Download presentation
Presentation is loading. Please wait.

1
HEARTLINE HSM Genoa Cardiology Meeting
NUOVI ORIZZONTI FARMACOLOGICI NELLA CARDIOPATIA ISCHEMICA Cardiopatia ischemica: nuovi orizzonti nella terapia con antiaggreganti orali Giancarlo Casolo Genova, Hotel NH Marina 21/22 Ottobre 2011

3
ESC Guideline 2010

4
Guidelines on myocardial revascularization

5
Prasugrel Ticagrelor Guidelines on myocardial revascularization

6
ESC Guideline 2011

7
STUDIO PLATO STUDIO TRITON TIMI 38 Current Oasis 7

8
STUDIO TRITON TIMI 38 STUDIO PLATO

9
TRITON-TIMI 38: Study Design
Wiviott SD et al AHJ 152: 627,2006 Adapted with permission from E.Antman TRITON-TIMI 38: Study Design ACS (STEMI or UA/NSTEMI) & Planned PCI ASA N= 13,600 Double-blind CLOPIDOGREL 300 mg LD/ 75 mg MD PRASUGREL 60 mg LD/ 10 mg MD Median duration of therapy - 12 months Patients were candidates for the trial if they were moderate-high risk, had an acute coronary syndrome, and there was a plan to perform PCI. A sample size of 13, 600 was considered necessary to provide at least 90 % power to test the primary hypothesis All patients were to receive ASA. Randomization was stratified by UA/NSTEMI vs STEMI DB study drug therapy consisted either of - standard dosing with clopidogrel with a LD of 300 mg and MD of 75 mg - OR prasugrel with a LD of 60 mg and MD of 10 mg DB study drug was to be given for a median of at least 12 months with a minimum of 6 mos and maximum of 15 months The primary composite EP was CV death, MI, or Stroke through the end of the study Key secondary EPs are listed here and among these was Stent thrombosis Key safety Eps included: TIMI major (non CABG) bleeds, and life-threatening bleeds Two key substudies are evaluating pharmacokinetics and genomics 1o endpoint: CV death, MI, Stroke 2o endpoints: CV death, MI, Stroke, Rehosp-Rec Isch CV death, MI, UTVR Stent Thrombosis (ARC definite/prob.) Safety endpoints: TIMI major bleeds, Life-threatening bleeds Key Substudies: Pharmacokinetic, Genomic 9 9 9
 & Planned PCI. ASA. N= 13,600. Double-blind. CLOPIDOGREL. 300 mg LD/ 75 mg MD. PRASUGREL. 60 mg LD/ 10 mg MD. Median duration of therapy - 12 months. Patients were candidates for the trial if they were moderate-high risk, had an acute coronary syndrome, and there was a plan to perform PCI. A sample size of 13, 600 was considered necessary to provide at least 90 % power to test the primary hypothesis. All patients were to receive ASA. Randomization was stratified by UA/NSTEMI vs STEMI. DB study drug therapy consisted either of - standard dosing with clopidogrel with a LD of 300 mg and MD of 75 mg. - OR prasugrel with a LD of 60 mg and MD of 10 mg. DB study drug was to be given for a median of at least 12 months with a minimum of 6 mos and maximum of 15 months. The primary composite EP was CV death, MI, or Stroke through the end of the study. Key secondary EPs are listed here and among these was Stent thrombosis Key safety Eps included: TIMI major (non CABG) bleeds, and life-threatening bleeds. Two key substudies are evaluating pharmacokinetics and genomics. 1o endpoint: CV death, MI, Stroke. 2o endpoints: CV death, MI, Stroke, Rehosp-Rec Isch CV death, MI, UTVR Stent Thrombosis (ARC definite/prob.) Safety endpoints: TIMI major bleeds, Life-threatening bleeds Key Substudies: Pharmacokinetic, Genomic")
10
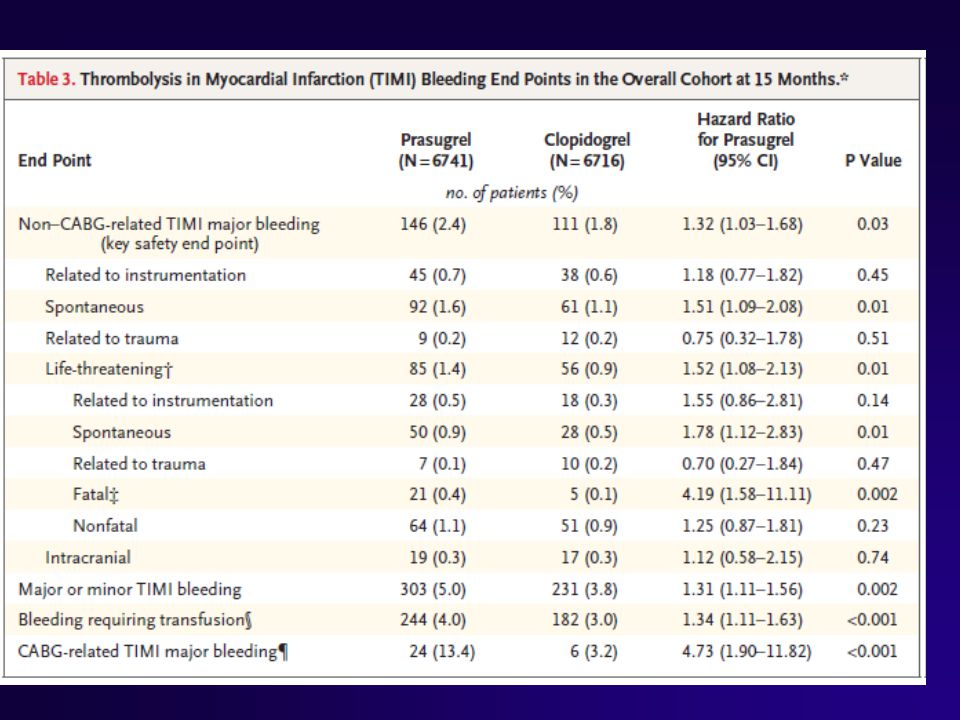
Balance of Efficacy and Safety TIMI Major NonCABG Bleeds
