Download presentation
Presentation is loading. Please wait.

1
INTRODUCTION to LOCAL ANESTHESIA and NEUROPHYSIOLOGY

2
Definition of Local Anesthesia
a loss of sensation in a circumscribed area of the body caused by a depression of excitation in nerve endings Or an inhibition of the conduction process in peripheral nerves; no loss of consciousness occurs

3
Properties of Local Anesthetics:
1) Not irritating to the tissue 2) No permanent alteration of nerve structure 3) Systemic toxicity should be low 4) Effective whether injected or applied topically 5) Time of onset of anesthesia should be as short as possible 6) Duration of action must be long enough to complete the procedure but not so long as to require an extended recovery 7) Should be stable in solution and easily biotransformed 8) Should not cause allergic reactions 9) Should be sterile or capable of being sterilized by use of heat
 Not irritating to the tissue. 2) No permanent alteration of nerve structure. 3) Systemic toxicity should be low. 4) Effective whether injected or applied topically. 5) Time of onset of anesthesia should be as short as possible. 6) Duration of action must be long enough to complete the procedure. but not so long as to require an extended recovery. 7) Should be stable in solution and easily biotransformed. 8) Should not cause allergic reactions. 9) Should be sterile or capable of being sterilized by use of heat.")
4
Neurophysiology The Neuron
The neuron is the structural unit of the nerve Two types of neurons 1) Sensory afferent (toward the CNS) 2) Motor efferent (away from the CNS)
 Sensory afferent (toward the CNS) 2) Motor efferent (away from the CNS)")
5
Sensory Neurons: transmit pain; three parts 1) Dendritic Zone- free nerve endings; most distal portion of the neuron 2) Axon- synapses with the CNS to transmit input to the brain 3) Cell Body- provides metabolic support for the entire neuron
 Dendritic Zone- free nerve endings; most distal portion of the neuron 2) Axon- synapses with the CNS to transmit input to the brain 3) Cell Body- provides metabolic support for the entire neuron")
6
Sensory Neurons (afferent)
")
7
Motor Neuron (efferent)
")
8
The Axon long cylinder of neural cytoplasm (axoplasm) encased in a
thin sheath, the nerve membrane, or axolemma axoplasm is a gelatinous substance that is separated from extracellular fluids by a continuous nerve membrane

9
nerve cell membrane is ~75 Angstroms thick
all cell membranes are organized to block the diffusion of water soluble molecules all cell membranes are selectively permeable via specialized pores transduce information by protein receptors responsive to chemical or physical stimulation by neurotransmitters, hormones, light, vibrations

10
The Membrane cell membrane is a bilipid layer of phospholipids
hydrophilic (polar) ends facing the outer surface and hydrophobic (nonpolar) ends projecting to the middle of the membrane
 ends facing the outer surface and. hydrophobic (nonpolar) ends projecting to the middle of. the membrane.")
11
the nerve membrane lies at the interface between the extracellular fluid and the axoplasm the nerve membrane separates highly ionic concentrations within the axon from those outside

12
The Membrane: Lipid Layer

13
The Membrane the resting nerve membrane has an electrical resistance about 50 times greater than that of the extra/intracellular fluids, thus preventing the passage of Na, K and Cl ions down their concentration gradients when a nerve impulse passes, electrical conductivity of the nerve membrane increases 100-fold: increased conductivity allows the passage of Na and K ions down their concentration gradient through the nerve membrane movement of these ions provides the energy for impulse conduction along the nerve some nerve fibers are covered in myelin, specialized Schwann cells

14
regular interval constrictions are called Nodes of Ranvier which form gaps between two adjoining Schwann cells

15
Electrophysiology of Nerve Conduction
Nerve resting potential is -70 mV; this is produced by differing concentrations of ions on either side of the nerve membrane Interior of the nerve is negative compared to the exterior before a stimulus excites the nerve

