Download presentation
Presentation is loading. Please wait.

1
Clinical Teaching in the ED

2
Educational Objectives
Develop skills to become a better clinical educator

3
How to… How to provide effective teaching while caring for patients in the ED

4
Residents as Teachers Residents play a critical role in medical student education Professional role models for students Impact on career choices Better understanding of students needs

5
Residents as Teachers General principles of clinical teaching
Bedside teaching Giving effective feedback Teaching procedures Teaching with High-Fidelity patient simulators Teaching effective discussion leading and lecturing Acad Emerg Med. 2006;13:

6
Precepting Medical Students
Make decisions at the bedside Encourage medical student independence Delegate specific tasks to the student Encourage responsible behavior

7
The Emergency Department
Different from inpatient and ambulatory care settings Complaint oriented specialty Unique educational opportunities

8
Opportunities Unique to EM
The undifferentiated acutely ill patient Extremes of age The poisoned or intoxicated patient Psychiatric emergencies Environmental emergencies Wound management and trauma Patients requiring emergency procedures Airway management and ultrasound

9
Teaching Opportunities
Unique content areas Teaching clinical vignettes Multitasking and time management skills Communication skills Role modeling professional behavior Reinforce EMC goals

10
EMC Goals “Competencies”
Perform complaint directed history and physical examinations Develop case specific differential diagnosis Present cases in a concise and organized fashion Appropriate utilization and interpretation of diagnostic studies Appropriate implementation of patient management plans Demonstrate medical professionalism Demonstrate an adequate fund of medical knowledge Demonstrate proficiency in basic procedures Temple MS IV Clerkship

11
EMC Objectives Directly participate and document care of at least 25 undifferentiated patients Directly participate and document care of at least 2 patients with each of the following conditions; Abdominal pain Chest pain Fever Musculoskeletal trauma / wound care Neurologic case Shortness of breath Provide & document “anticipatory guidance” for at least 5 patients Temple MS IV Clerkship

12
EMC Objectives Perform and / or interpret and document your participation in selected clinical skills or diagnostic tests; Interpret cervical spine radiograph Interpret chest radiograph Perform and interpret 12-lead ECG Perform intravenous access Perform phlebotomy Temple MS IV Clerkship

13
Observation of ED H&P’s
Acad Emerg Med 2003;42:s102

14
Observation of Procedures
Acad Emerg Med 2004;11:500

15
Direct Observation Direct observation of medical students performing H&P’s is uncommon Direct observation as a method of teaching is underutilized Medical students are more likely to receive both procedural instruction and assistance if selected procedures are directly observed

16
Diagnosing the learner
Medical Student - Intern Independent Learner Dependant Learner Intern - Senior Resident Assess the learners needs Strengths and weaknesses

17
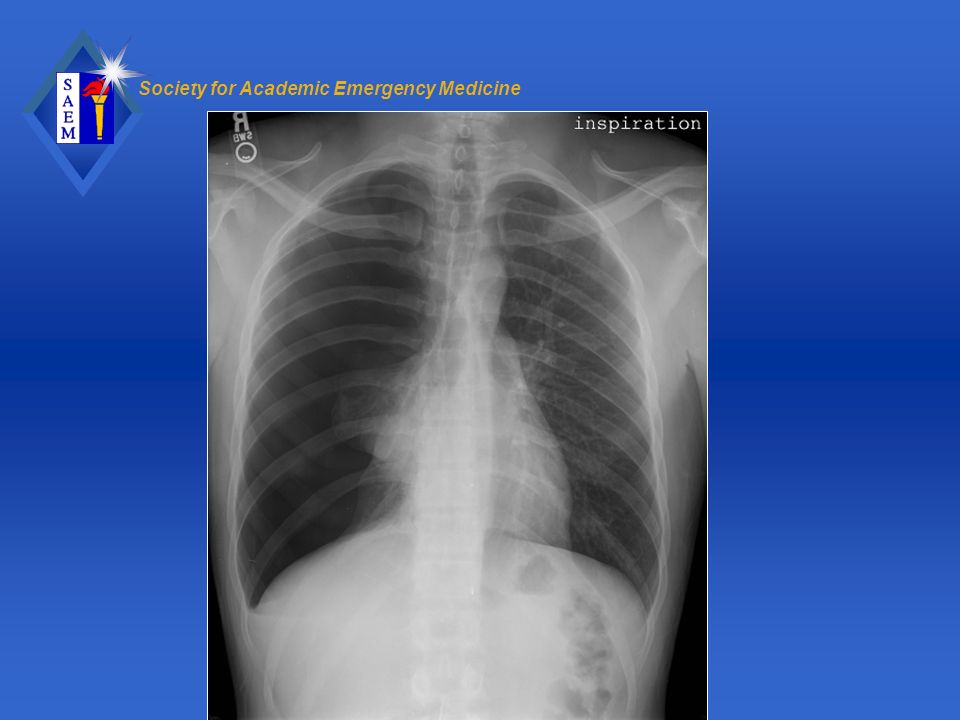
Case 1 35 year old male presents with CP and SOB

