Download presentation
Presentation is loading. Please wait.

1
Ovary Reserve Dr. Vincenzo Volpicelli Seconda Università degli Studi di Napoli Dipartimento di Scienze della Vita SUNfert Fertility Center Cardito

2
Ovary reserve Patient age USG: ovarian measures and number of secondary follicles (3th day) basal FSH (3th day) basal E2 (3th day) β-inhibina (3th day) MIF (3th day) Clomiphene Challenge test (CCCT) Gn-RH-a test FSH test
 basal FSH (3th day) basal E2 (3th day) β-inhibina (3th day) MIF (3th day) Clomiphene Challenge test (CCCT) Gn-RH-a test FSH test")
3
Female age is very important in consideration of probability for conception because it is very much related to egg quality. A 45 year old can have good quality eggs (for her age) and still be fertile, although this is quite uncommon. At the other extreme, a 25 year old can have very poor quality eggs and be infertile - unless she uses donor eggs. These are extreme examples, but the point is that egg quantity and quality tends to decline significantly in the 30s and faster in the early 40s, but egg quantity and quality in an individual woman can be average for her age, better than average, or worse than average.
 and still be fertile, although this is quite uncommon. At the other extreme, a 25 year old can have very poor quality eggs and be infertile - unless she uses donor eggs. These are extreme examples, but the point is that egg quantity and quality tends to decline significantly in the 30s and faster in the early 40s, but egg quantity and quality in an individual woman can be average for her age, better than average, or worse than average..")
4
median volumes of the left and right ovaries no significant differences 4.6 and 4.8 cm 3, respectively; interquartile range: 3.0–7.3 and 3.1–7.9; 3.1–7.9; P =.79 P =.79

5
Age/FSH/follicles/ovarian volume significant positive correlation between age and FSH level (R =.372, P <.001), but not between age and ovarian volume (R =.039, P =.69). A significant relation between FSH and the number of follicles (H = 20.8, P <.001), but not between FSH and volume (R =.102, P =.29). There is a significant decrease in the number of follicles and a higher cycle cancellation rate in women with volume smaller than 3 cm 3 compared with those with volume greater than 3 cm 3. The mean ovarian volume was 6.0 ± 4.7 cm3 (67).
, but not between FSH and volume (R =.102, P =.29). There is a significant decrease in the number of follicles and a higher cycle cancellation rate in women with volume smaller than 3 cm 3 compared with those with volume greater than 3 cm 3. The mean ovarian volume was 6.0 ± 4.7 cm3 (67)..")
6
Age/n. follicles red line: 37.5 years n. follicles: 25.000

7
n. follicles/patients age

9
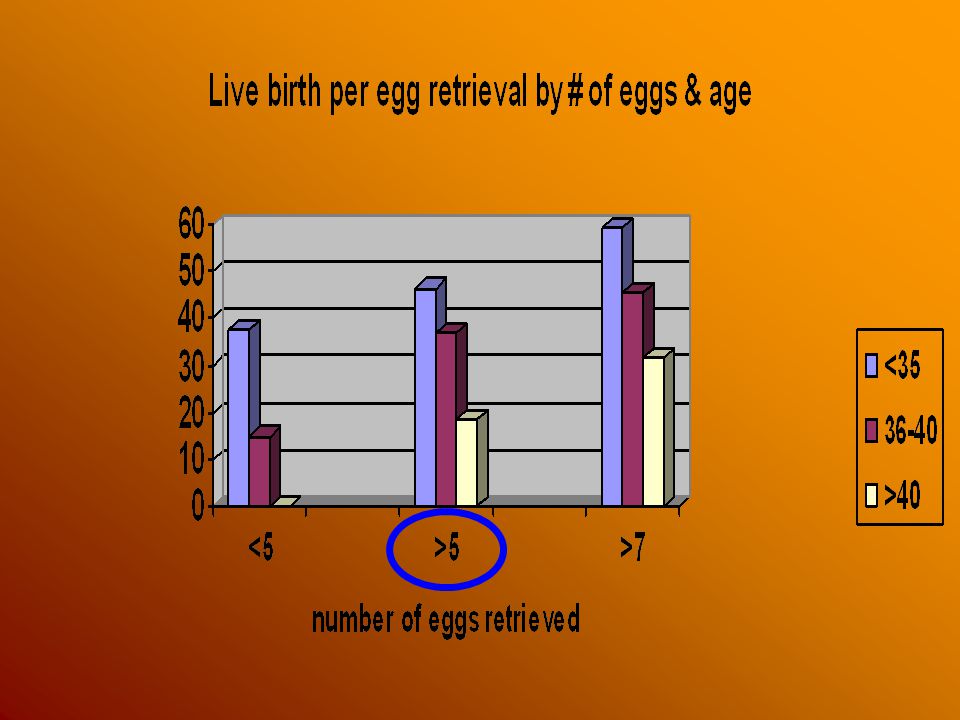
Number of eggs retrieved and IVF pregnancy and success rates according to female age The data in the graph above indicates that: Women under 35 in our IVF program (on the average) have good live birth rates, even with less than 5 eggs, and do better if we get more than 5 eggs, and best with more than 7 eggs Women 35-39 (on the average) have low live birth rates with less than 5 eggs, which are substantially better with 5-7, and best with more than 7 eggs Women 40-42 do very poorly if we get less than 5 eggs, have reasonable live birth rates with 5-7 eggs, and best with more than 7 eggs This is another example of decreasing egg quality with increasing female age. As women age, we need more eggs to be able to make IVF work - because the lower quality of the eggs.

