Download presentation
Presentation is loading. Please wait.

1
Pediatric Seizure and SE Patient ED Care: Challenging Cases
Edward P. Sloan, MD, MPH, FACEP 1

2
Dept of Emergency Medicine University of Illinois College of Medicine
Edward P. Sloan, MD, MPH Professor Dept of Emergency Medicine University of Illinois College of Medicine Chicago, IL Edward P. Sloan, MD, MPH, FACEP 2

3
Attending Physician Emergency Medicine
University of Illinois Hospital Our Lady of the Resurrection Hospital Chicago, IL Edward P. Sloan, MD, MPH, FACEP 3

4
Housekeeping Issues Disclosures Meeting support from UCB Pharma
Thank you Dave Riccio IV levetiracetam, a second generation AED May soon be an IV parenteral option in the ED Please fill out a CME form with your Please give feedback to improve our work

5
Overview Acute Pediatric Seizures
Common ED problem Seizures: 6% of EMS encounters Pediatric seizures: 1% of all ED visits Pediatric febrile: 1 in 125 visits (0.8%) Pediatric afebrile: 1 in 500 visits (0.2%)
 Pediatric afebrile: 1 in 500 visits (0.2%)")
6
Objectives Management Issues
Learn likely sz etiologies Seizure Rx without IV access Review seizure termination Rx Explore IV Rx for SE prevention Review EEG in E.D. SE Discuss clinical impact

7
Case Presentations ED Pediatric Seizure Cases
Seizing infant, no IV access Pediatric status epilepticus Adolescent sz pt with seizures College student with new onset sz New onset SE in an adolescent Discussion

8
Case #1: Seizing infant, no IV access
What therapies can be given? By what route? With what effect?

9
Febrile illness at home Seizing for paramedics Arrives in arms of CFD
Case #1 Hx 9 month old Febrile illness at home Seizing for paramedics Arrives in arms of CFD No IV access in field

10
Hyperpyrexia, abn vital signs Actively seizing, generalized
Case #1 Px Hyperpyrexia, abn vital signs Actively seizing, generalized Tonic-clonic motor activity Cardiopulm exam OK No IV access available

11
What are the diagnoses in this child?
Case #1 Dx What are the diagnoses in this child?

12
Generalized convulsive status epilepticus (GCSE)
Case #1 Dx Generalized convulsive status epilepticus (GCSE) Complex febrile seizure
 Complex febrile seizure.")
13
Case #1 Rx: Non-IV Options
What treatment would you provide for this patient? PR diazepam or rectal gel Buccal midazolam IM fosphenytoin IM midazolam IM phenobarbital

14
Case #1 Rx: Non-IV Options
IM midazolam Buccal midazolam IM fosphenytoin PR diazepam PR diazepam rectal gel IM phenobarbital less good

15
How do we diagnose ped SE? What is the optimal Rx protocol? Why?
Case #2: Pediatric SE How do we diagnose ped SE? What is the optimal Rx protocol? Why?

16
Seizure-like activity? Patient with staring spells
Case #2 Hx 7 year old male Seizure-like activity? Patient with staring spells Some headache and shaking movement, esp of hands Frontal headache, vomiting

17
AMS, r/o seizure disorder
Case #2 Hx (con’t) Seen at 2130, 2230 sign-out AMS, r/o seizure disorder “Once all of the labs are back, he should be OK to go home…”
 Seen at 2130, 2230 sign-out. AMS, r/o seizure disorder. Once all of the labs are back, he should be OK to go home…")
18
98.7 98/60 72 20 Well hydrated CV, lung exams normal Neuro exam intact
Case #2 Px / Well hydrated CV, lung exams normal Neuro exam intact

19
Tachycardia, assoc with AMS Confused, staring off into space
Case #2 Px (con’t) 0220 “episode” Tachycardia, assoc with AMS Confused, staring off into space Resolved without any Rx Three more episodes over 40’ Diaphoresis, urinary incontinence
 0220 episode Tachycardia, assoc with AMS. Confused, staring off into space. Resolved without any Rx. Three more episodes over 40’ Diaphoresis, urinary incontinence.")
20
What is the likely diagnosis in this pediatric patient?
Case #2 Dx What is the likely diagnosis in this pediatric patient? Absence status epilepticus Complex partial status epilepticus (CPSE) with autonomic signs Generalized non-convulsive seizure with autonomic signs Generalized convulsive SE
 with autonomic signs. Generalized non-convulsive seizure with autonomic signs. Generalized convulsive SE.")
21
Repetitive episodes with AMS Associated autonomic signs
Case #2 Dx Repetitive episodes with AMS Associated autonomic signs Rule out generalized nonconvulsive status epilepticus Complex partial status epilepticus Absence status epilepticus

