Download presentation
Presentation is loading. Please wait.

1
Pulmonary Function Tests
Ghassan Jamaleddine, M.D. American University of Beirut

2
Use of PFT’s Evaluating breathlessness
Initial evaluation of patient with known respiratory disease Following the course of a respiratory disease Pre-operative assessment Disability evaluation Screening of subclinical disease

3
Disadvantages of PFT’s
Patient’s cooperation and an informed technician are required Measures the lung and chest as a unit Evaluates disease at only one point in time Errors in programs of computer driven automated equipment

4
Routine PFT’s Spirometry with or without Flow Volume loop
Static lung volumes Single Breath Diffusing Capacity

9
Spirometry Forced vital capacity
Forced Expiratory Volume in one second (FEV1) Percent Expired (FEV1/FVC or FEV1%) Forced Mid-Expiratory Flow (FEF 25-75) or Maximal Mid-Expiratory Flow (MMEF or MMF) Peak or Maximal Expiratory Flow Rate (PEF or MEFR)
 Percent Expired (FEV1/FVC or FEV1%) Forced Mid-Expiratory Flow (FEF 25-75) or Maximal Mid-Expiratory Flow (MMEF or MMF) Peak or Maximal Expiratory Flow Rate (PEF or MEFR)")
11
Adapted from Fletcher C, Peto R
Adapted from Fletcher C, Peto R. The natural history of chronic airflow obstruction. Br Med J 1977; 1:

12
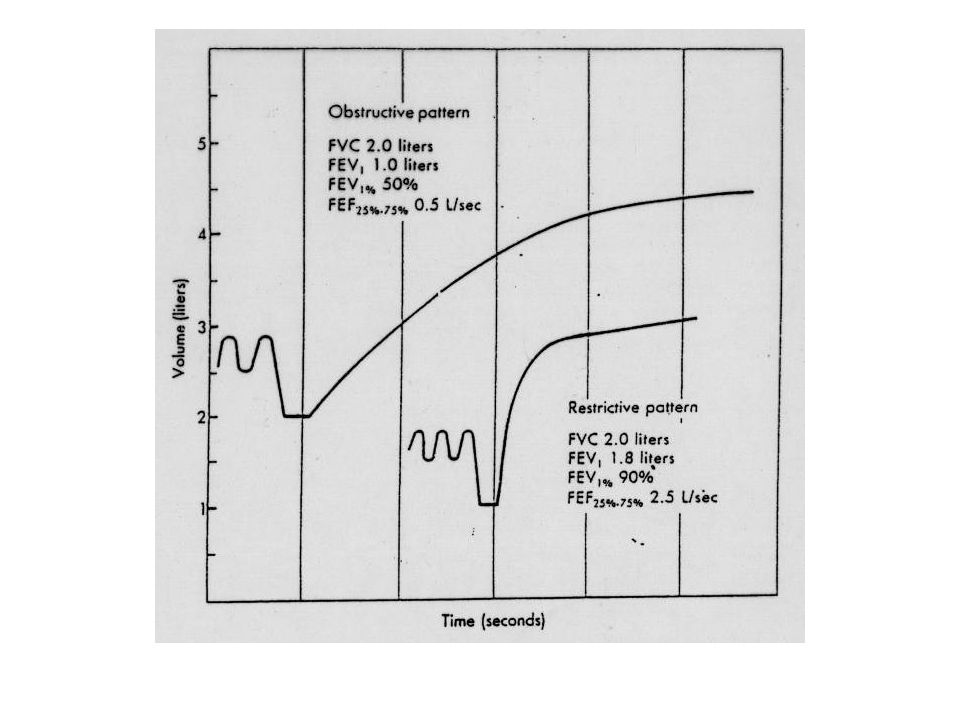
Pattern of defects seen on PFT’s
Obstructive Vent defect FVC reduced or Normal FEV1 reduced FEV1/FVC is reduced Example: Asthma, COPD Restrictive Vent defect FVC reduced FEV1 normal or reduced FEV1/FVC is increased Example: pulmonary fibrosis, pleural effusion, neuromuscular