16
STEP 1 - Stimulus excites nerve which leads to: 1) Slow Depolarization- inside of nerve becomes less negative 2) Threshold Potential- extremely rapid depolarization occurs from the falling electrical potential 3) Rapid Depolarization- interior is electrically positive +40 mV and the outside is negative (-70 mv)
 Slow Depolarization- inside of nerve becomes less negative 2) Threshold Potential- extremely rapid depolarization occurs from the falling electrical potential 3) Rapid Depolarization- interior is electrically positive +40 mV and the outside is negative (-70 mv)")
17
Resting to Threshold Potential

18
Threshold Potential to Rapid Depolarization

19
STEP 2 - after depolarization, repolarization occurs Repolarization- electric potential inside the cell gradually becomes more negative until the interior is again restored to –70 mV

20
Depolarization Repolarization

21
Depolarization -excitation leads to increase in permeability of the cell membrane to sodium ions -transient widening of transmembrane ion channels allow passage of the sodium ions -rapid influx of sodium ions into the interior of the nerve cell causes depolarization of the cell membrane from resting to firing threshold which is -50 to -60 mV

22
Firing Threshold magnitude of the decrease in negative trans-membrane potential that is necessary to initiate an action potential (impulse); getting more positive with more influx of Na+
; getting more positive with more influx of Na+")
23
Firing Threshold

24
-decrease in negative transmembrane potential of +15 mV; from –70 mV to –55 mV is necessary to reach the firing threshold; voltage differences of less than +15 mV will not induce firing -exposure to a nerve with local anesthetic raises its firing threshold -elevating the firing threshold means that more sodium must pass through the membrane to decrease the negative transmembrane potential to a level where depolarization occurs

25
-when the firing threshold is reached, sodium rapidly enters the axoplasm due to increased membrane permeability -depolarization lasts ~ .3 msec

26
Repolarization The action potential is terminated when the membrane repolarizes; this is caused by the inactivation of increased permeability to sodium The movement of Na+ and K+ during depolarization is passive

27
Repolarization

28
After the membrane potential returns to –70 mV there is still a slight amount of excess sodium within the nerve cell and a slight excess of potassium extracellularly Sodium is moved out of the cell using ATP and the sodium pump Repolarization requires ~ .7 msec

29
Absolute Refractory Period the nerve is unable to respond to another stimulus regardless of its strength Relative Refractory Period a new impulse can be initiated at this time but only by a stronger than normal stimulus; follows the absolute refractory period

30
Membrane Channels Sodium channels line the excitable nerve membrane which are lipoglycoproteins situated firmly in the membranes Sodium passes through the channels 12 times easier than potassium Sodium ions are “thinner” than potassium or chloride ions and should therefore move easily down concentration gradients through membrane channels into the nerve cell, however: However, sodium ions are hydrated at rest and increase in size to 3.4 Angstroms; they are too large to pass through the sodium channels when the nerve is at rest

31
Membrane Channels

32
Membrane Channels Potassium and chloride can pass through these gated channels During depolarization the gated transmembrane sodium channels change their configuration to allow the sodium ions to enter the cell

33
Impulse Propagation Activation of an action potential by a stimulus Disruption of the resting nerve membrane potential Interior of the cell goes from negative (–70 mV) to positive (+40 mV) Exterior of the cell changes from positive to negative Local currents begin flowing between the depolarized segment and the adjacent resting area Local currents flow from positive to negative extending for several mm along the nerve membrane As a result, the interior of adjacent areas become less negative and the exterior becomes less positive
 to positive (+40 mV) Exterior of the cell changes from positive to negative Local currents begin flowing between the depolarized segment and the adjacent resting area Local currents flow from positive to negative extending for several mm along the nerve membrane As a result, the interior of adjacent areas become less negative and the exterior becomes less positive")
34
Impulse Propagation