22
How would you initially treat this pediatric seizure patient?
Case #2 Rx How would you initially treat this pediatric seizure patient? IV diazepam IV lorazepam IV phenobarbital IV valproate Rectal diazepam

23
Case #2 Rx Would you load this patient with another antiepileptic drug prior to transfer to the children’s hospital? Yes No

24
Case #2 Rx If you were to load this patient with an AED, what agent would you use? IV phenytoin IV fosphenytoin IV phenobarbital IV valproate Other

25
Transfer to Children’s for ICU observation
Case #2 Rx IV lorazepam IV valproate Transfer to Children’s for ICU observation

26
Case #3: Adolescent Sz Pt with Seizures
How to manage seizing children on PO valproate? Does a level need to be checked prior to ED loading? When and how to rapidly restore a therapeutic level?

27
Hx complex partial seizures
Case #3 Hx 12 yo F Hx autism Hx complex partial seizures Hx secondary generalized tonic-clonic seizures Pt taking Depakote sprinkles BID Presents to ED, has 2nd seizure

28
Generalized tonic-clonic seizure
Case #3 Px VS OK prior to seizure Chest: Clear CV: Reg without Neuro: Non-focal Generalized tonic-clonic seizure

29
Hx complex partial seizures
Case #3 Dx Generalized seizures Hx complex partial seizures Sub-therapeutic valproate level vs. break-thru seizure

30
Case #3 Rx After an initial dose of a benzodiazepine is given, would you obtain a valproate level prior to giving IV valproate? Yes No

31
Case #3 Rx To achieve a high therapeutic level of 125 ucg/ml, if the measured level is 25 ucg/ml, how much IV valproate should be administered in mg/kg ? 100 mg/kg 50 mg/kg 20 mg/kg 5 mg/kg

32
IV lorazepam, avoid status epilepticus Determine valproate level
Case #3 Rx IV lorazepam, avoid status epilepticus Determine valproate level For every mg/kg loaded, the level goes up 5 mcg/ml To increase the level by 100 mcg/ml, give 20 mg/kg. For a 50 kg child, give 1000 mg of IV valproate

33
Case #4: College Student, New Onset Sz
What is the likely etiology? What are the long-term implications? How to manage once the seizure has stopped?

34
21 year old college student No known neuro history
Case #4 Hx 21 year old college student No known neuro history Final exams, sleepless Great party after the last exam Pt with single generalized seizure in am, upon awakening

35
Neuro: slightly post-ictal Exam otherwise normal
Case #4 Px Vitals OK Neuro: slightly post-ictal Exam otherwise normal Patient has a 2nd seizure in the ED

36
What is the likley diagnosis in this young adult?
Case #4 Dx What is the likley diagnosis in this young adult? Complex partial seizures with secondary generalization Juvenile myoclonic epilepsy Generalized tonic-clonic seizure Absence seizure

37
Juvenile myoclonic epilepsy
Case #4 Dx Juvenile myoclonic epilepsy Related to sleep deprivation, alcohol consumption, occurs upon awakening May have a history of myoclonic jerks Responds long-term best to valproate

38
Benzodiazepines to Rx the acute sz Ongoing protection an issue
Case #4 Rx Benzodiazepines to Rx the acute sz Ongoing protection an issue Phenytoin may not be optimal Valproate may be preferred Avoid status epilepticus

39
Case #5: New Onset AMS/Spells
What is the AMS? Is it a seizure? How should we Rx new onset seizure patients? What role does the ED EEG play in sz and SE?

40
HA, frontal, cw prior migraines HA relieved with ibuprofen
Case #5 Hx 13 year old female HA, frontal, cw prior migraines HA relieved with ibuprofen AMS this AM, with ? motor activity Restless at home, thrashing on bed No other systemic sx

41
Neuro: No focal deficit. MS OK
Case #5 Px Vitals OK, afebrile Alert, O x 3, NAD Head/Neck OK Chest/cor/abd OK Neuro: No focal deficit. MS OK

42
What diagnostic tests are indicated at this point?
Case #5 Question # 1 What diagnostic tests are indicated at this point?

