortion. HYPOPLASIA : Failure to growth of all or partial part of NS. Hypotrophy (Micro Insize) Hypofunction / Fatal. e.g Microensephaly, Arnold – Chiary Syndrome.")
3
Hyperplasia : Overgrowth parts of NS
e.g Macroensephaly, Hydrocephallus, Function? Hypertrophy: True Hypertrophy / Pseudo Hypertrophy Defect On Enclosing of the Neural Tube There is “Cele” Formation, or Spina Bifida Formation (Occulta/Aperta) e.g Meningocele, Encephalo -/ Myelo – Meningcocele, Syringo -Encephalo –/ Myelo – Meningcocele (Syringo Myelia)
 e.g Meningocele, Encephalo -/ Myelo – Meningcocele, Syringo -Encephalo –/ Myelo – Meningcocele (Syringo Myelia)")
6
DYS – HISTOGENESIS : incorrect migration and/or naturation – differentation ECTOPIC : mature tissue found in abnormal places HETEROPIC : intermingled of some mature tissues in abnormal places HAMARTOMA : abnormal composition of mature tissues at its normal places NEOPLASMA (GEN MUTATION) : benign and malignant
 : benign and malignant.")
7
Abnormalities of anatomy / location of NS
DYS – NEUROANATOMY Abnormalities of anatomy / location of NS - Dyslocation - Reverse of Several Centre DYS - NEUROCHEMISTRY - NEUROPHYSIOLOGY INHIBIT : Slow Conduction – Slow Movement / Analysis / etc EXCITE : Rapid / Hyperactivity (ies) DYS – REGULATION / CONTROL : UNCONTROL MOVEMENT – PATHOLOGICAL REFLEXES DYSFUNCTIONAL IMPULS CONDUCT
 DYS – REGULATION / CONTROL : UNCONTROL MOVEMENT – PATHOLOGICAL REFLEXES. DYSFUNCTIONAL. IMPULS CONDUCT.")
8
CNS CELLS NEURON GLIAL CELL CHOROID PLEXUS CELL ASTROCYTE
OLIGODENDROGLIA EPENDYMA MICROGLIA CHOROID PLEXUS CELL

9
OLIGO DENDROGLIA NEURON ASTROCYTE

10
Neuron Effector cells of Nervous System
Neuron loss with progressive aginh Neuron of CNS cannot effectively regenerate axons over long distance → limit ability of CNS to respond to different type of injury Infarct transects internal capsule creates permanent motor deficiti Neuron in CNS don’t remyelinate → demyelinating disease causes permanent functional deficit (multipel sclerosis)
")
11
PIGMENTED NEURON ( SUBSTANTIA NIGRA ) neuromelanin
 neuromelanin")
12
ATROPHIC NEURON hyperchromatic Loss of neurons
* global/regional reduction (atrophic) * single neuron
 * single neuron.")
13
ATROPHIC CEREBRAL CORTEX

14
CHROMATOLYSIS Injured neuron swell → cytoplasm swell → chromatolysis: response to injury Reversible/death CYTOPLASM FLUID ACCUMULATION MARGINATION NUCLEUS NISSL SUBSTANCE

15
CENTRAL CHROMATOLYSIS
ANTERETROGADE DEGENERATION

16
Astrocyte Support neurons Promote repair

17
ASTROCYTE

18
GLIOSIS Reaction to injury Proliferation of astrocyte
Evolves in hours to day and persists to an extent that is usually commensurate with the severity of injury Reactive astrocyte : gemistocytic astrocyte: exentric plump nuclei, eosinophilic cytoplam Glial scar: composed of reactive astrocytes and their processes.