35
Impulse Propagation Transmembrane potential decreases approaching firing threshold for depolarization When transmembrane potential decreases by 15mV from resting potential, firing threshold is reached and rapid depolarization occurs The newly depolarized segment sets up local currents and it all starts over again Newly depolarized segments return to resting state after absolute and relative refractory periods Waves of depolarization can move in only one direction due to the absolute and relative refractory periods, thus retrograde (backward) movement is prevented
 movement is prevented")
36
Impulse Spread 1) Unmyelinated Nerves
-high electrical resistance cell membrane -slow forward “creeping” spread of impulses -conduction of unmyelinated C fibers is1.2 m/sec

37
2) Myelinated Nerves -insulating myelin separates the extra/intracellular charges -the farther apart the charges the smaller the current necessary to charge the membrane -current leaps from node to node saltatory conduction

38
Myelinated Nerves if conduction of an impulse is blocked at one node, the local current skips that node and continues to the next node

39
A minimum of 8 to 10 mm of nerve must be covered by anesthetic solution to ensure adequate block of impulse spread

40
Mode and Site of Action of Local Anesthetics
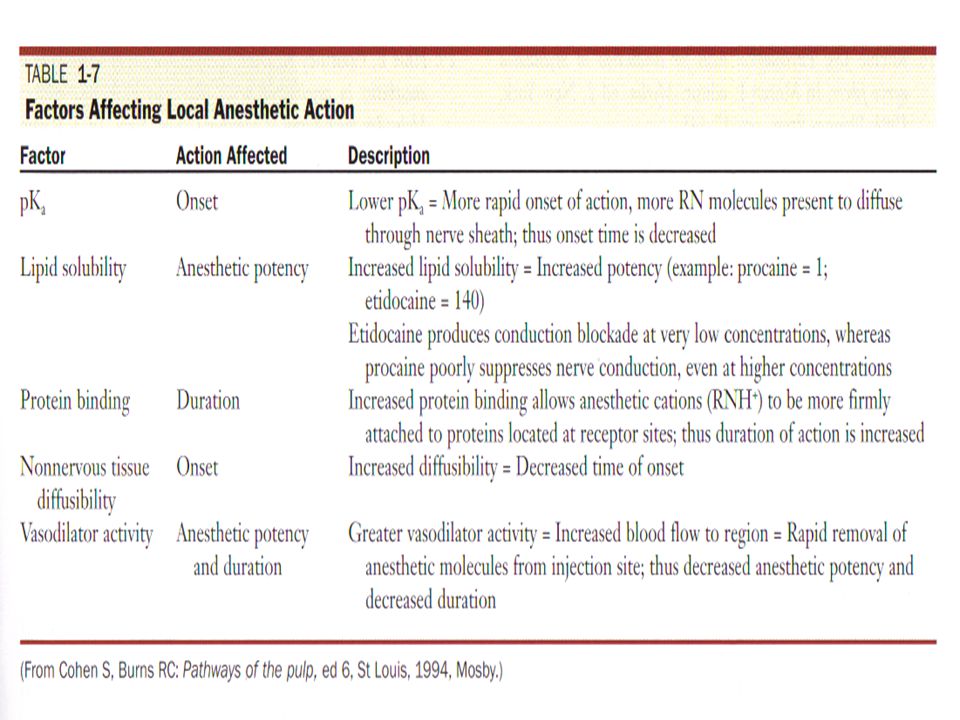
Local anesthetics interfere with the excitation process in the nerve membrane in one or more of the following ways: 1) Altering the basic resting potential of the nerve membrane 2) Altering the threshold potential (firing level) 3) Decreasing the rate of depolarization* 4) Prolonging the rate of repolarization
 Altering the basic resting potential of the nerve membrane. 2) Altering the threshold potential (firing level) 3) Decreasing the rate of depolarization* 4) Prolonging the rate of repolarization.")
41
Because of local anesthetics, cellular depolarization is not sufficient to reduce the membrane potential of a nerve fiber to its firing threshold and a propagated action potential does not develop

42
Where Do Local Anesthetics Work?
Specific Receptor Theory local anesthetics act by binding to specific receptors on the sodium channel the action of the drug is direct and is not mediated by some change in the general properties of the cell membrane a specific receptor site for local anesthetics exists in the sodium channel which eliminates permeability to sodium ions Therefore: no impulse conduction