43
Did this patient have a seizure? Yes No
Case #5 Question # 2 Did this patient have a seizure? Yes No

44
Case #5 Question # 3 Does the patient require admission for observation for possible new onset seizures? Yes No

45
Neuro consult: EEG and then D/C Dx: Seizure, migraine HA
Case #5 Clinical Course Labs, tox screen neg CT negative Neuro consult: EEG and then D/C Dx: Seizure, migraine HA While EEG applied, pt with AMS Agitation, thrashing on cart

46
Is this repeat spell a seizure? What type?
Case #5 Question # 4 Is this repeat spell a seizure? What type?

47
Does this AMS, motor activity require Rx? What Rx?
Case #5 Question # 5 Does this AMS, motor activity require Rx? What Rx?

48
Case #5 Question # 6 Does the patient require admission for observation for possible new onset seizures?

49
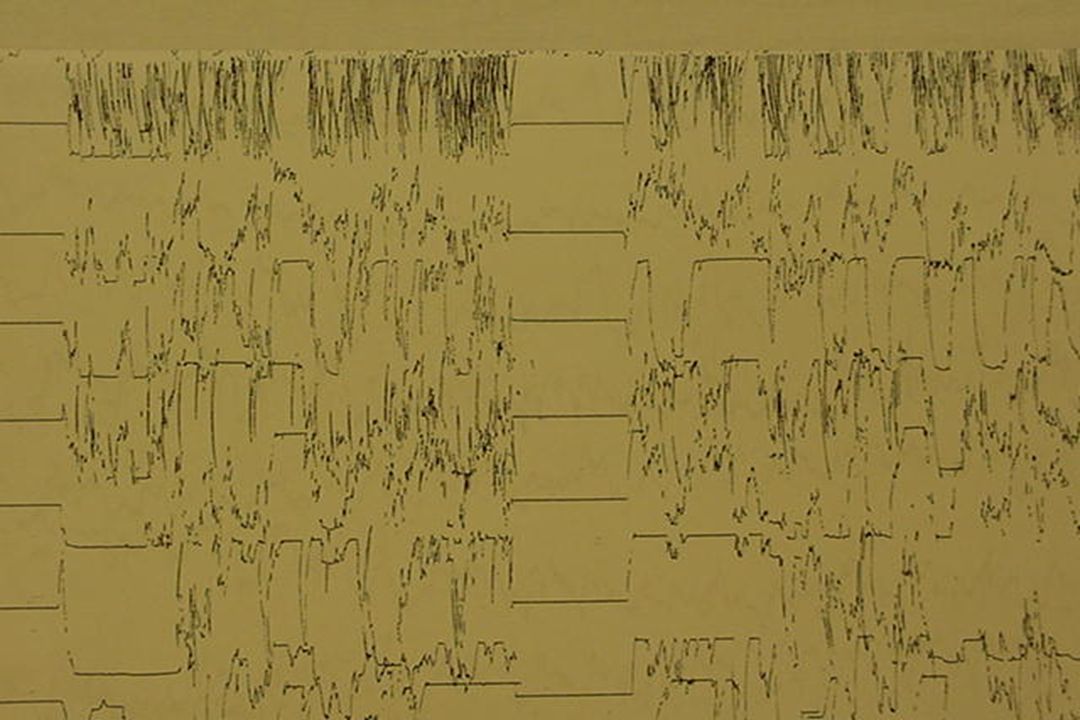
Case #5 Clinical Course (con’t)
During EEG, pt with R face focal sz Leftward gaze noted Seizure then generalizes Meds are given Seizure is terminated

50
What med is to be used for seizure control / SE termination?
Case #5 Question # 7 What med is to be used for seizure control / SE termination?

51
What med is to be used once SE is terminated? Why?
Case #5 Question # 8 What med is to be used once SE is terminated? Why?