11
USG (3 th day): n. pre-antral follicles Ovarian size: V = D1 x D2 x D3 x 0.5233 (v.n. 12.77 ± 3.75) Cortical/medullar rate (v.n. 1.26 ± 0.27)
 Cortical/medullar rate (v.n ± 0.27).")
12
Number of eggs retrieved and IVF pregnancy success rates according to female age antral follicles count is the best predictor of the response that the ovaries will give, and the number of eggs that will be retrieved. To some extent, the more eggs we have to work with, the greater the chance that IVF will be successful. There are several issues involved with this: 1. 1.More eggs - will give more fertlized eggs 2. 2.More embryos for E-T 3. 3.Women that respond well to the drugs sometimes will also have better quality eggs as well - which will be more likely to develop into quality embryos

13
Day 3 FSH level Interpretation (DPC Immulite only) Less than 9 Reassuring level. Expect a good response to ovarian stimulation. 9 - 10 Fair. Response is between completely normal and somewhat reduced (response varies widely). Overall, a somewhat reduced live birth rate. 10 - 12 Reduced ovarian reserve. Usually show a reduced response to stimulation and some reduction in egg and embryo quality with IVF. Reduced live birth rates on the average. 12 - 17 Generally show a more marked reduction in response to stimulation and usually a further reduction in egg and embryo quality with IVF. Low live birth rates. Over 17 "No go" level. Very poor (or no) response to stimulation. No live births. "No go" levels must be individualized for the particular lab assay and IVF center. Day 3 FSH level
. Overall, a somewhat reduced live birth rate Reduced ovarian reserve. Usually show a reduced response to stimulation and some reduction in egg and embryo quality with IVF. Reduced live birth rates on the average Generally show a more marked reduction in response to stimulation and usually a further reduction in egg and embryo quality with IVF. Low live birth rates. Over 17 No go level. Very poor (or no) response to stimulation. No live births. No go levels must be individualized for the particular lab assay and IVF center. Day 3 FSH level.")
14
Some caveats about day 3 FSH testing In general, ovarian reserve and egg quantity is as bad as worst FSH. If you have an FSH of 15 in one cycle and have it repeated in another cycle and get a 7 - the situation is not improving. Some women do "bounce around" with FSH levels in the normal to abnormal range - but they will generally respond and have chances for pregnancy more like those women who are consistently at their higher FSH level. Waiting for a menstrual cycle with a lower FSH level and then stimulating quickly for IVF is probably of no benefit at all. Young (e.g. under 35) women with elevated FSH levels stimulate better and have a higher pregnancy potential than "older" women.
 women with elevated FSH levels stimulate better and have a higher pregnancy potential than older women..")
15
BASAL FSH BASAL FSH Receiver operating characteristic curve of studies reporting on the performance of basal FSH to predict poor ovarian response. Bancsi. Metanalysis of basal FSH. Fertil Steril 2003.