TRITON: Results 15 138 events Clopidogrel HR 0.81 ( ) P=0.0004 12.1 CV Death / MI / Stroke 9.9 10 NNT = 46 Endpoint (%) Prasugrel This slide depicts the balance of efficacy and safety observed in the trial. At the top is shown the significant reduction in the primary endpoint as presented a few moments ago. The number needed to treat to prevent one event was 46 At the bottom is the rate of TIMI major non CABG bleeds--a key safety endpoint-- which was 2.4% with prasugrel and 1.8% with clopidogrel—a 0.6% Absolute risk increase. The excess of 35 major bleeds with prasugrel corresponded to an HR of 1.32 and P value of The number of subjects who would need to be treated to result in one excess major bleed (NNH) was 167. 5 35 events TIMI Major NonCABG Bleeds Prasugrel 2.4 HR 1.32 ( ) P=0.03 1.8 Clopidogrel NNH = 167 30 60 90 180 270 360 450 Adapted with permission from Wiviott SD et al NEJM 357:2007 Days 10 10 10
 P= CV Death / MI / Stroke NNT = 46. Endpoint (%) Prasugrel. This slide depicts the balance of efficacy and safety observed in the trial. At the top is shown the significant reduction in the primary endpoint as presented a few moments ago. The number needed to treat to prevent one event was 46. At the bottom is the rate of TIMI major non CABG bleeds--a key safety endpoint-- which was 2.4% with prasugrel and 1.8% with clopidogrel—a 0.6% Absolute risk increase. The excess of 35 major bleeds with prasugrel corresponded to an HR of 1.32 and P value of The number of subjects who would need to be treated to result in one excess major bleed (NNH) was events. TIMI Major NonCABG Bleeds. Prasugrel HR 1.32 ( ) P= Clopidogrel. NNH = Adapted with permission from Wiviott SD et al NEJM 357:2007. Days")
11
Timing of Benefit (Landmark Analysis)
8 6.9 Clopidogrel Clopidogrel 6 5.6 5.6 Primary Endpoint (%) 4.7 4 Prasugrel Prasugrel HR 0.82 P=0.01 HR 0.80 P=0.003 2 1 1 2 3 30 60 90 180 270 360 450 Days Loading Dose Maintenance Dose 11
 Prasugrel. Prasugrel. HR 0.82 P=0.01. HR 0.80 P= Days. Loading Dose. Maintenance Dose. 11.")
12
CV Death, MI, Stroke Major Subgroups
TRITON TIMI-38 Reduction in risk (%) 18 UA/NSTEMI B 21 STEMI Male 21 Female 12 <65 25 Age 65-74 14 >75 6 No DM 14 DM 30 BMS 20 DES 18 The beneficial effect of prasugrel on the primary end point was consistent across key prespecified major subgroups. Notable observations include: A significant benefit in both the UA/NSTEMI and STEMI cohorts There was a consistent reduction in events with prasugrel in men and women, pts with and without diabetes, those treated with either a BMS or DES whether or not a GPI was administered and regardless of the degree of renal function All P values in tests for interaction for the subgroups described were negative. Not depicted on the slide are the data showing a reduction in events with prasugrel regardless of the timing of the LD GPI 21 No GPI 16 14 CrCl < 60 20 CrCl > 60 19 Pinter = NS OVERALL 0.5 Clopidogrel Better Prasugrel Better 1 2 Wiviott SD et al NEJM 357: 2001, 2007 HR 12 12 12
 18. UA/NSTEMI. B. 21. STEMI. Male. 21. Female. 12. < Age > No DM. 14. DM. 30. BMS. 20. DES. 18. The beneficial effect of prasugrel on the primary end point was consistent across key prespecified major subgroups. Notable observations include: A significant benefit in both the UA/NSTEMI and STEMI cohorts. There was a consistent reduction in events with prasugrel. in men and women, pts with and without diabetes, those treated with either a BMS or DES. whether or not a GPI was administered and regardless of the degree of renal function. All P values in tests for interaction for the subgroups described were negative. Not depicted on the slide are the data showing a reduction in events with prasugrel regardless of the timing of the LD. GPI. 21. No GPI CrCl < CrCl > Pinter = NS. OVERALL Clopidogrel Better. Prasugrel Better Wiviott SD et al NEJM 357: 2001, HR")
13
Principali risultati nello studio TRITON TIMI 38