19
Case 1 Interpret the chest radiograph, provide a clinical diagnosis
Document how you would manage this case

20
Case 1 61% of students (n=192) correctly interpreted the chest radiograph 95% of the students that correctly interpreted the chest radiograph managed the case appropriately *Needle decompression *Tube thoracostomy

21
Student – Patient Encounter
Student evaluates patient Case presentation Preceptor verifies data Evaluation / management plan is implemented Periodic reevaluation / follow up Disposition

22
Case Presentation Skills
Improve: *Patient care *Educational experience *Learner – teacher communication

23
Case Presentations “Precepting pitfalls”
Interrupting the case prior before completion Taking over the case Inappropriate lectures

24
Case Presentations Listen carefully
Allow the presenter to proceed without interruption The post presentation pause… *Feedback *Reassurance *Validation *What should I do next?

25
Case Presentations Brief, focused 2 – 3 minutes in length
Directed opening statement *Chief complaint and pertinent PMH Description of the HPI, pertinent ROS Additional medical history, etc. Physical examination Differential diagnosis Diagnostic and treatment plan

26
Assessment – Oriented Presentation
Opening statement includes the diagnostic impression or assessment followed by a treatment plan Followed by historical and physical examination data including pertinent positive and negative features that support the clinical assessment Acad Emerg Med 2003;10:842-47

27
Method of Questioning Assertive Facilitative Teaching styles
Teacher Centered Learner Centered Fam Med 2001;33:344-6

28
Assertive Style Teacher – centered approach
Can gauge the learners knowledge base Asks direct questions Provides information Gives directions

29
Assertive Style What antibiotics should we treat this patient with?
What is the dose of _____? What is the drug of choice for_____? What is the differential diagnosis of RUQ pain?

30
Suggestive Style Can offer suggestions or alternative methods of patient care with questions or statements Can share opinions and practical experience

31
Suggestive Style “Although a KUB may be helpful, a non-contrast helical CT scan is a better diagnostic test for this patient” “Augmentin is a treatment option for strep throat, penicillin however is a more cost effective choice”

32
Collaborative Style Socratic approach Learner oriented
Explores clinical reasoning and problem solving abilities Use of higher level questions to promote critical thinking

33
Collaborative Style What do you think is wrong with the patient?
How should we proceed? What diagnostic studies are necessary? How should we manage this case? Do you think the patient needs to be admitted?

34
Facilitative Style Elicits and accepts the learners ideas to promote self understanding May also offer feelings and can encourage the learner Uses silence

35
Facilitative Style Ms. Jones shared some personal information about her past medical history with you. How did that make you feel?

36
Reactive Comments Ways to redirect and reorient the learner
The delayed response *Allows the learner to reflect and reconsider *Provides an opportunity to withdraw the incorrect answer *Gives the learner a second try

37
Ways to redirect and reorient the learner
Reactive Comments Ways to redirect and reorient the learner *Asking questions containing additional clues *Modifying the question so that the incorrect answer is correct *Treating wrong answers as possible

38
Precepting Models Traditional Model One Minute Preceptor
Patient Centered Learner Centered

39
Traditional Precepting Model
Patient centered Inquiry phase is diagnosis driven Most time is spent on patient care issues rather than learner issues The teacher functions as an expert consultant Focus on areas requiring clarification or areas missed during the presentation

40
One Minute Preceptor Model
Learner centered Inquiry phase elicits the learners understanding of the case Flexible / modifiable Used in both the inpatient and ambulatory care setting Five microskills Focus on the learners reasoning Fam Med 2003;35:391-3

41
One Minute Preceptor Model
Case presentation and discussion process Teach Teach a general rule Provide positive feedback Correct mistakes Diagnose Patient Listen Clarify Diagnose Learner Get a commitment Probe for supporting evidence

42
Get a Commitment Provides an assessment of the learners interpretation of the history and physical examination data Data analysis and synthesis What do you think is going on with this patient? What do you want to do for this patient? Commitment may focus on diagnosis, diagnostic evaluation, treatment plans, etc.