16
P1V1 = P2 (V1-Δ V)
")
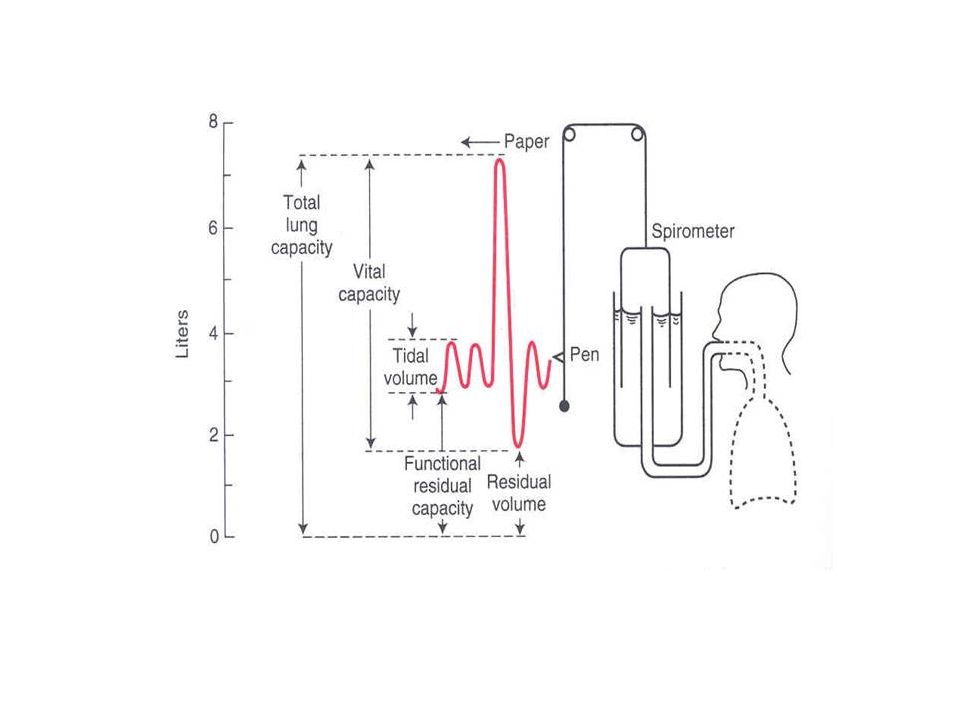
18
Lung Volumes Functional Residual Capacity Expiratory Reserve Volume
Residual Volume Inspiratory Capacity Total Lung Capacity Vital Capacity

19
FLOW VOLUME LOOP

22
Diffusion Transfer of a gas across a tissue sheet, governed by Fick’s law Rate of Transfer = A D x P/T

24
Diffusion Capacity (measurement)
A D x (P1- P2) T AD/T = Diffusion constante Rate of transfer (CO) = Vco = Dlco x (P1-P2) Dlco = Vco/ PA –Pa = Vco/ PA 25 ml/min/mmHg
 T. AD/T = Diffusion constante. Rate of transfer (CO) = Vco = Dlco x (P1-P2) Dlco = Vco/ PA –Pa = Vco/ PA. 25 ml/min/mmHg.")
25
Diffusing Capacity Influenced by:
Changes in alveolar-capillary membrane Pulmonary circulation Ventilation perfusion matching Hemoglobin concentration

26
Diffusion Capacity Very important in
Interstitial lung disease Drug induced lung injury Reduced in Emphysema because of destruction of alveolar units

27
PFT Patterns in Disease
PFT results are best interpreted with knowledge of the patients history, physical exam and occasionally chest X-ray.

