Download presentation
Presentation is loading. Please wait.

1
Aspects on the Role of the Pathologist in CRC
Najib Haboubi FRCS FRCP FRCPath D Path Professor of Health Sciences, Liver and Gastrointestinal Pathology. University Hospital of South Manchester UK

2
Selected Topics Multi Disciplinary Meeting(MDT).
Resection Margins (Long and Circumferential). Assessment after CRT for Rectal Cancer
. Assessment after CRT for Rectal Cancer.")
3
Background In UK (60m) there are 35,000 new cases and 16,000 deaths per annum. New patterns in some parts of the world. In India 6th commonest among female and 9th amongst male.

4
Accurate Pathological Reporting
Confirm diagnosis. Inform prognosis. Plan treatment of individual patients. Audit pathology services. Evaluate and audit the quality of other services like radiology, surgery and oncology. Collect accurate data for cancer registration and epidemiology. Facilitate high quality research. Plan service delivery.

5
Multi Disciplinary Team (MDT)
Colorectal Surgeons Radiologists. Pathologists. Oncologists. Specialist Nurse. Hepatobiliary(Thoracic) Surgeon Stoma Nurse. Clinical geneticist / counsellor. Social worker. Clinical trials coordinator or research nurse. GP Dietician. Gastroenterlogist
 Surgeon. Stoma Nurse. Clinical geneticist / counsellor. Social worker. Clinical trials coordinator or research nurse. GP. Dietician. Gastroenterlogist.")
7
Video Conferencing

8
MDT Takes place at regular intervals
Encourages a more efficient and team working atmosphere . Have a consensus approach to treatment according to agreed protocols. Quick and appropriate referral pattern. Audit surgical treatment. Audit pathology reports.

11
Evidence Based

12
Second Edition 2007 Few important additions.

15
Assessment of RM Longitudinal
Circumferential / lateral /Radial / non peritonealised resection margin.

16
Minimum safe Longitudinal Margin
5 3 2 1 < 1cm

17
Reappraisal of 5 cm rule of distal excision for carcinoma of rectum
Williams , Dixon and Johnston Br.J.Surgery 1983

18
Conclusion The application of the 5 cm rule of distal excision may cause patients with low rectal cancer to lose their anal sphincter unnecessarily.

19
Kirwan , Drumm, Hogan, Keohane
Determining safe margin of resection in low anterior resection for rectal cancer. Br.J.Surg 1988 1cm

20
Declining indication for APR resection in favour of AR
Kirwan , O’Riordain and Waldron….. Br.J.Surg 1989

21
Karanjia, Schache, North and Heald
‘Close shave’ in anterior resection. Br.J.Surg. 1990 <1cm V >1cm

22
Conclusion Reduction of resection margins (provided TME and washout is properly performed) does not increase local recurrence or compromise survival.
 does not increase local recurrence or compromise survival.")
23
DCR 2011

24
Conclusion Does not influence Oncological outcome

25
Additions in the 2nd edition (1)
Documentation type of procedure . For rectal cancer, it is expected to have more AP than APR .

26
National Audit AR 1670 APR 746 Hartman’s 299
There is a trend of increase the AR over APR due to: Better preoperative treatment Better imaging modalities and Better surgery . Good surgeons should be able to undertake AR for tumours above 5cm from anal verge.

27
Currently Increasingly there are surgeons who practice restorative surgery for ‘ultra’ low rectal cancer: 3 cm

28
Circumferential (CRM) / Lateral / Radial / Non Peritonealised Resection Margin (NPRM)
 / Lateral / Radial / Non Peritonealised Resection Margin (NPRM)")
30
Circumferential resection margin Involvement (CRMI) 1mm or less
High Local Recurrence. Low Survival. Poor Standard of Surgery. Aggressive Disease. Tumour Location. Male gender.

35
Addition to the 2nd edition (2)
Grading of surgical plane of resection in rectal cancer. The continuous feedback to surgeons may lead to improve quality of surgery.