14
TRITON: Previous STOKE or TIA (3.8%)
1414 L i n k 5 : T R I T O N T I M I 3 8 TRITON: Previous STOKE or TIA (3.8%) Wiviot SD et al. N Engl J Med 2007;357:
 Wiviot SD et al. N Engl J Med 2007;357:")
15
PLATO study design UA/NSTEMI (moderate-to-high risk) STEMI (if primary PCI) All receiving ASA; clopidogrel-treated or -naive; randomised within 24 hours of index event (N=18,624) Clopidogrel If pre-treated, no additional loading dose; if naive, standard 300 mg loading dose, then 75 mg qd maintenance; (additional 300 mg allowed pre PCI) Ticagrelor 180 mg loading dose, then 90 mg bid maintenance; (additional 90 mg pre-PCI) 6–12-month exposure Primary endpoint: • CV death + MI + Stroke Key secondary: • CV death + MI + Stroke in patients intended for invasive management • Total mortality + MI + Stroke • CV death + MI + Stroke + recurrent ischaemia + TIA + arterial thrombotic events • MI alone / CV death alone / Stroke alone / Total mortality Primary safety: • Total major bleeding UA = unstable angina; PCI = percutaneous coronary intervention; ASA = acetylsalicylic acid; CV = cardiovascular; TIA = transient ischaemic attack James S et al. Am Heart J 2009;157:
 Clopidogrel. If pre-treated, no additional loading dose; if naive, standard 300 mg loading dose, then 75 mg qd maintenance; (additional 300 mg allowed pre PCI) Ticagrelor. 180 mg loading dose, then. 90 mg bid maintenance; (additional 90 mg pre-PCI) 6–12-month exposure. Primary endpoint: • CV death + MI + Stroke. Key secondary: • CV death + MI + Stroke in patients intended for invasive management. • Total mortality + MI + Stroke. • CV death + MI + Stroke + recurrent ischaemia + TIA + arterial thrombotic events. • MI alone / CV death alone / Stroke alone / Total mortality. Primary safety: • Total major bleeding. UA = unstable angina; PCI = percutaneous coronary intervention; ASA = acetylsalicylic acid; CV = cardiovascular; TIA = transient ischaemic attack. James S et al. Am Heart J 2009;157:")
16
Cumulative incidence (%) Days after randomisation
K-M estimate of time to first primary efficacy event (Composite of CV death, MI or stroke) Completeness of follow-up 99.97% = five patients lost to follow-up 13 12 Clopidogrel 11.7 11 10 9.8 9 Ticagrelor 8 7 Cumulative incidence (%) 6 5 4 3 2 1 HR 0.84 (95% CI 0.77–0.92), p=0.0003 60 120 180 240 300 360 Days after randomisation No. at risk Ticagrelor 9,333 8,628 8,460 8,219 6,743 5,161 4,147 Clopidogrel 9,291 8,521 8,362 8,124 6,743 5,096 4,047 K-M = Kaplan-Meier; HR = hazard ratio; CI = confidence interval Wallentin L, Harrington R et al. New Engl J Med 2009;361 ( /NEJMoa ).
 Completeness of follow-up 99.97% = five patients lost to follow-up Clopidogrel Ticagrelor Cumulative incidence (%) HR 0.84 (95% CI 0.77–0.92), p= Days after randomisation. No. at risk. Ticagrelor. 9,333. 8,628. 8,460. 8,219. 6,743. 5,161. 4,147. Clopidogrel. 9,291. 8,521. 8,362. 8,124. 6,743. 5,096. 4,047. K-M = Kaplan-Meier; HR = hazard ratio; CI = confidence interval. Wallentin L, Harrington R et al. New Engl J Med 2009;361 ( /NEJMoa ).")
17
Hierarchical testing of major efficacy endpoints
All patients* Ticagrelor (n=9,333) Clopidogrel (n=9,291) HR for ticagrelor (95% CI) P Value† Primary objective, n (%) CV death + MI + stroke 864 (9.8) 1,014 (11.7) 0.84 (0.77–0.92) <0.001 Secondary objectives, n (%) Total death + MI + stroke CV death + MI + stroke + ischaemia + TIA + arterial thrombotic events Myocardial infarction CV death Stroke 901 (10.2) 1,290 (14.6) 504 (5.8) 353 (4.0) 125 (1.5) 1,065 (12.3) 1,456 (16.7) 593 (6.9) 442 (5.1) 106 (1.3) 0.88 (0.81–0.95) 0.84 (0.75–0.95) 0.79 (0.69–0.91) 1.17 (0.91–1.52) 0.005 0.001 0.22 Total death 399 (4.5) 506 (5.9) 0.78 (0.69–0.89) *The percentages are K-M estimates of the rate of the endpoint at 12 months. Patients could have had more than one type of endpoint. Death from CV causes included fatal bleeding and only traumatic fatal bleeds were excluded from the CV death category; †By Cox regression analysis Wallentin L, Harrington R et al. New Engl J Med 2009;361 ( /NEJMoa ).