52
How should the meds be given? Why?
Case #5 Question # 9 How should the meds be given? Why?

53
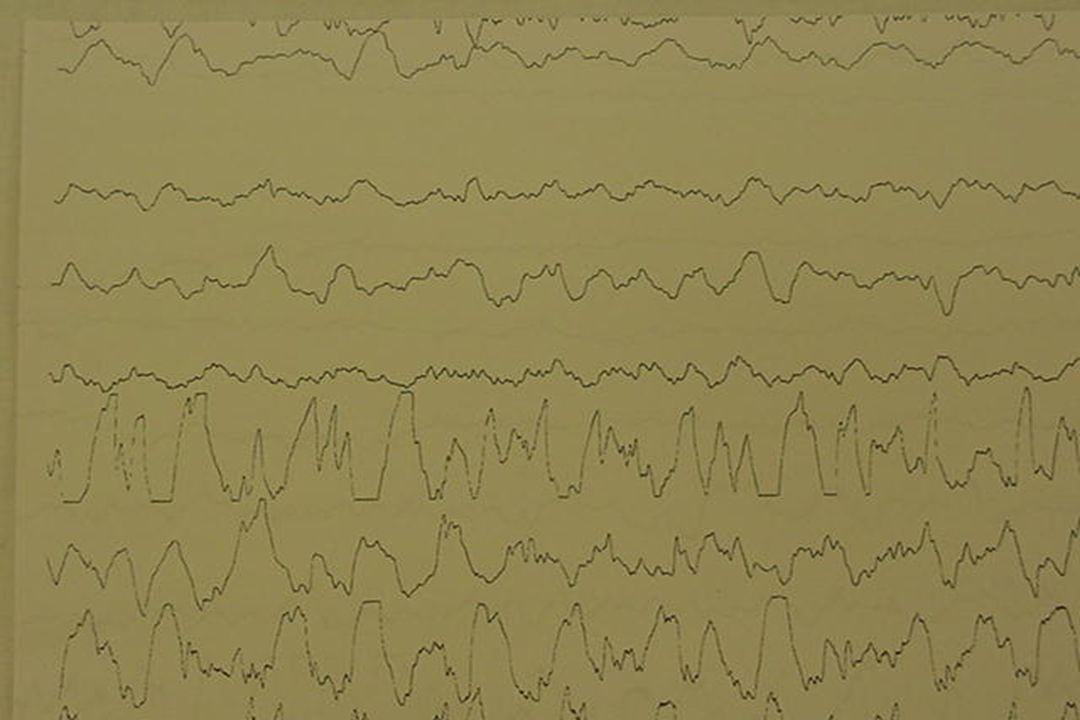
Case #5 Clinical Course (con’t)
SE terminated with Rx Pt stabilized ALS transfer to Children’s with team Pt with resolving AMS at time of D/C

54
Lorazepam to Rx the acute sz
Case #5 Rx Lorazepam to Rx the acute sz IV phenytoin, fosphenytoin, valproate, phenobarbital are AED load options PRN meds during transfer

55
What is the diagnosis in this young patient? Absence seizure
Case #5 Dx What is the diagnosis in this young patient? Absence seizure Complex partial seizures with secondary generalized seizure Focal motor seizure Complex migraine headache

56
Complex partial seizure with secondary generalized seizure
Case #5 Dx New onset seizure/SE Complex partial seizure with secondary generalized seizure Hx migraine headaches

57
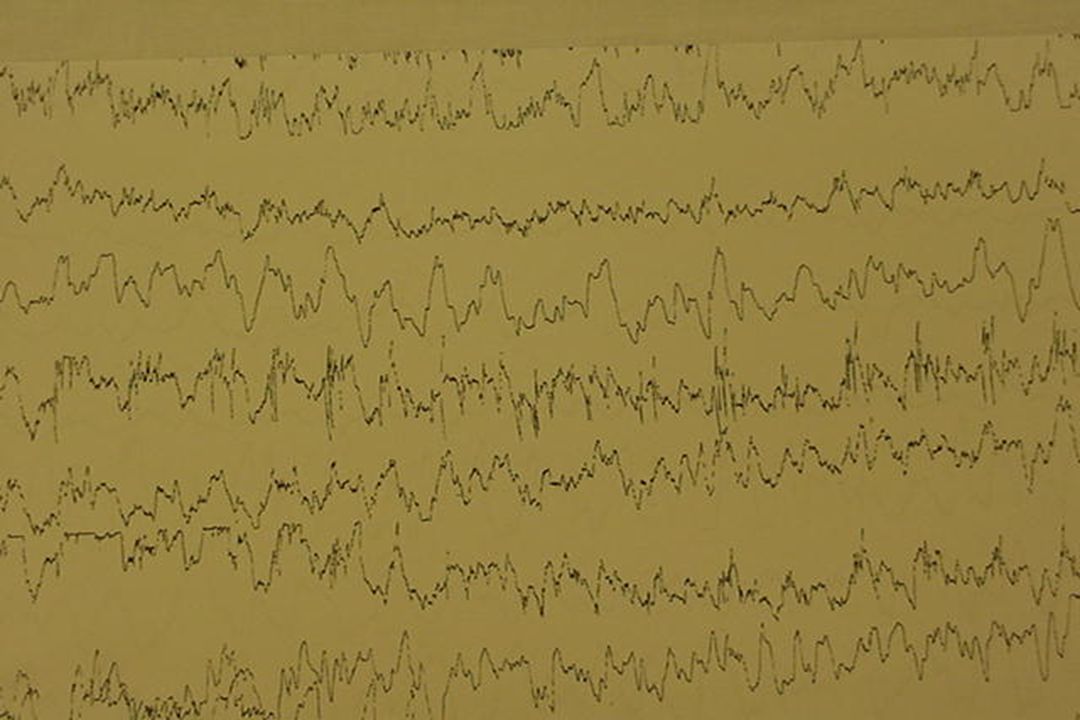
Do you believe you could diagnose a seizure on an EEG? Yes No
Case #5 Dx Do you believe you could diagnose a seizure on an EEG? Yes No