36
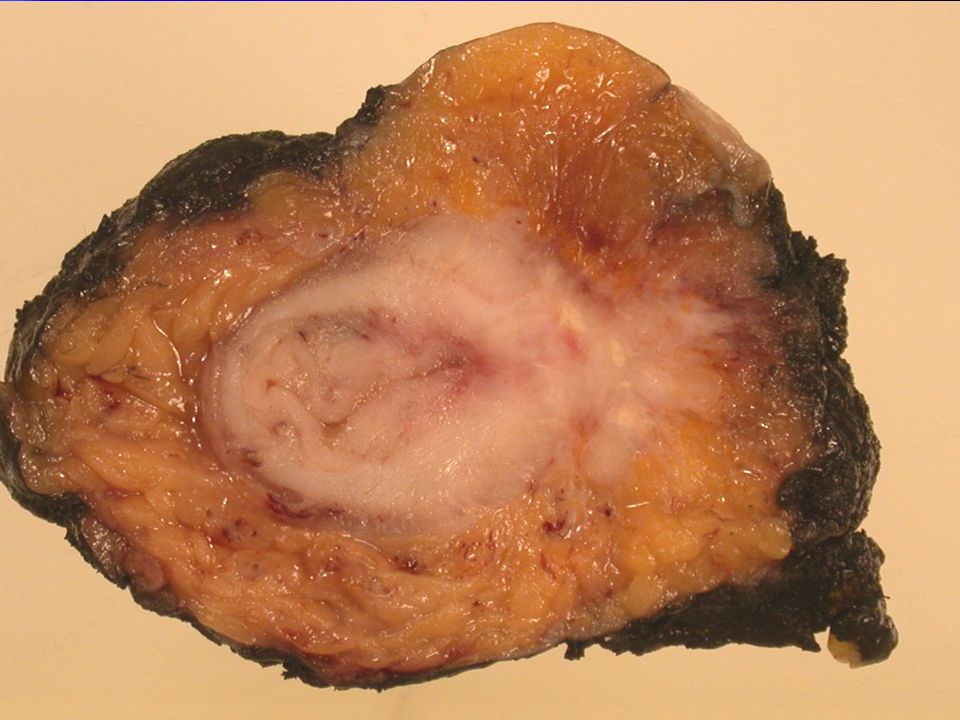
Macroscopic Evaluation of Rectal cancer Resection Specimens
Clinical Significance of the Pathologist in Quality Control. 2 years follow up. Iris Nagtegaal et al J Clin Oncol 2002, 20:

37
Macroscopic Grading of TME
A (3) ( Good). Complete. Smooth, no coning, defect >5 mm and regular CRM C (1) ( Poor). Defects down to the Muscularis ,conning, no bulk and irregular CRM B(2) .Nearly complete. Defect present but Muscularis is not apparent(except at the insertion of LA) and irregular CRM.
 ( Good). Complete. Smooth, no coning, defect >5 mm and regular CRM. C (1) ( Poor). Defects down to the Muscularis ,conning, no bulk and irregular CRM. B(2) .Nearly complete. Defect present but Muscularis is not apparent(except at the insertion of LA) and irregular CRM.")
39
Results Grade A&B - good and acceptable C- Poor Local Recurrence 8.7%
15% Local recurrence and Distant Metastasis 20.3% 36.1% 2 Year Survival 90.5% 76.9%

40
Addition to the 2nd edition (3)
Measurement of tumour beyond the muscularis propria recorded in mm. This is to: a/ facilitate audit of preoperative imaging of extramural spread as it is of importance in selecting patients of rectal cancer to choose a therapy arm . b/ It has a prognostic implication for rectal cancer. 5mm or more is associated with adverse prognosis.

42
Addition to the 2nd edition (4)
Recording tumour involvement of the NPRM in colonic tumours (in addition to rectum) like the caecum. These patients may be selected for post operative adjuvant therapy. Bateman et al J Clin Path 2005 and Quirke et al 2006 J Path
 like the caecum. These patients may be selected for post operative adjuvant therapy. Bateman et al J Clin Path 2005 and Quirke et al 2006 J Path.")
43
Addition to the 2nd edition (5)
Recording serosal ( peritoneal surface) involvement. ‘Tumour cells visible either on the peritoneal surface or free in the peritoneal cavity carry bad prognosis’
 involvement. ‘Tumour cells visible either on the peritoneal surface or free in the peritoneal cavity carry bad prognosis’")
44
Shepherd, Baxter and Love J. Clin. Path 1995
Influence of local peritoneal involvement on pelvic recurrence and prognosis in rectal cancer. Shepherd, Baxter and Love J. Clin. Path 1995