 Clopidogrel. (n=9,291) HR for ticagrelor. (95% CI) P Value† Primary objective, n (%) CV death + MI + stroke. 864 (9.8) 1,014 (11.7) 0.84 (0.77–0.92) < Secondary objectives, n (%) Total death + MI + stroke. CV death + MI + stroke + ischaemia + TIA + arterial. thrombotic events. Myocardial infarction. CV death. Stroke. 901 (10.2) 1,290 (14.6) 504 (5.8) 353 (4.0) 125 (1.5) 1,065 (12.3) 1,456 (16.7) 593 (6.9) 442 (5.1) 106 (1.3) 0.88 (0.81–0.95) 0.84 (0.75–0.95) 0.79 (0.69–0.91) 1.17 (0.91–1.52) Total death. 399 (4.5) 506 (5.9) 0.78 (0.69–0.89) *The percentages are K-M estimates of the rate of the endpoint at 12 months. Patients could have had more than one type of endpoint. Death from CV causes included fatal bleeding and only traumatic fatal bleeds were excluded from the CV death category; †By Cox regression analysis. Wallentin L, Harrington R et al. New Engl J Med 2009;361 ( /NEJMoa ).")
18
Time to death/myocardial infarction/stroke
13 12.3 12 Clopidogrel 11 10 10.2 9 Ticagrelor 8 7 K-M estimated rate (% per year) 6 5 4 3 2 1 HR 0.84 (95% CI 0.77–0.92), p=0.0001 60 120 180 240 300 360 Days after randomisation No. at risk Ticagrelor 9,333 8,628 8,460 8,219 6,743 5,161 4,147 Clopidogrel 9,291 8,521 8,361 8,124 6,650 5,096 4,047 Wallentin L, Harrington R et al. New Engl J Med 2009;361 ( /NEJMoa ).
 HR 0.84 (95% CI 0.77–0.92), p= Days after randomisation. No. at risk. Ticagrelor. 9,333. 8,628. 8,460. 8,219. 6,743. 5,161. 4,147. Clopidogrel. 9,291. 8,521. 8,361. 8,124. 6,650. 5,096. 4,047. Wallentin L, Harrington R et al. New Engl J Med 2009;361 ( /NEJMoa ).")
19
Time to myocardial infarction
7 6.9 Clopidogrel 6 5.8 5 Ticagrelor 4 K-M estimated rate (% per year) 3 2 1 HR 0.84 (95% CI 0.75–0.95), p=0.005 60 120 180 240 300 360 Days after randomisation No. at risk Ticagrelor 9,333 8,678 8,520 8,279 6,796 5,210 4,191 Clopidogrel 9,291 8,560 8,405 8,177 6,703 5,136 4,109 Wallentin L, Harrington R et al. New Engl J Med 2009;361 ( /NEJMoa ).
 HR 0.84 (95% CI 0.75–0.95), p= Days after randomisation. No. at risk. Ticagrelor. 9,333. 8,678. 8,520. 8,279. 6,796. 5,210. 4,191. Clopidogrel. 9,291. 8,560. 8,405. 8,177. 6,703. 5,136. 4,109. Wallentin L, Harrington R et al. New Engl J Med 2009;361 ( /NEJMoa ).")
20
Time to cardiovascular death
7 6 Clopidogrel 5 5.1 4 4.0 K-M estimated rate (% per year) Ticagrelor 3 2 1 HR 0.79 (95% CI 0.69–0.91), p=0.001 60 120 180 240 300 360 Days after randomisation No. at risk Ticagrelor 9,333 8,294 8,822 8,626 7,119 5,482 4,419 Clopidogrel 9,291 865 8,780 8,589 7,079 5,441 4,364 Wallentin L, Harrington R et al. New Engl J Med 2009;361 ( /NEJMoa ).
 Ticagrelor HR 0.79 (95% CI 0.69–0.91), p= Days after randomisation. No. at risk. Ticagrelor. 9,333. 8,294. 8,822. 8,626. 7,119. 5,482. 4,419. Clopidogrel. 9, ,780. 8,589. 7,079. 5,441. 4,364. Wallentin L, Harrington R et al. New Engl J Med 2009;361 ( /NEJMoa ).")
21
End point primario nei pazienti dello studio PLATO
2121 Link 9: PLATO STEMI End point primario nei pazienti dello studio PLATO avviati all’angioplastica primaria CV death, MI, stroke (%) Steg G et al. Circulation. 2010;122:
 Steg G et al. Circulation. 2010;122:")
22
PLATO Conservative Arm
James et Al. BMJ 2011