43
Probe for Supporting Evidence
Exploring the underlying thought process allows you to identify any gaps in data synthesis or misconceptions What findings support your diagnosis? What else do you think could be going on with this patient?

44
Teaching General Rules
Instruction is more memorable if offered as a general rule Teaching scripts for a particular complaint or presentation *Pearls of wisdom *Teach what learners need to know Keys features of a particular illness Treatment options Approach to a particular complaint Reason for hospital admission

45
Teaching General Rules
“You should always consider hypoglycemia in the differential diagnosis of a patient with an altered mental status” “You should always consider AAA in your differential diagnosis of non-traumatic low back pain in the elderly”

47
Feedback In the setting of clinical medical education, feedback refers to information describing students’ or house officers’ performance in a given activity that is intended to guide their future performance in that same or in a related activity JAMA 1983;250:777-81

48
Feedback Goals Praise the learner for a job well done
*Positive feedback Provide direction or suggestions on how the learner can improve their clinical performance *Constructive criticism *Guidance to correct mistakes

49
Feedback and Evaluation
*Formative Provides an honest assessment of performance, including suggestions for improvement Evaluation *Summative Describes performance as it relates to the achievement of learning objectives Course grade

50
Praise – Criticism – Praise
Feedback The way in which feedback is provided will influence the perception of its helpfulness Praise – Criticism – Praise

51
Feedback Nonjudgmental Descriptive Be consistent Well timed
*Refer to specific behaviors or actions Be consistent Well timed Ask for self evaluation Always start with positive feedback Incorporate suggestions for improvement Individualized

52
Brief Feedback Bedside Informal Unscripted Unplanned
*During observation of clinical / procedural skills *End of a patient encounter

53
Formal Feedback Usually more formal
May also be unscripted or unplanned Usually occurs away from the bedside *End of a patient encounter *End of a shift *Midpoint or end of the clerkship

54
Feedback July – December 2004
*51/53 MS completed the survey 96.1% of MS reported receiving feedback during their EMC Of the students receiving feedback, 80.4% reported receiving SFICP 93.6% of the students reported the feedback they received was beneficial 97% of supervising physicians felt that the feedback they provided was beneficial Ann Emerg Med. 2005;46:S88

55
Feedback No difference was noted in the frequency of feedback and SFICP provided as reported by the following groups: Academic (n=16) vs. clinical (n=9) faculty Senior (n=13) vs. junior (n=12) faculty Male (n=24) vs. female (n=9) supervising physicians Senior residents (n=8) and faculty (n=25)
 vs. clinical (n=9) faculty. Senior (n=13) vs. junior (n=12) faculty. Male (n=24) vs. female (n=9) supervising physicians. Senior residents (n=8) and faculty (n=25)")
56
Feedback The vast majority of SMS report receiving feedback
Most students felt that more feedback would be helpful Supervising physicians’ perception of providing feedback matched that reported by the students

57
Basic Teaching Teaching facts – knowledge
*Differential diagnosis for specific chief complaint *How to approach a certain clinical condition *Teaching the technique to perform a basic procedure

58
General Teaching Strategies
Tailor specific teaching to the level of the learner and the clinical situation *Get to know the student *Tailor teaching to students career interests *Use varied ED pathology to your advantage Optimize the interaction *Focus on one teaching point *Encourage problem solving *Incorporate bedside teaching

59
General Teaching Strategies
Seek opportunities to teach *Interesting physical examination findings *Radiographs *ECG’s *Procedures Be a professional *Be a role model *Establish a friendly learning environment *Be approachable

60
General Teaching Strategies
Use additional resources *Hard copy texts *On-line texts *Journal articles *Educational websites *Prepared cases *Old ECG’s, Xrays, etc.