28
PFT Disease Obstructive Restrictive FVC N or FEV1 FEV1/FVC N MMEF or V50 N or MVV FRC RV TLC N or

29
Case 1 14 year old boy came to ER with increasing shortness of breath
History of asthma since age of 2-3 Maintained on ICS and Beta2 agonists Followed by Family physician, past year frequent attacks, several courses of antibiotics and systemic corticosteroids

30
Case 1 (cont’d) In ER started on iv steroids and inhaled Beta 2 agonists, no improvement, admitted No history of atopy, no nasal nor GI symptoms, no family history of asthma Exam: decrease breath sounds Admitted

31
Case 1 (cont’d) CXR, CBC, chemistry non revealing
After 2 days of treatment with steroids and inhaled bronchodilators there was no improvement in symptoms Noticed faint voice and tachypnea on minimal exercise PFT obtained

32
Case PFT’s FVC 93%, FEV1 45%, FEV1/FVC 41% TLC 90%, RV 90%, DLCO 100%
?????
34
Case 1(cont’d) FOB: subglottic stenosis (? Congenital)
Tracheostomy followed by reconstructive surgery Total recovery, no more asthma treatment

35
Case 2 32 year old man presented with 2 months history of increasing shortness of breath Married, non-smoker, bank employee, no history of asthma No other symptoms Shortness of breath increasing before presentation Seen by multiple physicians, given a number of antibiotics, bronchodilators, aminophylline

36
Case 2 (Cont’d) Exam: BP 120/80, RR 18, P100, BMI 29, afebrile, chest: clear… rest of exam was normal ER: ABG’s normal, CXR: normal, CT angio: normal, neuro consult (fellow): no neuro problem Patient reassured by the team
: no neuro problem. Patient reassured by the team.")
37
Case 2 (cont’d) Spirometry obtained: FVC 50% FEV1 55% FEV1/FVC 80%
MVV 20% ????

38
Case 2 (cont’d) Neurology attending reconsulted EMG: Myasthenia Gravis
Diagnosis suspected from FVC and MVV Neuromuscular illness

39
Case 3 A 60 year old man with history of ex-smoking, history of seasonal colds, admitted for hernia operation Pulmonary consulted for pre-op clearance because of obesity The patient denied pulmonary complaints, but his wife disclosed that he has a chronic cough

40
Case 3 Predicted Values Measured Values % Predicted FVC 6.00 liters 4.00 liters 67 % FEV1 5.00 liters 2.00 liters 40 % FEV1/FVC 83 % 50 % 60 % Obstructed defect

41
Case 3

42
Pre-operative screening
Patients with known pulmonary illness or symptoms Overweight patients Patients undergoing surgery in the chest or near the diaphragm

43
Case 4 A 65 year old man non-smoker, lawyer, admitted for elective Lap Chole. Reports long history of mild cough, and dyspnea on exertion Physical exam: bibasilar dry crackles (velcrow), clubbing of the fingers
, clubbing of the fingers.")
44
Case 4 Predicted Values Measured Values % Predicted FVC 5.68 liters
65 % FEV1 4.90 liters 3.52 liters 60 % FEV1/FVC 84 % 79 % 94 % Restricted defect

45
Case 4 TLC 60% RV 40% DLCO 40% HRCT

46
Case 4

47
Case 5 68 year old man with progressive dyspnea of one year duration, ex-smoker, no cough, no wheezing, no orthopnea… History of CAD, SVT post angioplasty on multiple medication EF% 55 Meds: Plavix, beta one blocker, diuretics, cordarone, ARB,

48
Case 5 FVC 50% FEV1 55% FEV1/FVC 85% TLC 70% DLCO 50%

49
Case 5 PFT’s: Major drop in FVC and DLCO compared to the PFT done 2 years earlier HRCT of chest: Increased markings over the bases, with areas of increased enhancement…. Consistent with Amiodarone toxicity

50
Follow up patients Connective Tissue diseases (e.g. scleroderma)
Patients on Therapy that might affect the pulmonary system Neuromuscular diseases

51
Follow up Patients with Lung Diseases
Obstructive airway diseases Interstitial lung diseases Sarcoidosis IPF ILD (CTD)
")
52
Conclusion PFT’s Spirometry Lung volumes DLCO

53
Conclusion: Indications
Evaluating breathlessness Initial evaluation of patient with known respiratory disease Following the course of a respiratory disease Pre-operative assessment Disability evaluation Screening of subclinical disease

Similar presentations













 Airway.>")
