43
Tertiary amine local anesthetics inhibit influx of sodium during nerve conduction

44
Mechanism of Action of Local Anesthetics
1) Displacement of calcium ions from the sodium channel receptor site 2) Binding of the local anesthetic molecule to this receptor site 3) Blockade of the sodium channel 4) Decrease in sodium conductance 5) Depression of the rate of electrical depolarization 6) Failure to achieve the threshold potential level (firing level) 7) Lack of development of propagated action potentials 8) Conduction blockade
 Displacement of calcium ions from the sodium channel receptor site. 2) Binding of the local anesthetic molecule to this receptor site. 3) Blockade of the sodium channel. 4) Decrease in sodium conductance. 5) Depression of the rate of electrical depolarization. 6) Failure to achieve the threshold potential level (firing level) 7) Lack of development of propagated action potentials. 8) Conduction blockade.")
45
1) The nerve remains in a polarized state, therefore there is no depolarization because the ionic movements responsible for the action potential fail to develop 2) The membrane’s electrical potential remains unchanged, therefore local currents do not develop and the self-perpetuating mechanism of impulse propagation is stalled 3) Nerve block produced by local anesthetic is called a nondepolarizing nerve block
 The nerve remains in a polarized state, therefore there is no depolarization because the ionic movements responsible for the action potential fail to develop 2) The membrane’s electrical potential remains unchanged, therefore local currents do not develop and the self-perpetuating mechanism of impulse propagation is stalled 3) Nerve block produced by local anesthetic is called a nondepolarizing nerve block")
46
Local Anesthetic Molecules
Majority of local anesthetics are tertiary amines (except Prilocaine) All local anesthetics are amphipathic (lipophilic/hydrophilic)
 All local anesthetics are amphipathic (lipophilic/hydrophilic)")
47
Three main parts of the local anesthetic molecule: 1) Lipophilic Part (aromatic ring) 2) Intermediate Chain (amide or ester) 3) Hydrophilic Part (ethyl alcohol/acetic)
 Lipophilic Part (aromatic ring) 2) Intermediate Chain (amide or ester) 3) Hydrophilic Part (ethyl alcohol/acetic)")
48
The lipophilic part of the local anesthetic is the largest portion of the molecule
Hydrophilic part of the local anesthetic is an amino derivative of ethyl alcohol or acetic acid Local anesthetics without a hydrophilic portion are not suitable for injection but are good topical anesthetics, i.e., Benzocaine

50
What Form Do Local Anesthetics Exist in the Cartridge?
Labs prepare local anesthetics as basic: poorly soluble in water and unstable on exposure to air; they have little to no clinical value in this state Since they are weakly basic, they combine readily with acids to form local anesthetic salts which makes them soluble in water and stable

51
Local anesthetics used for injection are dispensed as salts, most commonly the hydrochloride salt, dissolved in either sterile water or saline; so in the cartridge they are salts

52
pH Variations Acidification of tissues decreases local anesthetic effectiveness Inadequate anesthesia results when local anesthetics are injected into inflamed/infected tissues pH of normal tissues ~ pH of inflamed tissues ~ 5.5 Local anesthetics containing epinephrine or other vasopressors are acidified by the manufacturer to inhibit the oxidation of the vasopressor

53
Clinically, the lower the pH the more burning on injection slower onset of anesthesia pH of the interior of the nerve remains unchanged and stable despite wide variations in extracellular fluid pH; so it is with the pH of the extracellular fluid that determines the success or failure of local anesthetics

54
Why not increase the pH of the local anesthetic in the cartridge
Why not increase the pH of the local anesthetic in the cartridge? ANSWER: Because the local anesthetic base is unstable, it would precipitate out of alkalinized solutions

55
The extracellular fluid pH is most important when it comes to the free base getting into the nerve sheath; if the extracellular pH is acidic, as with an infection, the local anesthetic can not enter the nerve in order to do its job; the free base state will never appear or so few molecules will cross the nerve membrane and inadequate anesthesia will occur

