Download presentation
Presentation is loading. Please wait.

1
Voiding Dysfunction in Children
By Dr.Turky K. Al-Mouhissen Urology Chief Resident - WR King Abdulaziz Medical Center - WR

2
Normal Bladder Function in Infants & Children:
The bladder is an abdominal organ Detrusor consists of meshwork of smooth m. which has the ability to elicit maximal active tension over a wide range of length This allows the bladder to be filled at low pressure (compliance) Reservoir function determined by activity of detrusor m. and bladder outlet Bladder sphincter plays a major role in urinary continence by closure of bladder neck & proximal urethra
 Reservoir function determined by activity of detrusor m. and bladder outlet. Bladder sphincter plays a major role in urinary continence by closure of bladder neck & proximal urethra.")
3
Literature suggests that
Immature detrusor-sphincter coordination, manifested as detrusor hypercontractility and interrupted voiding, commonly occurs in 1st 1-2 years causing a degree of functional bladder outflow obstruction (Sillen et al,1992;Yeung et al,1998) Some found significant age related differences in the histologic structure of the sphincter compared to adults Activation, coordination, and integration of various parts of the bladder-sphincter complex involves central, somatic & autonomic nervous system through Sacral parasympathatic (pelvic n.) Thoracolumbar symp. (hypogastric & sympathatic chain) Sacral somatic n. (pudendal n.)
 Some found significant age related differences in the histologic structure of the sphincter compared to adults. Activation, coordination, and integration of various parts of the bladder-sphincter complex involves central, somatic & autonomic nervous system through. Sacral parasympathatic (pelvic n.) Thoracolumbar symp. (hypogastric & sympathatic chain) Sacral somatic n. (pudendal n.)")
4
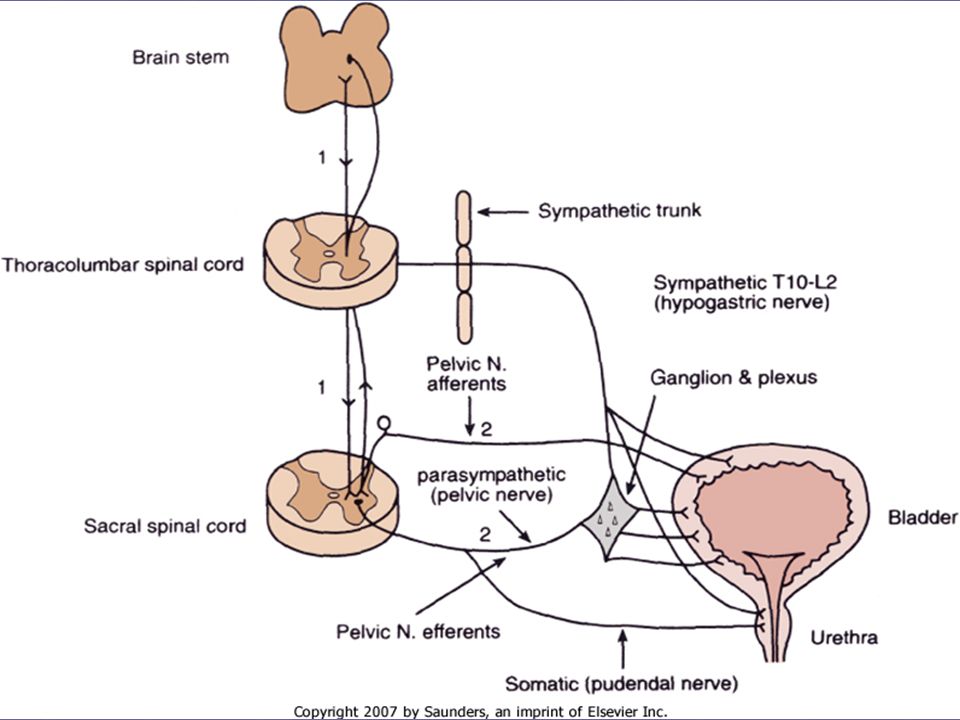
Parasymp. N. fibers run in pelvic n
Parasymp. N. fibers run in pelvic n. (S2-S4) to supply the pelvic and vesical plexuses before entering the bladder Symp. n. arises from (T10-L2) to inferior mesenteric ganglion hypogastric n. to the pelvic plexus & bladder There is also symp. innervation from T10-L2 supplying the detrusor and urethral sphincter The somatic nervous system (pudendal n.) supplies the periurethral pelvic floor muscles The sensory & motor n. carried by all 3 nerves innervate the bladder and urethral sphincter
 to supply the pelvic and vesical plexuses before entering the bladder. Symp. n. arises from (T10-L2) to inferior mesenteric ganglion hypogastric n. to the pelvic plexus & bladder. There is also symp. innervation from T10-L2 supplying the detrusor and urethral sphincter. The somatic nervous system (pudendal n.) supplies the periurethral pelvic floor muscles. The sensory & motor n. carried by all 3 nerves innervate the bladder and urethral sphincter.")
6
Parasymp. supply causes detrusor contraction (muscarinic receptors)
Detrusor relaxation (B receptors) Smooth m contraction at trigone & bladder neck (alpha receptors) Parasymp. supply causes detrusor contraction (muscarinic receptors) Pudendal supply causes striated sphincter contraction Within the spinal cord, information from bladder afferents integrated with other sources and projected to brain stem centers to coordinate with mic. centers
 Smooth m contraction at trigone & bladder neck (alpha receptors) Parasymp. supply causes detrusor contraction (muscarinic receptors) Pudendal supply causes striated sphincter contraction. Within the spinal cord, information from bladder afferents integrated with other sources and projected to brain stem centers to coordinate with mic. centers.")
7
Development of Normal Bladder Function and Micturition Control
CMG studies on normal infants showed bladder function in young children is very different from adults During the 1st 2-3 years of life There is progressive development from initially indiscriminate infants voiding pattern to more socially conscious and voluntary (adult) type of micturition
 type of micturition.")
8
The natural evolution of bladder control entails nervous system & depends on:
Progressive increase in bladder functional storage capacity Maturation of voluntary control over the urethral striated muscle sphincter Development of direct volitional control over the bladder sphincter unit, so that the child can voluntary initiate or inhibit micturition reflex

