Download presentation
Presentation is loading. Please wait.

1
Laser treatment in glaucoma
H-Attarzadeh MD. Associate professor of ophthalmology Isfahan university of medical sciences

2
Laser surgical treatment in glaucoma
Laser trabeculoplasty Laser peripheral iridotomy Laser iridoplasty Laser cyclophotocoagulation

3
Laser trabeculoplasty
In the early 1970s attempts were made to use argon laser energy to puncture through TM into Schlemm,s canal, which was unsuccesful. In 1979, Wise and Witter used non-penetrating laser energy in the TM and found that they were able to lower IOP for a prolonged period.

4
Mechanism It is not entirely clear.
Thinning and scarring of the TM at the site of laser treatment. The spaces between the laser spots are widened and free of debris. The initial theory is that a mechanical tightening of the terabecular ring increased aqueous outflow.

5
Indications for laser terabeculoplasty
Effective in the treatment of the following: 1- primary open-angle glaucoma 2- exfoliative glaucoma 3- pigmentary glaucoma

6
Less effective in the treatment of the following
Aphakic eyes Pseudophakic eyes

7
Unlikely to be effective in the treatment of the following
Angle-recession glaucoma Inflammatory glaucoma Congenital/developmental glaucoma Juvenile glaucoma

8
Not possible in the treatment of the following
Synechial angle closure such as: Neovascular glaucoma and ICE syndrome

9
Technique of laser terabeculoplasty
Wavelength :Argon green or blue-green Spot size: 50 micron Duration: 0.1 second Power: mW Applications: spots per 180 degree or spots / 360 degree Lens: Goldmann 3-mirror or equivalent

10
General considerations
In lightly pigmented angles a beginning power of mw is reasonable. In heavily pigmented angles, lower powers such as mw should be used. Postoperative IOP spikes are especially worrisome in patients with marked angle pigmentation or advanced optic nerve head damage.

11
The aiming beam should be directed at the junction between the pigmented and non-pigmented TM.
Patients are usually seen 1 or 2 hours after the LTP to ensure that no postoperative IOP rise has occurred. Topical corticosteroids should be used 4 times a day for 4 days in addition to the preexisting glaucoma medications.

12
The typical tissue response to LTP is a blanching of the TM, often associated with a small gas bubble. The bubbles are transient, but the blanching may persist for several days.

14
Complications LTP is an extremely safe procedure.
The most common complication is an elevated IOP which occur in 20% of cases. Transient corneal opacities, mild iritis, peripheral anterior synechiae

16
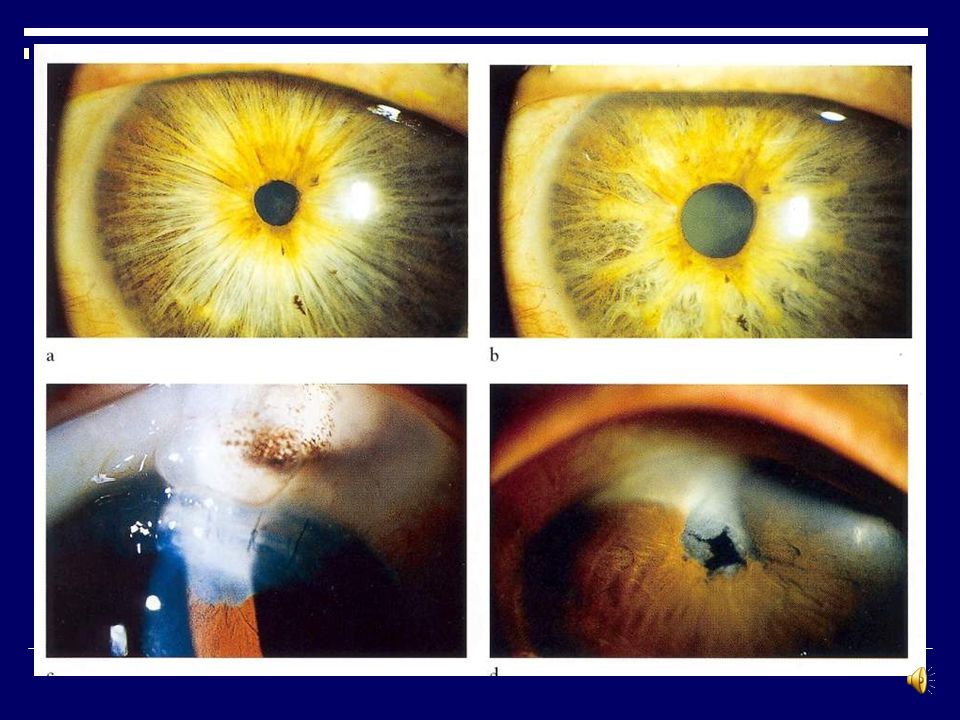
Laser peripheral iridotomy
LPI was first introduced in 1956, but it become popularized with the advent of the argon laser and more recently the Nd:YAG This technology has almost totally replaced surgical iridectomy.

17
Indications Acute angle closure glaucoma
Secondary pupillary block due to any reason. LPI is not helpful for synechial angle closure caused by neovascularization, ICE syndrome. LPI is used for patients at risk for developing angle closure.

18
Technique To lower the IOP in case of acute angle closure glaucoma by medication. Supranasal area is prefered. The depth of an iris crypt is a proper position.

19
Argon laser peripheral iridotomy
Spot size: 50 micron Duration: second Power: 1 W Lens: Abraham or Wise

22
Nd:YAG laser peripheral iridotomy
Spot size: fixed Duration: fixed ( nanoseconds) Energy: 1-12 j Lens: Abraham or Wise
 Energy: 1-12 j. Lens: Abraham or Wise.")
24
Postoperative management
A drop of a2-adrenergic agonist. The IOP checking 1-2 hours later. Prednisolone 4 times a day for 4 days. Preoperative glaucoma medications are to be continued. Pilocarpine should be avoided.

25
Complications Transient iritis is the most complication.
IOP elevation is common. Occasionally corneal epithelial opacities. Lens epithelial changes. Bleeding of the iris is a frequent complication. Monocular diplopia (rarely)
")
26
Laser iridoplasty Laser iridoplasty is performed on patients with plateau iris syndrome. It can be used before LTP to provide better view of the iridocorneal angle. 4 to 6 applications are applied per quadrant.

28
Argon laser iridoplasty
Spot size: mic. Duration: second Power; mw Lens: none or Goldmann 3-mirror

29
A common problem in glaucoma patients who have been on chronic miotic therapy is a markedly constricted pupil. This is especially a problem in a patient with early cataract formation. It may be possible to improve their vision by dilating the pupil with laser pupilloplasty.

30
This procedure involves the application of low energy, contraction burns in several radial row around the pupil. Standard setting are 0.2 to 0.5 second, 200 to 500 microns, and 200 to 500 mw. Postoperative complications include IOP rise and transient iritis.

31
ضمن عرض پوزش بدلیل حجم بالای LECTUER ادامه اسلایدها امکان پذیر نمیباشد در صورت نیاز به ادامه لطفا به واحد سمعی و بصری مرکز آموزشی درمانی فیض مراجعه و یا با شماره تلفن داخلی 392 تماس حاصل نمائید با تشکر

Similar presentations







 1)Noninvasive 2) non-contact imaging 3)Millimeter penetration Aproximately 2-3 mm in tissue with micrometer scale (axial.>")




 IN CORRECTING HIGH MYOPIA By: H.R. ZIAI MD. Esfand 1391 Isfahan.>")










 Endolenticular.>")