16
Day 3 estradiol relatively new about 80 pg/ml "masking" the poor ovarian reserve

17
Day 3 estradiol Moderately elevated day-3 FSH levels (>13 IU/ml) predict egg lower quantity better than egg quality M. Luna-Rojas, L. Grunfeld, B. Sandler, M. Duke, A.B. Copperman, J. Barritt Fertility and Sterility September 2004 (Vol. 82, Page S127)
.")
18
β-inhibin β-inhibin (granulosa cells): <45 pg/ml PR 28% 45 pg/ml PR 95% very low in women over 35 of age
: <45 pg/ml PR 28% 45 pg/ml PR 95% very low in women over 35 of age")
19
β -inhibin physiology FSH + + + IGF-1 + + + Gn- RH - - - In turn, inhibin suppresses FSH

20
β -inhibin values <45 pg/ml PR 28% 45 pg/ml PR 95% over 35 and endometriosi

21
Clomiphene challenge test CCCT is a dynamic type of test that can discover some cases of poor ovarian reserve that are still showing a normal day 3 FSH. hypothalamic-hypophysial- ovarian axis completeness

22
Clomiphene challenge test This test is done by: 1. Obtaining a day 3 FSH and estradiol 1. Obtaining a day 3 FSH and estradiol 2. The woman takes two tablets of clomiphene (100 mg) on days 5-9 of the cycle 2. The woman takes two tablets of clomiphene (100 mg) on days 5-9 of the cycle 3. Repeat an FSH level on day 10 of the cycle 3. Repeat an FSH level on day 10 of the cycle The normal test would show: –a low FSH, LH and E 2 on day 3 –more 2 increased FSH, LH and E 2 on day 10
 on days 5-9 of the cycle 2. The woman takes two tablets of clomiphene (100 mg) on days 5-9 of the cycle 3. Repeat an FSH level on day 10 of the cycle 3. Repeat an FSH level on day 10 of the cycle The normal test would show: –a low FSH, LH and E 2 on day 3 –more 2 increased FSH, LH and E 2 on day 10.")
23
Clomiphene challenge test Expected Values: cycle day 3 E2 65- 70 FSH <10 cycle day 10-11 LH <10 FSH <10

24
Response to to ovarian stimulation with FSH and antral follicles count This is not really a "test" that we do to help us determine egg quantity and quality - it is part of a treatment for infertility. However, the response of the ovaries when the woman takes injectable FSH for stimulation is often very predictive of the egg quantity and, therefore, also the relative chances for success with infertility treatment. injectable FSHinjectable FSH Response to stimulation and antral follicle countsResponse to stimulation and antral follicle counts are important predictors of outcome, and are discussed in detail on the next slide. Response to stimulation and antral follicle counts

25
Response to ovarian stimulation with FSH and E 2 testing 75 UI FSH injection on day 3 testing both the baseline and 24 hour post-injection estradiol If the estradiol response and antral follicle number are poor, ovarian reserve and egg quantity are also likely to be poor.

26
Gn-RH-a test/E 2 rising Pattern A: early rising followed by fall of estradiol level after 4 days Pattern B: estradiol slow rising and slow fall on 6 th day Pattern C: persistent estradiol rising Pattern D: no answer

27
Gn-RH-a pattern/PR

28
Poor response the devil is in the definition The original definition of low response to ovarian response by Garcia et Acosta was based on low peak E2 concentrations alone. They stimulated patients with hMG (150 IU IM daily) and defined low responders as patients with a peak E2 concentration of <300 pg/mL
 and defined low responders as patients with a peak E2 concentration of <300 pg/mL.")
29
Poor responders diminished ovarian reserve E 2 < 500 pg/mL on day of hCG <4 de Graaf follicles on day of hCG lower fertilization rates lower cleavage rates lower resulting embryos lower pregnancy rates

30
THE END

Similar presentations













: Stimulates growth of ovarian follicles, and estrogen.>")