56
Effect of decreased pH on actions of local anesthetic
Less free base (RN) molecules available to diffuse across nerve sheath
 molecules available to diffuse across nerve sheath.")
57
Block anesthesia can be successful even in the presence of infection; do not inject directly into the infection because it can be spread throughout the connective tissue

58
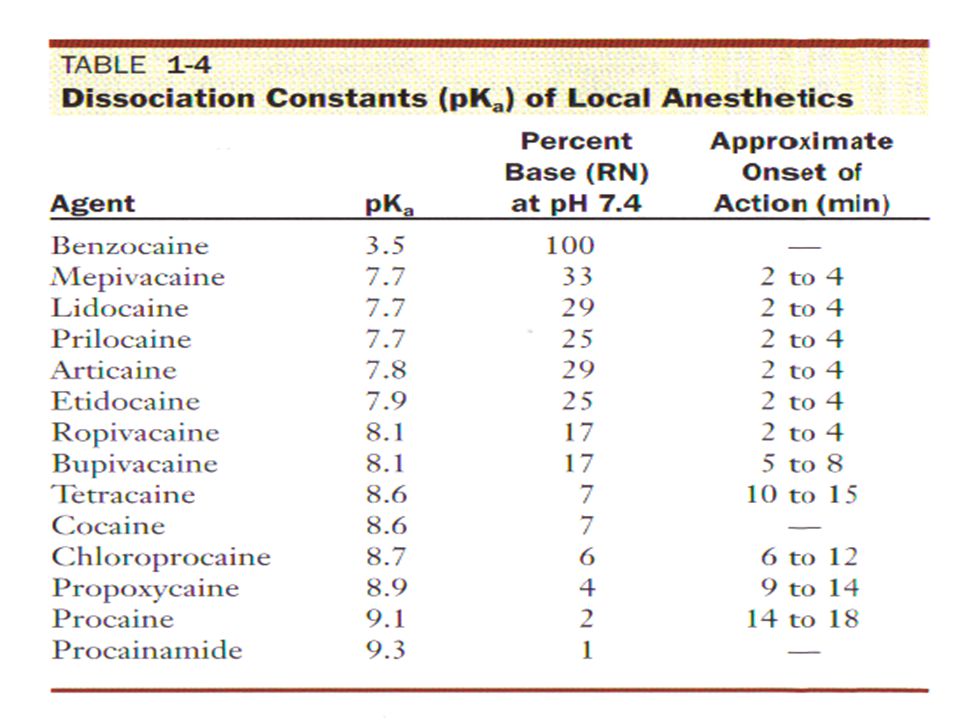
Dissociation of Local Anesthetics
The local anesthetic salt is dissolved in sterile water or saline -It exists simultaneously as: 1) uncharged molecules (free base) (RN) (Class C) 2) positively charged molecules (cation) (RNH+) (Class D)
 uncharged molecules (free base) (RN) (Class C) 2) positively charged molecules (cation) (RNH+) (Class D)")
59
Dissociation of Local Anesthetics pKa is a measure of a molecule’s affinity for hydrogen ions (H+); when the pH of a solution has the same value as the pKa, 50% of the drug exists as the free base (RNH+) and 50% exists as the cation (RN)
; when the pH of a solution has the same value as the pKa, 50% of the drug exists as the free base (RNH+) and 50% exists as the cation (RN)")
60
Low pH (acidic) shifts toward the cationic form; more RNH+ High pH (basic) shifts toward the free base form; more RN
 shifts toward the cationic form; more RNH+ High pH (basic) shifts toward the free base form; more RN")
61
The relative proportions of ionic forms (RNH+, RN) depends on three variables: 1) pH of the local anesthetic solution 2) pH of the surrounding tissues (infection or not) 3) pKa or dissociation constant of the specific local anesthetic
 depends on three variables: 1) pH of the local anesthetic solution 2) pH of the surrounding tissues (infection or not) 3) pKa or dissociation constant of the specific local anesthetic")
63
higher pKa increased H+ increased Onset Time Bupivacaine with pKa ~8
higher pKa increased H increased Onset Time Bupivacaine with pKa ~8.1 will take longer to work because there are fewer free base molecules available to penetrate the nerve membrane it can take up to 8 minutes at pH of 7.4 (tissue pH) (especially with infection present)
 (especially with infection present)")
64
Four Factors Are Involved In The Action of a Local Anesthetic: 1) Diffusion of the drug through the nerve sheath 2) Binding of the drug at the receptor site in the membrane channel 3) Free bases (RN) cross the nerve membrane 4) Cation (RNH+) blocks the receptor The uncharged, lipid-soluble free base (RN) form of the local anesthetic is responsible for diffusion through the nerve membrane
 Diffusion of the drug through the nerve sheath 2) Binding of the drug at the receptor site in the membrane channel 3) Free bases (RN) cross the nerve membrane 4) Cation (RNH+) blocks the receptor The uncharged, lipid-soluble free base (RN) form of the local anesthetic is responsible for diffusion through the nerve membrane")
65
Local Anesthetics with lower pKa have large number of free base molecules (RN) that are able to diffuse through the nerve sheath But the anesthetic action of this drug is inadequate because at intracellular pH of 7.4 a very small number of base molecules dissociate back to the cationic form (RNH+) necessary for binding at the receptor site (e.g., Benzocaine = pKa 3.5)
 that are able to diffuse through the nerve sheath But the anesthetic action of this drug is inadequate because at intracellular pH of 7.4 a very small number of base molecules dissociate back to the cationic form (RNH+) necessary for binding at the receptor site (e.g., Benzocaine = pKa 3.5)")
66
The rate of onset is related to the pKa of the local anesthetic Bupivacaine at pKa 8.1 has a slower onset than Lidocaine pKa 7.7