19
GLIOSIS

20
GEMISTOCYTE

21
OLIGODENDROGLIA Neuroectodermal origin
Myelin-producing cells during late gestational period and early neonatal

22
EPENDYMA Modulate fluid transfer between the cerebrospinal fluid and CNS During gestation some viral target the ependymal cell → aqueductus stenosis → congenital hydrocephalus

23
CANALIS CENTRALIS EPENDYM

24
MICROGLIA Phagocytic macrophage-derived cells
Reactions: changes in areas of injury 2 pattern : focal and diffuse microgliosis Microglial nodule: responses to viral or other infection. Rod cells: prominent elongated nucleus Gitter cells: response to necrosis: it will become phagocytic, accumulate lipid and other material

25
MICROGLIA (PHAGOCYTE)
")
26
ACTIVATED MICROGLIA MYELINOLYSIS

27
INTRA NUCLEAR INCLUSION
( CYTOMEGALO VIRUS )
")
28
NEGRI BODY INTRACYTOPLASM (RED)
(RABIES ENCEPHALITIS)
")
29
VASCULAR DILATATION (HYPEREMIA) PMN NEUTROPHIL NEURONOPHAGIA
 PMN NEUTROPHIL NEURONOPHAGIA")
30
HYDROCHEPALUS TYPE : COMMUNICANS : obstruction occurs outside ventricle system NON-COMMUNICANS EXVACUO (COMPENSATED)
 .")
31
HYDROCEPHALUS Primary hydrocephalus Secondary hydrocephalus
Accompanied by increased intracranial pressure Due to: Obstruction Congenital acquired Impaired CSF absorption Excess CSF production Secondary hydrocephalus Compensatory to loss of cerebral tissue

32
SITES OF OBSTRUCTION OF CSF PATHWAY
Subarachnoid space Arachnoid granulationes Plexus choroid Lateral ventricle 3rd ventricle Cerebral aqueduct 4th ventricle Exit foramina

33
OBSTRUCTED AQUADUCT SYLVIOUS
( BRAIN TUMOR)
")
34
OBSTRUCTIVE HYDROCEPHALUS
( NEOPLASM )
")
35
OBSTRUCTIVE HYDROCEPHALUS
( INFECTION )
")
36
OBSTRUCTIVE HYDROCEPHALUS
( GLIAL TISSUE POST VIRAL INFECTION)
")
37
TRAUMA Penetrating wounds produce hemorrhage and blast effects. Velocity contributes a blast effect to a projectile High-velocity : it disrupts tissues by its own mass and also centrifugal blast that enlarges the diameter → immediate death Low-velocity Seizures are threat in healed penetrating wounds, 6-12 mo after : collagenous tissue is displaced in the brain

38
HIGH VELOCITY BULLET WOUND

39
LOW VELOCITY BULLET WOUND

40
HEMORRHAGIC TRACT (PENETRATING WOUND)
")
41
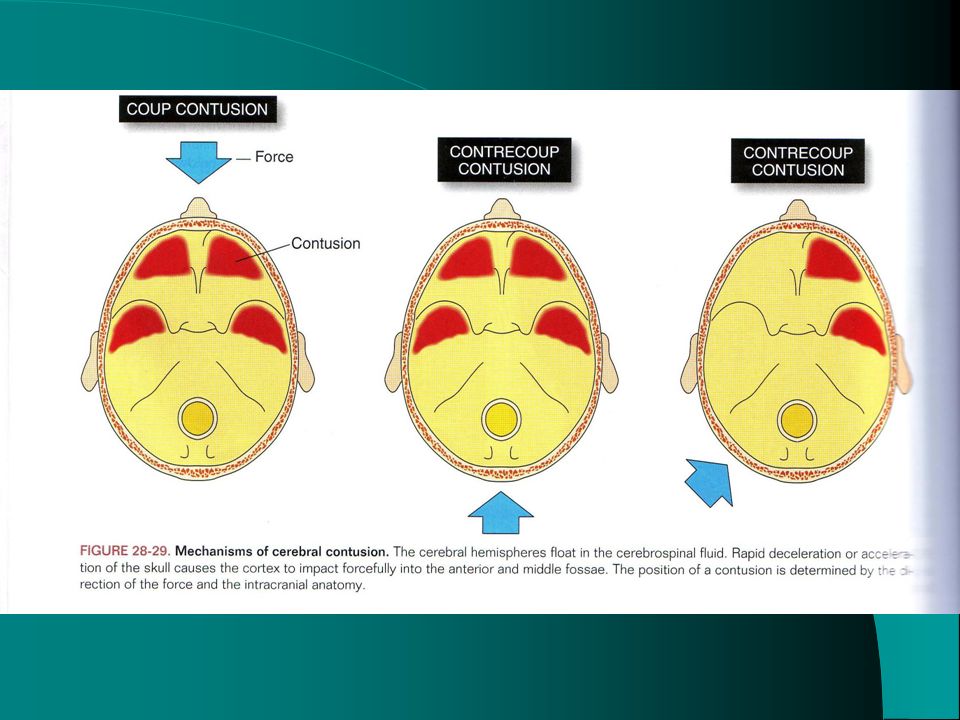
Subdural hematoma Significant cause of death from falls, assaults, vehicular acidents, sporting mishaps Frontal/occipital area is struck by blunt object → cerebral hemispher displaced in an anteroposterior direction → hit against inner aspect Soft cerebral tissue becomes compact then recoil → shearing effect Usually stop after mL