23
PLATO Major Bleeding* (STEMI)
2323 PLATO Major Bleeding* (STEMI) Link 9: PLATO STEMI * PLATO major bleeding was defined as significant disabling bleeding, a fall in hemoglobin of ≥3 g/dL or a need for transfusion of ≥2 U red cells. Steg G et al. Circulation. 2010;122:
 Link 9: PLATO STEMI. * PLATO major bleeding was defined as significant disabling bleeding, a fall in hemoglobin of ≥3 g/dL or a need for transfusion of ≥2 U red cells. Steg G et al. Circulation. 2010;122:")
24
K-M estimated rate (% per year) PLATO life-threatening/ fatal bleeding
Total major bleeding 13 NS Ticagrelor Clopidogrel 12 11.6 11.2 11 NS 10 NS 8.9 8.9 9 7.9 8 7.7 7 NS K-M estimated rate (% per year) 5.8 5.8 6 5 4 3 2 NS 1 0.3 0.3 PLATO major bleeding TIMI major bleeding Red cell transfusion * PLATO life-threatening/ fatal bleeding Fatal bleeding Major bleeding and major or minor bleeding according to TIMI criteria refer to nonadjudicated events analyzed with the use of a statistically programmed analysis in accordance with definition described in (Wiviott SD et al. NEJM. 357: ); *Proportion of patients (%); NS = not significant Wallentin L et al. N Engl J Med Sep 10;361(11):
 NS PLATO major bleeding. TIMI major bleeding. Red cell transfusion * PLATO life-threatening/ fatal bleeding. Fatal bleeding. Major bleeding and major or minor bleeding according to TIMI criteria refer to nonadjudicated events analyzed with the use of a statistically programmed analysis in accordance with definition described in (Wiviott SD et al. NEJM. 357: ); *Proportion of patients (%); NS = not significant. Wallentin L et al. N Engl J Med Sep 10;361(11):")
25
Non-CABG and CABG-related major bleeding
9 NS Ticagrelor Clopidogrel 7.9 8 7.4 7 NS 5.8 6 5.3 p=0.0264 5 4.5 K-M estimated rate (% per year) 4 3.8 p=0.0246 2.8 3 2.2 2 1 Non-CABG PLATO major bleeding Non-CABG TIMI major bleeding CABG PLATO major bleeding CABG TIMI major bleeding Wallentin L et al. N Engl J Med Sep 10;361(11):
 p= Non-CABG PLATO major bleeding. Non-CABG TIMI major bleeding. CABG PLATO major bleeding. CABG TIMI major bleeding. Wallentin L et al. N Engl J Med Sep 10;361(11):")
26
Dyspnoea All patients Ticagrelor (n=9,235) Clopidogrel (n=9,186)
HR for ticagrelor (95% CI) P Value Dyspnoea*, % Any dyspnoea adverse event Discontinued due to dyspnoea 13.8 0.9 7.8 0.1 1.84 (1.68–2.02) 6.12 (3.41–11.01) <0.001 * Combined incidence of dyspnoea, dyspnoea at rest, dyspnoea exertional, dyspnoea paroxysmal nocturnal and nocturnal dyspnoea Wallentin L et al. N Engl J Med Sep 10;361(11):
 P Value. Dyspnoea*, % Any dyspnoea adverse event. Discontinued due to dyspnoea (1.68–2.02) 6.12 (3.41–11.01) < * Combined incidence of dyspnoea, dyspnoea at rest, dyspnoea exertional, dyspnoea paroxysmal nocturnal and nocturnal dyspnoea. Wallentin L et al. N Engl J Med Sep 10;361(11):")
27
Holter monitoring program
Holter monitor first week Ticagrelor (n=1,451) Clopidogrel (n=1,415) P Value Ventricular pauses ≥3 seconds, n (%) Ventricular pauses ≥5 seconds, n (%) 84 (5.8) 29 (2.0) 51 (3.6) 17 (1.2) 0.01 0.10 Holter monitor at 30 days (n= 985) (n=1,006) 21 (2.1) 8 (0.8) 17 (1.7) 6 (0.6) 0.52 0.60 Patients with Ventricular Pauses ≥3 seconds (n=89) (n=62) Patients with symptomatic pauses, n (%) 4 (4.5) 8 (12.9) 0.06 Wallentin L et al. N Engl J Med Sep 10;361(11):
 Clopidogrel. (n=1,415) P Value. Ventricular pauses ≥3 seconds, n (%) Ventricular pauses ≥5 seconds, n (%) 84 (5.8) 29 (2.0) 51 (3.6) 17 (1.2) Holter monitor at 30 days. (n= 985) (n=1,006) 21 (2.1) 8 (0.8) 17 (1.7) 6 (0.6) Patients with Ventricular Pauses ≥3 seconds. (n=89) (n=62) Patients with symptomatic pauses, n (%) 4 (4.5) 8 (12.9) Wallentin L et al. N Engl J Med Sep 10;361(11):")
28
Other findings All patients Ticagrelor (n=9,235) Clopidogrel (n=9,186) P Value* Serum creatinine (% increase from baseline value), mean SD During treatment Follow-up visit 10 22 8 21 <0.001 0.59 * P-values were calculated with the use of Fischer’s exact test Wallentin L et al. N Engl J Med Sep 10;361(11):
:")
29
Ticagrelor is a more effective alternative than clopidogrel
Conclusions Reversible, more intense P2Y12 receptor inhibition for one year with ticagrelor in comparison with clopidogrel in a broad population with STEMI and NSTEMI ACS provides Reduction in MI and stent thrombosis Reduction in CV and total mortality No change in the overall risk of major bleeding Raised risk for non-procedure-related bleeding Ticagrelor is a more effective alternative than clopidogrel for the continuous prevention of ischaemic events, stent thrombosis and death in the acute and long-term treatment of patients with ACS