9
Change in bladder function parameters
Voiding frequency During the 3rd trimester, the fetus voids at rate 30 times/24 hrs Immediately after birth, this drops for the 1st days only Increases again after 1st 1/52 to reach a peak by 2-4 /52 to an average once/hour This rate declines to times/day at 6-12 mo. 8-10 times/day by 2-3 years

10
This reduction in voiding frequency observed during the 1st years of life related mainly to an increase in bladder capacity parallel to body growth By the age of 12, voiding pattern is very similar to that in adult ( 4-6 voids / day )
")
11
Bladder capacity can be estimated
An adequate reservoir function of urine storage is necessary to meet the increase rate of urine production and decreased voiding frequency in the growing child Bladder capacity can be estimated For young infants: Bladder capacity (ml) = * age (mo) For children: Bladder capacity (ml) = (age [yr] + 2) * 30 koff’s formula Bladder capacity (ml) = 30 + (age [yr] * Hijalma’s formula
 = * age (mo) For children: Bladder capacity (ml) = (age [yr] + 2) * 30 koff’s formula. Bladder capacity (ml) = 30 + (age [yr] * 30 Hijalma’s formula.")
12
In parallel to increase in bladder capacity, the mean voided volume of each micturation increases with age CMG studies showed that most infants with incomplete maturation of det.- sphin. coordination before the age 1, are still able to have satisfactory emptying (>80) There are limited studies on detr. pressure at voiding in infants due techn. difficulties
 There are limited studies on detr. pressure at voiding in infants due techn. difficulties.")
13
Limited data documented higher maximum detr. pressure with mict
Limited data documented higher maximum detr. pressure with mict. than in adults Male infants voided significantly higher pressure than females (mean Pdetmax 118 vs. 75cm H20, P<.03) Studies showed that high detrusor pressures noted during micturition were mainly observed only during the 1st year of life & decreased progressively with age
 Studies showed that high detrusor pressures noted during micturition were mainly observed only during the 1st year of life & decreased progressively with age.")
14
Evolution of Normal Micturition Control
Traditionally, it has been assumed that micturition occurs by simple spinal reflex with no mediation by higher neural centers Recent studies showed that even in full term fetuses and newborns, mict. Is modulated by higher centers Further extensive modulation occurs during the postnatal period