65
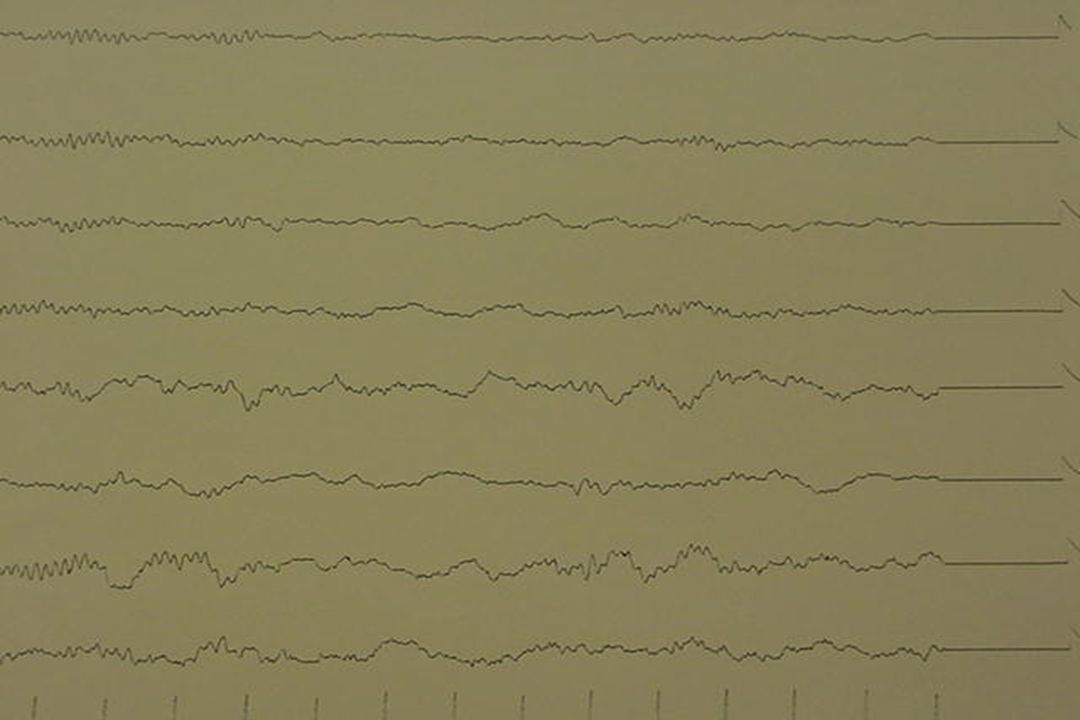
Conclusions Key Learning Points
Acute, repetitive spells = sz Multiple meds and routes possible Opportunity to optimize Rx Acute seizure control: IV benzos 2nd line Rx may differ based on Dx Ongoing needs may influence 2nd Rx EEG may be of use in ED seizures

66
Recommendations Management Implications
Educate about sz etiologies Make multiple drugs available Alternate routes should be used A protocol should exist Utilize EEG when necessary Be aware of optimal Rx at disposition

67
CME Question Have you learned something new about pediatric seizures today such that you can change and improve your clinical practice? Yes No

68
CME Follow-up CME providers require follow-up to assess if your learning has indeed improved your clinical practice. Can we ask you this question via again in the future? Yes No

69
Questions?? Edward P. Sloan, MD, MPH, FACEP ferne_aaem_france_2005_sloan_pedssz_fshow.ppt 4/1/2017 4:49 PM Edward P. Sloan, MD, MPH, FACEP 54 1 54

Similar presentations




















 Grants Chapter 6.>")