61
Qualities of an Effective Teacher
Clinical competence Explaining the decision making process Treating learners with respect Actively involve learners Promote learner autonomy Teach with enthusiasm Communicate expectations for performance Creates a friendly teaching environment

62
Challenging Students Less than enthusiastic performance
*Lack of initiative *Lack of attention to details *Poor use of time *Repetitive mistakes *Defensive when receiving feedback *Unprofessional behavior

63
Alternative Teaching Methods
Brief structured observation Bedside case presentations

64
Brief Structured Observation
Designed to increase teaching effectiveness in busy clinical settings *Easy – no preparation *Brief – little time required

65
Brief Structured Observation
Observe the encounter Debrief the learner Conclude interaction

66
Observe the Encounter Brief observation
*2 – 5 minutes Limited to certain aspects of H & P Preceptor records observations / statements / actions performed by the learner

67
Debrief the Learner Ask the learner what they learned from the observed segment *Can be done in front of the patient Directly evaluate; *Fund of knowledge *Physical examination skills *Clinical reasoning skills

68
Conclude Interaction Feedback Point out strengths
*Positive reinforcement Give the learner one thing to work on *Suggestions for improving clinical performance

69
Bedside Case Presentations
Addresses challenges of teaching *Effective teaching vs patient care *Time management *Assessment of the learner Increases patient satisfaction Promotes professional behavior Mixed reactions from learners

70
Bedside Case Presentations
Implementation Learner and patient preparation *Use of medical terminology Listen to the presentation Clarify / obtain additional information Have learner present evaluation / treatment plan at the bedside ??? Address all patient concerns / questions

71
EM Clerkship Grades Emergency Medicine Clerkship
Uniform Grading Guidelines

72
Evaluation of Clinical Performance
Evaluation of acquired clinical knowledge, skills, attitudes, and behaviors *Clerkship goals “competencies” Ability to incorporate these competencies into clinical medicine

73
Evaluation of Clinical Performance
"Criterion – based” or “Fixed – standard" grading *Identify goals or competencies *Determine expected standards of proficiency *Achievement of the minimum standards of proficiency would represent a “pass” grade *Performance that is above the minimum expectations could earn grades such as “High Pass” and “Honors”

74
TUH – EM Clerkship Clinical Evaluation Card
Student Name: Date / Shift: Evaluator: Block: Clinical Skills: (Learning Objectives) 1. Perform complaint directed history & physical examinations 2. Develop case specific differential diagnosis 3. Present cases in a concise and organized fashion 4. Appropriate utilization and interpretation of diagnostic studies 5. Appropriate implementation of patient management plans 6. Demonstrate medical professionalism 7. Demonstrate an adequate fund of medical knowledge Demonstrate proficiency in basic procedures Patient acuity: High Medium Low Varied Patient encounters: – – or more Overall grade: H HP P C F
 1. Perform complaint directed history & physical examinations. 2. Develop case specific differential diagnosis. 3. Present cases in a concise and organized fashion. 4. Appropriate utilization and interpretation of diagnostic studies. 5. Appropriate implementation of patient management plans. 6. Demonstrate medical professionalism. 7. Demonstrate an adequate fund of medical knowledge. Demonstrate proficiency in basic procedures. Patient acuity: High Medium Low Varied. Patient encounters: 1 – 2 3 – 5 6 or more. Overall grade: H HP P C F.")
75
Feedback on clinical performance: Nonjudgmental, descriptive (refer to
specific cases, performances, behaviors, or actions), objective appraisal of performance Positive feedback (What did the student do well?): Suggestions to improve clinical performance: Any additional comments: Discussed with student Yes No
, objective appraisal of performance. Positive feedback (What did the student do well ): Suggestions to improve clinical performance: Any additional comments: Discussed with student Yes No.")
76
HONORS The outstanding student
Comprehensive achievement of the knowledge, skills, attitudes, and behaviors Top “10%” Resourceful, efficient, and insightful In-depth medical knowledge base Perform detailed but focused H & P’s Well organized presentations Role model Strives for excellence even in difficult situations

77
HIGH PASS Identify major problems The solid student
Perform appropriate but focused H & P’s Demonstrate professional behavior The solid student Well beyond minimum course requirements Next “25% - 35%” Resourceful and efficient Above average fund of medical knowledge

78
PASS The average student Meets basic course requirements
Next “50% - 60%” Average fund of medical knowledge Perform an adequate H & P May omit certain portions of the H & P Presentations generally organized Demonstrate professional behavior

79
CONDITION / FAIL A performance that falls below expected minimum standards *Clinical knowledge, skills, attitudes, and behaviors Requires specific and detailed documentation by senior EM resident and / or attending

80
Expected Grade Distribution
Rigid cut off values are not used Year to year the percentage of students receiving a particular grade may vary

81
Summative Evaluation Overall shift grade Honors (5) High Pass (4)
Condition (0) Fail (0) # of patient encounters 1 – 2 (x1) 3 – 5 (x2) 6 or more (x3)
 Fail (0) # of patient encounters. 1 – 2 (x1) 3 – 5 (x2) 6 or more (x3)")
82
RIME Evaluation Framework
Reporter Interpreter Manager Educator Pangaro LN Uniformed Services University of the Health Sciences