15
The final steps usually achieved at 3-4 yrs
During the 2nd & 3rd year of life, there is a progressive development toward a socially conscious continence and a more voluntary (adult) type mict. The final steps usually achieved at 3-4 yrs Most develop the adult pattern of urinary control & will be dry day & night The child has learned to inhibit a mict. Reflex and postpone voiding and voluntarily initiate mict. At socially acceptable time & place
 type mict. The final steps usually achieved at 3-4 yrs. Most develop the adult pattern of urinary control & will be dry day & night. The child has learned to inhibit a mict. Reflex and postpone voiding and voluntarily initiate mict. At socially acceptable time & place.")
16
bladder is unique among other visceral organs
Neurologic control of normal mic. occurs at different levels of CNS from the spinal cord (sacral mic. centers) to the brain stem (pontine mic. Centers) Cerebellum, basal ganglion, limbic system, thalamus and hypothalamus, and cerebral cortex bladder is unique among other visceral organs its function is under control of somatic and autonomic n. system Beside acetylcholine & NE, other neurotransmitters involved during bladder stimulation PG substance P, Opioid, vasoactive intestinal peptide, neuropeptide Y
 to the brain stem (pontine mic. Centers) Cerebellum, basal ganglion, limbic system, thalamus and hypothalamus, and cerebral cortex. bladder is unique among other visceral organs. its function is under control of somatic and autonomic n. system. Beside acetylcholine & NE, other neurotransmitters involved during bladder stimulation. PG substance P, Opioid, vasoactive intestinal peptide, neuropeptide Y.")
17
Transitory Detrusor-Sphincter Discoordination in Infancy
Studies showed that all children may transiently display some degree of abnormal bladder-sphincter function Urodynamic findings show association of high voiding pressures and interruption of flow BUT no impairment of overall bladder empting This type of dysfunction resolved with a period of successful toilet training, transient or intermittent, and does not persist

18
Non-Neuropathic Bladder Sphincter Dysfunction in Children

19
Dysfunctional voiding may
Reported 15 % of 6-year old children suffer from Non-Neuogenic B.S.Dysfunction Dysfunctional voiding may starts with detrusor instability with sphincter & pelvic floor overactivity then develops gradually fractionated voiding with increasing PVR Finally, develops bladder decompensation and the lazy bladder syndrome Distinction between Neuropathic & Non-neuropathic bladder dysfunctions may not be clear

20
The term non-neuropathic is based purely on the fact that no obvious and identifiable neurologic lesions can be identified In adults, lower urinary tract function has been well understood and standardization of terminology has been established In contrast, neural control over the bladder-sphincter unit in children is age dependent and is much more variable and complex

21
General Etiologic Classification of Bladder Dysfunction
Derangement of Nervous Control: Congenital malformation of CNS, e.g.: myelomeningocele, spina bifida, caudal regression synd., tethered cord Developmental disturbances, e.g.,: Mental retardation, dysfunctional voiding, urge synd. Acquired conditions, e.g.: CP, progressive degenerative diseases of CNS, transverse myelitis, MS, vascular malformations, trauma of spinal cord

22
Disorders of Detrusor & Sphincteric Muscle function:
Congenital conditions Muscular dystophy, neuronal dyplasia Acquired conditions Chronic bladder distension, fibrosis of detrusor & bladder wall Structural abnormalities Bladder extrophy, epispadias, cloacal anomoly, uretroceles, PUV, prune belly syndrome Traumatic stricture, damage to sphincter or urethra Other unclassified conditions Giggle incontinence Hinman syndrome Ochoa syndrome (urofacial syndrome)
")
23
Functional classification of bladder dysfunction
based on functional state of the bladder-sphincter complex with respect of detrusor activity bladder sensation bladder compliance and function urethral function during the filling & voiding phase of CMG

24
During the filling phase:
Detrusor activity Normal or stable Overactive : phasic involuntary detrusor contractions which occur spontaneously or provoked by alteration of posture, coughing, walking, jumping Unstable: contraction unrelated to underlying neurologic disorder Detrusor hyperreflexia : overactivity related disturbance of neural control mechanism

25
Bladder sensation during filling phase:
Normal / hypersensitive / hyposensitive / absent Bladder capacity normal/ / high / low Compliance Normal / high / low Urethral function Normal / incompetent

26
During the voiding phase
Detrusor activity Normal: Voiding achieved by voluntarily initiated detrusor contractions that is sustained and cannot usually suppressed voluntarily until after 4 year old Underactive Acontractile Urethral function Normal obstructive