43
Subdural hematoma Tissue response
Formation of granulation tissue → outer membrane Fibroblast from outer membrane moved into the hematoma → inner membrane : 2 weeks Evolution: Reabsorbe leave a small amount of telltale hemosiderophage Remain static, with potential for calcification Enlarge : 6 months

44
CHRONIC SUBDURAL HEMATOMA
(INNER NEOMEMBRANE)
")
45
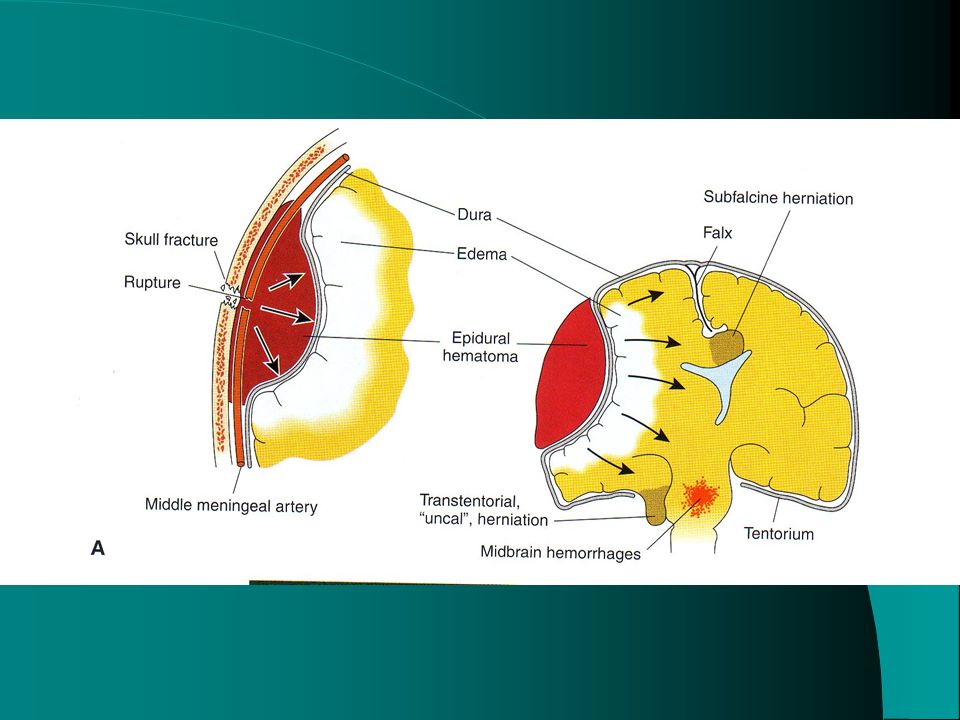
EPIDURAL HEMATOMA Middle meningeal artery branches splay across temporal-parietal area Hemorrhage into epidural space, separating dura from calvaria 4-8 hours: asymptomatic 30-50 mL: intracranial pressure increased → exceed venous pressure → circulatory stagnation and cerebral ischemia → global cerebral hypoxia

46
EPIDURAL HEMATOMA Cushing reflex : protective response
HR slow to increase ventricular filling Myocardial contraction is forceful Systolic pressure increased Compensatory mechanism exhausted : temporal lobe displaced downward → transtentorial herniation Herniation compress uncus/hyppocampus against midbrain and other structures : 3rd cranial nerve Pupil fixed and dilated