67
Antioxidants and pH Antioxidants are added to local anesthetics to delay the oxidation of the vasopressor; oxidation will turn the solution a reddish-brown Sodium bisulfite is a common antioxidant placed in local anesthetic solution Lidocaine 2% with a pH of 6.8 is acidified to a pH of 4.2 with the addition of the antioxidant sodium bisulfite The shelf life of local anesthetics decrease as the pH of the solutions decreases

68
The large buffering capacity of the tissue (pH 7
The large buffering capacity of the tissue (pH 7.4) is able to maintain a normal tissue pH, however, it takes a longer time to do so after an injection of a pH 4.2 solution than with a pH 6.8 solution the end result is a slower clinical onset of action while the tissue pH equilibrates the pH of the solution with the pH of the tissues
 is able to maintain a normal tissue pH, however, it takes a longer time to do so after an injection of a pH 4.2 solution than with a pH 6.8 solution the end result is a slower clinical onset of action while the tissue pH equilibrates the pH of the solution with the pH of the tissues.")
69
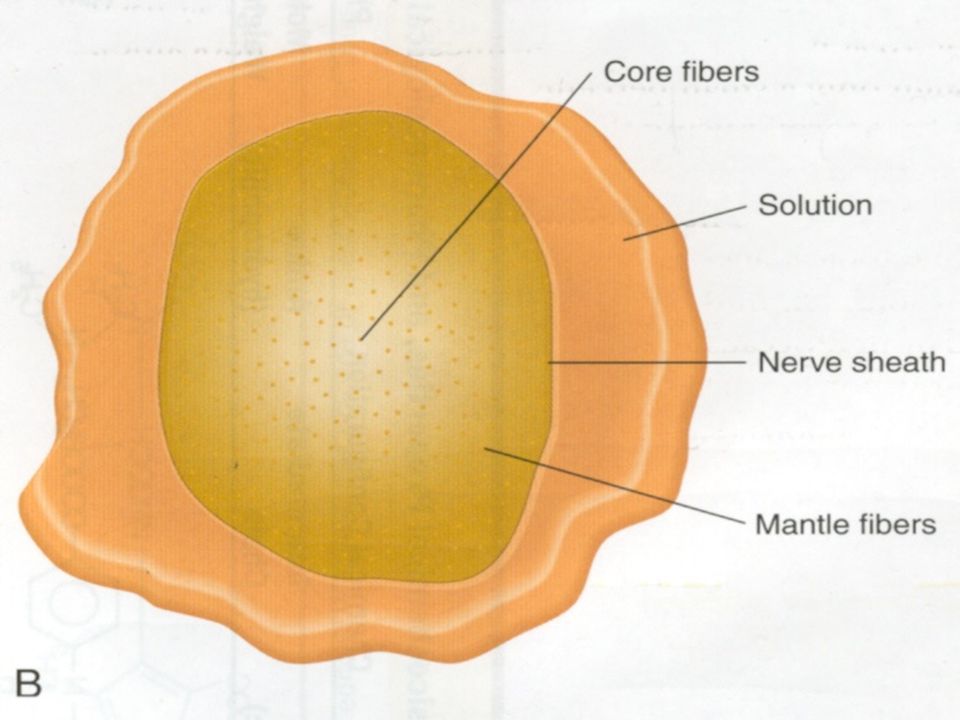
Barriers to Diffusion of the Solution