27
Bladder-Sphincter dysfunction during filling
Overactive (unstable) bladder, urge syndrome, urge incontinence Traditionally the infant bladder has been described as unstable or uninhibited Recent studies showed that bladder is normally quiescent and stable even in newborn Clinically, the condition of (unstable bladder) is best exhibited by URGE SYNDROME with or without urge incontinence
 bladder, urge syndrome, urge incontinence. Traditionally the infant bladder has been described as unstable or uninhibited. Recent studies showed that bladder is normally quiescent and stable even in newborn. Clinically, the condition of (unstable bladder) is best exhibited by URGE SYNDROME with or without urge incontinence.")
28
Urge incontinence consists of small quantities of urine loss
Urge syndrome characterized frequent attacks of sudden and imperative sensations of urge due to detrusor overactivity during filling (girls>boys) The unstable contractions are often counteracted by voluntary contractions in the pelvic floor muscles to externally compress the urethra (hold maneuvers) exhibited as squatting in many cases Urge incontinence consists of small quantities of urine loss More in afternoon when the child plays and is not alert enough to contract the pelvic floor in response to the urge sensation
 The unstable contractions are often counteracted by voluntary contractions in the pelvic floor muscles to externally compress the urethra (hold maneuvers) exhibited as squatting in many cases. Urge incontinence consists of small quantities of urine loss. More in afternoon when the child plays and is not alert enough to contract the pelvic floor in response to the urge sensation.")
29
Functional urinary incontinence
Defined as involuntary loss of urine due to failure of control of bladder sphincter unit, frequent enough to cause social or hygienic problem with the absence of underlying anatomic causes Stress incontinence represents involuntary leakage of urine occurring when the intravesical pressure exceeds the bladder outlet or urethral pressure in the absence of measurable detrusor contractions Unlike adults, true stress incont. Extremlely uncommon in neurologically normal children and generally not associated with abnormal CMG

30
Giggle incontinence: Involuntary and typically unpredictable wetting during giggling or laughter In contrast to stress incontinence, it produces much larger volume of urine leak amounting to complete bladder emptying CMG may be normal or occasionally demonstrate some detrusor overactivity Rx is difficult bt sometimes a course of anticholinergic drugs may help Some suggested that it’s centrally mediated and hereditary disorder that may respond to CNS stimulants as methylphenidate

31
Bladder-Sphincter dysfunction during bladder emptying
Dysfunctional voiding Characterized by incomplete relaxation or overactivity of the pelvic floor muscles during voiding Can manifest in different patterns depending on the degree of outflow obstruction caused and the status of the detrusor activity

32
Staccato and fractionated voiding
In staccato voiding the urinary stream is often delayed after the onset of detrusor contraction and is typically interrupted resulting in a few small squirts of urine passed in quick sensation Interrupted voiding caused by periodic bursts of pelvic floor muscle activities during micturition resulting in characteristic abrupt elevation of voiding pressure coinciding with paradoxical cessation of urinary flow Flow time usually prolonged and bladder emptying incomplete

33
Fractionated voiding is characterized by infrequent & incomplete emptying secondary to detrusor inactivity Micturition occurs in several small discontinuous fractions due to poor detrusor contractions Significant PVR Abdominal straining usually evident to improve emptying Straining paradoxically counteracted by reflex increase in pelvic floor muscles that is triggered by increase in intravesical pressure

34
Infrequent voiding and (lazy bladder) syndrome
Described together as they represent a spectrum of diseases that are more commonly occurs in girls The lazy bladder syndrome is generally regarded as the endpoint of long standing dysfunctional voiding occurring in a fully decompensated system Due to chronic functional outflow obst., there is gradual deterioration in detrusor contractility and emptying efficiency PVR & bladder capacity increase progressively with inefficient emptying

35
Bcs urge sensation is either absent or diminished, voiding is very infrequent and occasionally the child may not void for 8-10 hrs or longer if engaged in activity Typical presentation, the mother always complains that the child never voids unless told to do so Other presentations Recurrent UTI, Overflow incontinence, constipation CMG findings Large bladder capacity, very high compliance on filling, absent detrusor contractions, voiding associated with increased abdominal pressures

36
Hinman’s Syndrome & Occult Neuropathic bladder
Different names: Nonneurogenic neurogenic bladder / subclinical neurogenic bladder / Hinman syndrome / occult neuropathic bladder Acquired form of bladder-sphincteric dysfunction in children characterized by a combination of bladder decompensation with incontinence, poor emptying, and recurrent UTI Most children have significant bowel dysfunction Has all the clinical & CMG features of neuropathic dysfunction but NO neuologic pathology CMG shows marked sphincteric overactivity with abrupt contractions of pelvic floor

37
Ochoa (urofacial) syndrome:
Children have all classic features of dysfunctional voiding, including urinary incontinence, recurrent UTI, constipation, reflux, Upper tract damage + peculiar painful or apparently crying facial expression during smiling Autosomal recessive, located on chromosome 10 CMG shows sustained contraction of external sphincter during voiding