83
Reporter Accurately gathers and clearly communicates clinical facts
*Medical interviewing *Physical examination skills *Case presentations

84
Interpreter Prioritizing the patient’s presenting complaints
*Developing a problem list *Developing a differential diagnosis *Interpreting basic diagnostic studies

85
Manager Developing a diagnostic and therapeutic plan
Tailoring the management plan to the patient

86
Educator Self-directed learning Critical reading skills

87
Barriers to Effective Teaching

88
Barriers to Teaching The Emergency Department The Teacher The Student
The Patient

89
The Emergency Department
Overcrowding Inadequate patient care space Unanticipated emergencies High level of acuity

90
Teaching Opportunities
Unique content areas Teaching clinical vignettes Multitasking and time management skills Communication skills Role modeling professional behavior Reinforce EMC goals

91
The Teacher Lack of confidence Little experience
Little or no formal training Not enough time Endless interruptions Too many other responsibilities Expectations?

92
The Teacher Every case has a teaching point
You have more experience than the students and junior residents Directed learning *Identify interesting cases *Task oriented learning Act interested

93
The Student Different levels of training Variable fund of knowledge
Learning attitude, enthusiasm Expectations?

94
The Student Identify gaps or misconceptions Teach to their level
Focus on one thing at a time

95
The Patient Level of acuity Painful injury or illness Mental status
Need for privacy Patient reluctance

96
The Patient Bedside teaching rounds are generally viewed as having a positive effect on patient care Most patients enjoy bedside teaching and often develop an increased understanding of their illness. Incorporate patients into the case discussion

97
Effective Clinical Teaching
No one best teaching style or method Teaching principles *Allow the student to play an active part in learning *Use questions that promote high order thinking *Offer feedback Reinforce positive behavior / actions Provide guidance for correcting mistakes

98
Be flexible (different levels of training)
The Bottom Line… Decide what to teach Take away point *History *Physical examination *Diagnostics *Therapeutics Be flexible (different levels of training)
")
99
Author Credit – Clinical teaching: David A. Wald DO
Questions

100
Postresidency Tools of the Trade CD
13) Negotiation – Ramundo 14) ABEM Certifications – Cheng 15) Patient Satisfaction – Cheng 16) Billing, Coding & Documenting – Cheng/Hall 17) Financial Planning – Hevia 18) Time Management – Promes 19) Balancing Work & Family – Promes & Datner 20) Physician Wellness & Burnout – Conrad /Wadman 21) Professionalism – Fredrick 22) Cases for professionalism & ethics – SAEM 23) Medical Directorship – Proctor 24) Academic Career Guide Chapter 1-8 – Nottingham 25) Academic career Guide Chapter 9-16 – Noeller 1) Career Planning – Garmel 2) Careers in Academic EM – Sokolove 3) Private Practice Career Options - Holliman 4) Fellowship/EM Organizations – Coates/Cheng 5) CV – Garmel 6) Interviewing – Garmel 7) Contracts for Emergency Physicians – Franks 8) Salary & Benefits – Hevia 9) Malpractice – Derse/Cheng 10) Clinical Teaching in the ED – Wald 11) Teaching Tips – Ankel 12) Mentoring - Ramundo
 Negotiation – Ramundo. 14) ABEM Certifications – Cheng. 15) Patient Satisfaction – Cheng. 16) Billing, Coding & Documenting – Cheng/Hall. 17) Financial Planning – Hevia. 18) Time Management – Promes. 19) Balancing Work & Family – Promes & Datner. 20) Physician Wellness & Burnout – Conrad /Wadman. 21) Professionalism – Fredrick. 22) Cases for professionalism & ethics – SAEM. 23) Medical Directorship – Proctor. 24) Academic Career Guide Chapter 1-8 – Nottingham. 25) Academic career Guide Chapter 9-16 – Noeller. 1) Career Planning – Garmel. 2) Careers in Academic EM – Sokolove. 3) Private Practice Career Options - Holliman. 4) Fellowship/EM Organizations – Coates/Cheng. 5) CV – Garmel. 6) Interviewing – Garmel. 7) Contracts for Emergency Physicians – Franks. 8) Salary & Benefits – Hevia. 9) Malpractice – Derse/Cheng. 10) Clinical Teaching in the ED – Wald. 11) Teaching Tips – Ankel. 12) Mentoring - Ramundo.")
Similar presentations