30
Risultati principali TRITON morte CV, IM, CVA 9.9 vs 12.1%, RRR -19%
NNT 46 CABG related bleeding NNH 10 PLATO morte cause vascolari, IM,CVA 9.8 vs 11.7%, RRR -16% NNT 53

31
Platelets and Coronary Thrombosis
Le piastrine hanno un ruolo chiave nella formazione del trombo in corrispondenza di una placca aterosclerotica vulnerabile che si e’ instabilizzata: La crescita rapida del trombo piastrinico all’interno di un’impalcatura fibrinica che lo stabilizza, puo’ condurre all’occlusione trombotica completa del vaso Coronary plaque Erosion/rupture Thrombotic occlusion Davies MJ. Am J Cardiol Aug 16;88(4A):2F-9F 31
:2F-9F. 31.")
32
Adesione piastrinica Lisman et Al. Frontiers in Bioscience ,2005
Schematic representation of adhesion and aggregation under flow conditions. A) Rolling of over -bound vWF mediated by GPIb. B) Firm attachment mediated by alpha(2)beta(1) and glycoprotein VI (GP VI) to , and by alpha(IIb)beta(3) to -bound vWF. C) , , and spreading. D) Aggregate formation. Lisman et Al. Frontiers in Bioscience ,2005
 Rolling of over -bound vWF mediated by GPIb. B) Firm attachment mediated by alpha(2)beta(1) and glycoprotein VI (GP VI) to , and by alpha(IIb)beta(3) to -bound vWF. C) , , and spreading. D) Aggregate formation. Lisman et Al. Frontiers in Bioscience ,2005.")
33
Meccanismi di attivazione piastrinica
Wallentine L. Eur Heart J 2009

35
Limitations of clopidogrel
Slow onset of action (steady state platelet inhibition: hour after mg load) Modest inhibition of platelet aggregation (steady state mean platelet inhibition %) Slow offset of effect (at least 5 – 7 days) Large interindividual variability in inhibition of platelet aggregation (poor platelet inhibition response in % of pts) Come tutti ben sappiamo, il clopidogrel è una delle pietre angolari nella prevenzione dell’aterotrombosi. Sfortunatamente il clopidogrel, che insieme all’aspirina è il farmaco più utlizzato in questo settore, ha delle importanti limitazioni: Problema nelle prime ore delle sindromi coronariche acute quando il rischio trombotico è più alto Efficacia antiapiastrinica non elevata e soprattutto con notevole variabilità interindividuale Questo preoccupa nei pazienti ad elevato rischio di sanguinamento
 Modest inhibition of platelet aggregation (steady state mean platelet inhibition %) Slow offset of effect (at least 5 – 7 days) Large interindividual variability in inhibition of platelet aggregation (poor platelet inhibition response in % of pts) Come tutti ben sappiamo, il clopidogrel è una delle pietre angolari nella prevenzione dell’aterotrombosi. Sfortunatamente il clopidogrel, che insieme all’aspirina è il farmaco più utlizzato in questo settore, ha delle importanti limitazioni: Problema nelle prime ore delle sindromi coronariche acute quando il rischio trombotico è più alto. Efficacia antiapiastrinica non elevata e soprattutto con notevole variabilità interindividuale. Questo preoccupa nei pazienti ad elevato rischio di sanguinamento.")
36
Clopidogrel Response Variability Baseline - 2hr (5mol ADP)
Resistance = 63% Number of patients ≤ -30 -20, -10 0, 10 20, 30 40, 50 60, 70 > 80 -30, -20 -10, 0 10, 20 30, 40 50, 60 70, 80 ∆ percent aggregation Gurbel PA et al. Circulation 2003; 107:2908