45
Local Peritoneal Involvement
Detected in 25.8% (54/209) of cases. Showed considerable prognostic disadvantage in curative and non curative cases. May be an important factor in local recurrence of upper rectal cancers.
 of cases. Showed considerable prognostic disadvantage in curative and non curative cases. May be an important factor in local recurrence of upper rectal cancers.")
46
The Prognostic Importance of Peritoneal Involvement in Colonic Cancer: a Prospective Evaluation
Shepherd et al Gastroenterology 1997 Strong predictive value for local recurrence / persistent disease specially when there is mucinous differentiation.

47
Additions in the 2nd edition (6)
Recording of marked or complete tumour regression in patients with rectal cancer that have received adjuvant chemo / radiotherapy (CRT)
")
48
Rectal cancer that have received adjuvant R/CRT.
Tumour regression is associated with improved prognosis.

49
Pathologist should record marked or CTR
Rectal cancer that have received adjuvant R/CRT. Tumour regression is associated with improved prognosis.

50
1895 XRT 1st used

51
BMJ 1897

52
Rationale for combined CRT for Rectal Cancer
Chemotherapy increases tissue sensitivity towards radiation. Radiation stops proliferation. Both tumourus and non tumourus tissue are affected.

53
Changes afflicting Tumour

54
Three folds decrease in local recurrence.
Short course preoperative radiotherapy interferes with the determination of pathological parameters in rectal cancer Iris Nagtegaal et al. J Path 2002,197: patients(706 TME alone, 598 TME+RT) No change in stage (No change in depth and although there is decrease in no. of LN retrieval but not in +ve lymph nodes)!! Three folds decrease in local recurrence.
 No change in stage (No change in depth and although there is decrease in no. of LN retrieval but not in +ve lymph nodes)!! Three folds decrease in local recurrence.")
55
Long course CRT Improves staging (depth and LN status).
Associated with c&pCTR

56
Classifications of Regression
Mandard : Cancer 1994,73; (1-5) Dworak : Int CRD 1997,12; (0-4) Wheeler : DCR 2002,45; (1-3) Ryan : Histopathol 2005,47;141.(1-3) PRINCIPLE Tumour Volume V Fibrosis.
 Dworak : Int CRD 1997,12;19. (0-4) Wheeler : DCR 2002,45;1051. (1-3) Ryan : Histopathol 2005,47;141.(1-3) PRINCIPLE. Tumour Volume V Fibrosis.")
57
Discrepancy in Staging
Author Grade Best Response (pCR) Worst Response Mandard 1-5 1 5 Dworak 0-4 4 Wheeler 1-3 3 Ryan
 Worst Response. Mandard Dworak Wheeler Ryan.")
58
Ryan’s modification of Mandard’s 5 point system
G1: No viable cancer cells (pCTR) : Single cells or small groups of cancer cells. G2: Residual cancer cells outgrown by fibrosis. G3: Significant fibrosis outgrown by cancer cells. : No fibrosis with extensive residual cancer.
 : Single cells or small groups of cancer cells. G2: Residual cancer cells outgrown by fibrosis. G3: Significant fibrosis outgrown by cancer cells. : No fibrosis with extensive residual cancer.")
59
Rayan et al Histopathology:2005,47:141-146. 60 patients G1, G2,G3.
Pathological response following long-course neoadjuvant CRT for locally advanced rectal cancer Rayan et al Histopathology:2005,47: 60 patients G1, G2,G3. none of the G1&2 (excellent and good) had local recurrence after mean 22 months.
 had local recurrence after mean 22 months.")
66
CTR we must be clear either pathologic (pCR) or clinical (cCR)
15-30% achieve pCR 25-50% of cCR are confirmed as pCR at subsequent surgery.