48
EPIDURAL HEMATOMA (FRONTO PARIETAL)
")
49
HERNIATION Cingulate gyrus under falx cerebri
Hippocampal uncus and parahippocampal gyrus over tentorium cerebeli Cerebelar tonsilar through foramen magnum Any defect in the dura and skull SITES OF HERNIATION

50
TRANSTENTORIAL HERNIATION (MIDBRAIN DISPLACED)
")
51
GLIOBLASTOMA MULTIFORME HEMORRHAGE HERNIATION

54
DEGENERATIVE DISORDERS
Head, generalized cerebral atrophy – CTscan

55
DEGENERATIVE DISORDERS
Brain, cerebral cortex, Alzheimer disease, silver stain

56
DEGENERATIVE DISORDERS
Brain, cerebral cortex, neuritic plaque stained for tau protein and beta-amyloid

57
DEGENERATIVE DISORDERS
Brain, substantia nigra, Lewy bodies

58
ALZHEIMER

59
Alzheimer Amyloid β protein Neurofibrillary tangles Genetic factors
Derived from APP Normal degradation of APP: proteolytic middle domain Alzheimer : proteolytic in either end Neurofibrillary tangles Paired of helical filaments consisted of abnormal form of MAP: tau Phosphorylation of tau results in a protein not associated with microtubules → deprives cells of its microtubules effect Impairing axonal transport & compromising neuronal function Genetic factors Apolipoprotein E

60
DEGENERATIVE DISORDERS
Spinal cord, amyotrophic lateral sclerosis (A) and normal (B)
 and normal (B)")
61
DEGENERATIVE DISORDERS
Brain, Creutzfeldt-Jakob disease

62
Prion disease (spongiform encephalopathies)
Transmissible neurodegenerative disease Infectious agents is prion Human prion gene (PRNP) express cell-surface glycoprotein bound to plasmalemma by glycolipid anchor PrPc and PrPsc not differ in sequence except 3 dimensional conformation an patterns of glycosylation
 express cell-surface glycoprotein bound to plasmalemma by glycolipid anchor. PrPc and PrPsc not differ in sequence except 3 dimensional conformation an patterns of glycosylation.")
64
Prion disease Kuru Creutzfeldt-Jacob disease (CJD) Fore people
Trembling Canibalism Spongiform cerebral and cerebelum Creutzfeldt-Jacob disease (CJD) Symptoms begin insidiously 6 months exhibits severe dementia 1 year : death
 Symptoms begin insidiously. 6 months exhibits severe dementia. 1 year : death.")
65
Prion disease Sporadic Inherited Iatrogenic New variant CJD

66
Sporadic 75% 1: 1.000.000 Polymorphisme codon 129 Classical features
Dementia Myoclonus Periodic spike-wave complexes

67
Genetic 15% Gertsmann-Straussler-Scheiner syndrome(GSS)
Spinocerebelar ataxia with demntia Fatal familial insomnia Profound disturbance of sleep-wake cycles Sings of pyramidal and cerebellar dysfunctions Mutation codon 178 PRNP gene

68
Iatrogenic Hormone injection Tissue grafts Medical devices
Human growth hormone (55 cases) Human pituitary gondotropin (5 cases) Tissue grafts Duramater (11 cases) Cornea (1 case) Pericardium (1 case) Medical devices Depth electrode (2 cases) Surgical instruments (not definitely proven)
 Human pituitary gondotropin (5 cases) Tissue grafts. Duramater (11 cases) Cornea (1 case) Pericardium (1 case) Medical devices. Depth electrode (2 cases) Surgical instruments (not definitely proven)")
69
New variant CJD Identified following surveillance following BSE epidemic in UK Mean age 26 years (compared to sporadic 65) Dysesthesia, none EEG of sporadic CJD Spngioform in basal ganglia and thalamus Extensive PrP plaques in cerebrum and cerebelum More PrP than sporadic CJD BSE is likely the source of vCJD

72
Thank You

Similar presentations





















 Central Nervous System Communication and coordination system of the body Seat of intellect and reasoning Consists of the.>")

 developmental.>")
 Brain and spinal cord Peripheral Nervous System (PNS) ◦ nerves.>")