37
Major pathways leading to the formation of thienopyridine active metabolites
Wallentine L. Eur Heart J 2009

38
Genetic effects on pharmacokinetic responses to clopidogrel
Percent difference in AUCo-t 162 healthy subjects -32.4 -6.8 -15.7 5.6 11.2 p value <0.001 0.59 0.03 0.45 CYP2C19 CYP2C9 CYP2B6 CYP3A5 CYP1A2 -50 -40 -30 -20 -10 10 20 30 Relative Percent Difference Mega J L et al, N Engll J Med 2009; 360:

39
Cytochrome P450 2C 19 polymorphism
Time course of ex-vivo platelet aggregation in response to 10 μM ADP Clopidogrel 75 mg/d 90 80 70 ADP 10 μmol/L-induced Platelet aggregation (%) 60 P <0.003 50 CYP2C19 genotype *1/*1 CYP2C19 genotype *1/*2 40 1 2 3 4 5 6 7 8 9 10 11 12 13 14 Time (Days) Hulot et al. Blood 2006; 108:
 60. P < CYP2C19 genotype *1/*1. CYP2C19 genotype *1/* Time (Days) Hulot et al. Blood 2006; 108:")
40
CYP2C19*2 polymorphism in young MI patients treated with clopidogrel
The AFIJI Multicentre Registry (n= 259) Kaplan Maier estimates of the rates of first cardiovascular event at 5years of follow-up 1 0.9 0.8 0.7 HR 3.69 (95% CI ) p=0.0005 0.6 Cumulative event- free survival (%) 0.5 Non carriers Carriers 0.4 1 2 3 4 5 Follow-up duration (years) Collet JP, et al, Lancet 2009; 373:
 Kaplan Maier estimates of the rates of first cardiovascular event at 5years of follow-up HR 3.69 (95% CI ) p= Cumulative event- free survival (%) 0.5. Non carriers. Carriers Follow-up duration (years) Collet JP, et al, Lancet 2009; 373:")
41
Cytochrome P450 2C19 polymorphism and stent thrombosis
2485 patients undergoing PCI and treated with clopidogrel p=0.002 30-day incidence of stent thrombosis (%) CYP2C19 *1/*1 CYP2C19 *1/*2 CYP2C19 *2/*2 Sibbing et al, Eur Heart Journal 2009; 30:
 CYP2C19. *1/*1. CYP2C19. *1/*2. CYP2C19. *2/*2. Sibbing et al, Eur Heart Journal 2009; 30:")
42
Attività piastrinica residua ed eventi cardiovascolari
prospective observational studies using the Accumetrics VerifyNow P2Y12 assay Price M et Al. Circulation 2011

43
Kaplan Meier Survival Curves
1789 Pazienti consecutivi 14% HRPP 14.6% 8.7% 9.7% 4.3% Cardiac death, myocardial infarction, any urgent coronary revascularization, and stroke at 2-year follow up Parodi G et Al. JAMA 2011

44
Two-year clinical outcome
Parodi G et Al. JAMA 2011

45
Analisi dei risultati Parodi G et Al. JAMA 2011

46
Verify-now LTA ADP WDA ADP PFA 100

47
ESC Guideline 2011

48
Antiplatelets Drug metabolism
F S O Ticagrelor N S O F Prasugrel Clopidogrel N S O CI No in vivo biotransformation Active compoud Intermediate metabolite Prodrug CYP-dependent oxidation CYP3A4/5 CYP2B6 CYP2C19 CYP2C9 CYP2D6 Binding Ticagrelor Hydrolysis by esterase Platelet Prasugrel P2Y12 Clopidogrel CYP-dependent oxidation CYP1A2 CYP2B6 CYP2C19 CYP-dependent oxidation CYP2C19 CYP3A4/5 CYP2B6

49
Diverso meccanismo d’azione degli inibitori del recettore P2Y12
Il ticagrelor e’ un potente inibitore reversibile del recettore P2Y12, con un meccanismo diverso da quello delle tienopiridine. Il farmaco infatti non impedisce l’interazione tra ADP e recettore, ma disattiva il recettore medesimo, rendendo impossibile quella modificazione conformazionale che lo associa ad una serie di azioni pro-aggreganti all’interno della piastrina. Nel momento in cui il prodotto si dissocia dal recettore quest’ultimo ripristina le sue piene funzioni. Ticagrelor appartiene alla classe farmacologica delle nuove pirimidine ciclopentiltiazolo. Il ticagrelor raggiunge la massima antiaggregazione piastrinica prodotta dal farmaco (50-60%) dopo 2 h dall’assunzione di una dose di carico di 180 mg e questo livello di inibizione si mantiene con la somministrazione di 90 mg x 2/die Becker RC, Gurbel PA Thromb Haemost 2010 49
 dopo 2 h dall’assunzione di una dose di carico di 180 mg e questo livello di inibizione si mantiene con la somministrazione di 90 mg x 2/die. Becker RC, Gurbel PA Thromb Haemost")
50
New Antiplatelet Agents