67
What do we do when there is cCR?

68
Operative Versus Non Operative Treatment for Stage 0 Distal Rectal Cancer Following Chaemoradiation Therapy Long-term Results Angelita Habr-Gama, et al Ann Surgery 2004

69
Results 26.8% of patients who received CRT developed complete clinical tumour response (observational group). Full thickness biopsy? The five-year overall and disease-free survival rates were 88% and 83% in Resection Group and 100% and 92% in Observation Group

70
Conclusion Stage 0 rectal cancer disease is associated with excellent long-term results irrespective of treatment strategy. Surgical resection may not lead to improved outcome in this situation and may be associated with high rates of temporary or definitive stoma construction and unnecessary morbidity and mortality rates.

71
Complete Clinical response After Preoperative CRT in Rectal cancer
Is Wait and See Policy Justified? Glynne-Jones et al DCR 2008 Narrative Review of 246 studies

72
Results The end point of complete clinical response is inconsistently defined. Insufficiently robust. Partial concordance with pathological complete response.

73
Conclusion The rationale of ‘wait and see’ policy when complete clinical response status is achieved relies on retrospective observations which are insufficient to support such policy. EXCEPT In patients who are recognised as unfit or refused surgery

74
What do we do when there is cCR?
There are at least one trial in UK and an audit in the North West Region. Registering ALL cases with cCR and cPR. Outcome?

75
`

76
The effective management of CRC requires
The involvement of the histopathologist at various stages of treatment pathway. Diagnostic. Therapeutic. Audit. Research.

80
FACTORS INFLUENCING BIOLOGICAL RESPONSE
Related to host and tissue. Related to therapy

81
Factors related to therapy
Dose . High dose more toxic Field. Large field more toxic. Concomitant chemotherapy is more toxic Post operative RT is more toxic than pre operative RT

82
MORPHOLOGY

83
Acute radiation colitis in patients treated with short term preoperative radiotherapy for rectal cancer Leupin et al (Switzerland) Am J Surg. Path. 2002
 Am J Surg. Path")
84
Radiation colitis Long Course
Short Course Sever mucosal inflammation. Prominent eosinophils. Crypt disarray Crypt epithelial damage. Nuclear abnormality Apoptosis of crypt epithelium. Either clinically silent or quick recovery. Long Course These features are either absent or rarely detected.

85
Haboubi, Rowland, and Schofield
The Light and Electron Microscopic Features of Early and Late Radiation-Induced Proctitis Haboubi, Rowland, and Schofield Am.J.of Gastro. 1988

91
Conflicts in the literature

92
How SC differs from LC in pathological and clinical parameters
78 patients(SC 65, LC13) Age (average 67 years) 54 males and 25 females Mean follow up 56 months(4-105) AR in 31 cases; APR in 47cases.
 Age (average 67 years) 54 males and 25 females. Mean follow up 56 months(4-105) AR in 31 cases; APR in 47cases.")
93
Results 1 32 Responders (Ryan grade 1 and 2)
10(76%) of LC vs. 22(33%)SC.
 of LC vs. 22(33%)SC.")
94
Results 2 7 patients had local recurrence (6SC,1LC)
Regression did not correlate with local recurrence

95
Result 3 Regression did not correlate with overall survival

96
Prognostic Significance of Tumour Regression After Preoperative CRT for RC
Rodel et al .J Clin Oncol 2005,23:8688 G 4 (Good) in 10.4% DFS 86%. G 2& DFS 75% G 0&1(Bad) >10% DFS 63%
 in 10.4% DFS 86%. G 2&3 DFS 75% G 0&1(Bad) >10% DFS 63%")
97
Result 4 Overall mortality correlated with lymph node positivity (p=0.009) 29% of responders were LN+ve versus 48% non responders
 29% of responders were LN+ve versus 48% non responders.")
98
Absence of LN in the resected specimen after Radical Surgery for Distal Rectal Cancer and Neoadjuvant CRT: What does it mean? Habr-Gama et al DCR 2008,51; 32(11%) patients had no LN.5YDFS 74% 171(61%) had ypNO YDFS 59% 78(28%) had yp(N+) YDFS 30%
 patients had no LN.5YDFS 74% 171(61%) had ypNO. 5YDFS 59% 78(28%) had yp(N+). 5YDFS 30%")
Similar presentations


























 patients Policy.>")








 MDT DATA FOR PATIENTS DIAGNOSED AUGUST 2010-JULY 2011 YSBYTY GWYNEDD (YG) MDT.>")