70
Induction of Local Anesthesia
Mantle Bundles (OUTSIDE) -fasciculi that are located near the surface of the nerve -first ones reached; exposed to higher concentration of the solution -blocked completely shortly after injection -innervates more proximal regions of the nerve (molars from IANB)
 -fasciculi that are located near the surface of the nerve. -first ones reached; exposed to higher concentration of. the solution. -blocked completely shortly after injection. -innervates more proximal regions of the nerve. (molars from IANB)")
72
Core Bundles (INSIDE) -fasciculi found closer to the center of the nerve -must delay before onset of anesthesia; lower concentration of solution -explains why patient may have inadequate pulpal anesthesia in the midst of profound soft tissue anesthesia -innervates more distal regions of the nerve (incisors from IANB)
 -fasciculi found closer to the center of the nerve -must delay before onset of anesthesia; lower concentration of solution -explains why patient may have inadequate pulpal anesthesia in the midst of profound soft tissue anesthesia -innervates more distal regions of the nerve (incisors from IANB)")
74
Induction Time Factors Under Clinician’s Control:
1) Concentration of the drug 2) pH of the local anesthetic solution Factors not Under Clinician’s Control: 1) Diffusion constant of the anesthetic drug 2) Anatomical diffusion barriers of the nerve
 Concentration of the drug. 2) pH of the local anesthetic solution. Factors not Under Clinician’s Control: 1) Diffusion constant of the anesthetic drug. 2) Anatomical diffusion barriers of the nerve.")
76
What is the order of recovery from Local Anesthetic?
Follows same diffusion patterns as induction only in the reverse order Mantle fibers lose anesthesia before the core fibers Third molars would regain sensation before incisors if an inferior alveolar nerve block were administered Recovery is a slower process than induction because the local anesthetic molecule is bound to the drug receptor site in the sodium channel and is released more slowly than it is absorbed

77
What if I need to re-inject a patient?
At the time of re-injection, the concentration of local anesthetic in the mantle fibers is less than the centrally located core fibers The partially recovered mantle fibers still contain some level of local anesthetic, although not enough to provide complete anesthesia Upon re-injection, the mantle fibers are again subjected to a high concentration of local anesthetic solution inward toward the nerve

78
-The combination of residual local anesthetic and the newly deposited supply results in rapid onset of profound anesthesia with a smaller volume of the drug being administered -Tachyphylaxis is an increased tolerance to a drug that is administered repeatedly; this could result in less anesthesia after re-injection

Similar presentations












 Nervous system functions Structure of a neuron Sensory, motor, inter- neurons Membrane potential Sodium.>")



 from one part of the body to another. ◦ Major regions.>")