51
I nuovi antiaggreganti piastrinici
Steady state Aggregazione 3-7 gg 3gg 2-3gg rapida Inizio anti- Aggreg. 2 h 30min rapida Grado di inibizione 30-50% 70-80% SI Legame reversibile NO SI Offset 5gg 4-5gg 36-48h -- Clopidogrel Prasugrel Ticagrelor Cangrelor

52
Prasugrel farmacodinamica
clopidogrel Jernberg et al, Eur Heart J 2006;27;

54
Ticagrelor Pharmacodynamics
AZD mg od AZD mg bd AZD mg bd % IPA Final AZD mg bd Clopidogrel 75mg od IPA: Inibition of Platelet Aggregation

55
Greater and More Consistent IPA with AZD6140 than Clopidogrel
Final Extent AZD mg bd Clopidogrel 100 100 80 80 60 60 Mean percent inhibition 40 40 20 20 2 4 8 12 2 4 8 12 24 2 4 8 12 2 4 8 12 24 Day 1 Day 14 Day 1 Day 14 Hours Hours

56
Circulation 2010

57
Onset and Offset of the Antiplatelet Effects
Ticagrelor vs Clopidogrel 10 20 30 40 50 60 70 80 90 100 0.5 1 2 4 8 24 48 72 120 168 240 Loading dose Last maintenance dose Ticagrelor (n=54) Clopidogrel (n=50) Placebo (n=12) Inhibition of Platelet Aggregation (IPA) percent 6 weeks Onset Maintenance Offset Time (hours) Gurbel PA et al, Circulation 2009; 120:
 Clopidogrel (n=50) Placebo (n=12) Inhibition of Platelet Aggregation (IPA) percent. 6 weeks. Onset. Maintenance. Offset. Time (hours) Gurbel PA et al, Circulation 2009; 120:")
58
Quale antiaggregante? Non esistono studi di confronto tra Prasugrel e Ticagrelor E’ possibile identificare una tipologia di paziente specifica per ciascun farmaco

59
Recent Meta-Analyses Link 11: Montalecot JACC 2010 Meta-analysis
5959 Link 11: Montalecot JACC 2010 Meta-analysis Recent Meta-Analyses Montalescot G et al. J Am Coll Cardiol 2010

60
Recent Meta-Analyses Adjusted comparison of Prasugrel vs. Ticagrelor
L i n k 1 2 : I n t J C a r d i o l L i n k 1 3 : C o m p a r i s o n o f t h e C h a r a c t e r i s t i c s ( P r a s u g r e l v s . T i c a g r e l o r ) 6060 Recent Meta-Analyses Adjusted comparison of Prasugrel vs. Ticagrelor Biondi-Zoccai G et al. Int J Cardiol 2010
 Recent Meta-Analyses. Adjusted comparison of Prasugrel vs. Ticagrelor. Biondi-Zoccai G et al. Int J Cardiol")
61
Prasugrel Azione rapida, legame irreversibile
. soggetto “giovane”, nessuna storia di accidenti CV, peso > 60Kg,* . paziente con STEMI avviato alla PCI . ACS con anatomia coronarica nota e avviato alla PCI *Non indizi di malattia che meriti BPAC

62
Ticagrelor Azione rapida , legame reversibile . Paziente con ACS
. Quadro angiografico ignoto . Clearance Creat >30 ml/min/1.73m2

64
P2Y12 reaction units (PRU) as assessed by the VerifyNow P2Y12 assay by protocol time and treatment
Gurbel PA et al, Circulation 2009; 120:

65
Effetto dello switching tra farmaci
Gurbel et Al. Circulation,2010

66
Conclusioni Una moderna terapia antiaggregante dei pazienti con malattia coronarica consente di ridurre gli eventi ischemici e la mortalità nei pazienti con SCA I nuovi antiaggreganti sono più potenti, risentono poco o nulla delle differenze individuali, e sono più efficaci rispetto al clopidogrel Poiché si associano ad un rischio emorragico maggiore la selezione dei pazienti diventa molto importante nella scelta del farmaco da utilizzare e richiede un utilizzo giudizioso soppesando il rischio trombotico e quello emorragico

68
Eseguito con il WASP

69
Reversibilità della inibizione e vantaggi potenziali
Becker RC, Gurbel PA Thromb Haemost 2010

Similar presentations







 Xu March, 2012 ACS trials. Outline – over 70 ACS trials Mangement strategy Cardiogenic shock Lytics/Referfusion Stable CAD/Elective.>")


