38
Of 66 children reported by Ochoa:
33% renal functional impairment 26% HTN 24% ESRD Bcs neural ganglion controlling the facial muscles are situated very close to the pontine micturition centers A small genetically predetermined congenital neurologic lesion in this area may be responsible for both the peculiar facial expression & bladder dysfunction

39
Postvoid dibbling Involuntary leakage of urine immediately after voiding Refers to post toilet trained girls who dribble soon after standing up after a void and otherwise normal with no other urinary symptoms May be result of vesicovaginal reflux where urine is trapped in the vagina during voiding & once the child stands, the urine dribble out When in doubt, can be confirmed by MCUG Harmless, tends to resolve with age Child may be taught to empty her vagina by simply voiding with her thigh apart & leaning forward after voiding before getting up

40
Dysfunctional Elimination Syndrome, Constipation, & Bladder Dysfunction
DES refers to broad spectrum of functional disturbances that may affect the urinary tract including that of functional bowel disturbances The close proximity of the rectum to posterior bladder wall make it possible that gross distension of the rectum by impacted feces can result in mechanical compression of the bladder & bladder neck leading to urinary obstruction

41
Classified as : Functional disorder of filling
Overactive, overdisteded, insensate bladder, may be associated with fecal impaction or rectal distension with infrequent call to stool Functional disorder of emptying Over recruitment of pelvic floor activity during voiding causing interrupted / incomplete emptying, with defecation difficulties due to nonrelaxation of puborectalis or pain on defecation

42
After successful Rx of constipation
DES influenced the clinical outcome of ureteric reimplantation surgery for VUR Children with constipation had the highest likehood of developing breakthrough UTI & requires surgery DES had an adverse effect on the rate of spontaneous reflux resolution requiring an average 1.6 years longer to outgrow reflux than in children without DES After successful Rx of constipation 89% of those with daytime incontinence and 63% of nighttime incontinence became dry Loening-Baucke et al (1997) Management of the underlying dysfunction should be given priority in the treatment protocol of children with conditions such as VUR / incontinence / UTI bsc successful Rx may significantly improve outcome
 Management of the underlying dysfunction should be given priority in the treatment protocol of children with conditions such as VUR / incontinence / UTI bsc successful Rx may significantly improve outcome.")
43
Relationship Betw. Bladder Sphincter Dysfunction, VUR, & Recurrent UTI
Impairment in the function of lower tract often coexists with recurrent UTI & VUR without neurologic pathology The most common abnormalities of lower tract coexist with VUR are Detrusor overactivity Uncoordinated detrusor sphincter during voiding Reflux may be worsened by detrusor instability

44
Male refluxers have higher maximum detrusor pressure > female
Studies showed that infants with UTI & VUR have high prevalence of high voiding detrusor pressure Male refluxers have higher maximum detrusor pressure > female May be due to high urethral resistance of the longer male urethra and smaller urethral meatus with anatomic difference in the external urethral sphincter Spontaneous resolution of VUR may be delayed in presence of abnormal dynamics of the bladder Successful Rx of underlying bladder dysfunction result in marked increase in the rate of spontaneous resolution of reflux & recurrent UTI X & reduction of UT

45
Evaluation of Non-Neurogenic Bladder Sphincter Dysfunction
History Majority present after toilet training with symptoms of nighttime / daytime urinary incontinence or both May present earlier with UTI or VUR Hx should include questions to exclude neurologic & congenital abnormalities Bowel dysfunction can coexist in the form of encorpresis, constipation and fecal impaction Urinary Hx should include symptoms of storage & voiding of urine

47
Physical examination:
Usually normal Careful examination is required Occasionally, palpable bladder may be found External genitalia examination Abnormalities of lower spine Neural tubal defect Asymmetrical gluteal folds Hairy patch Dermovascular malformation Lipomatous abnormality of sacral region Rectal exam. may reveal impacted stool

48
Laboratory Not routinely required
Urinanalysis may be performed to R/O bacteruria & glucosuria Serum & urine osmolarity may be looked in case of nocturnal enuresis

49
Ultrasound 1st line investigation
Simple, reliable, available, & noninvasive tool Provides anatomical & functional problems Recently used to measure bladder parameters used in calculating bladder volume & wall thickness index (BVWI) BVWI classified into normal / thick / thin Studies showed these classifications corresponded closely to CMG findings of bladder dysfunctions This classification can act as reliable tool to guide for further invasive investigations
 BVWI classified into normal / thick / thin. Studies showed these classifications corresponded closely to CMG findings of bladder dysfunctions. This classification can act as reliable tool to guide for further invasive investigations.")
50
Other imaging studies:
Radiologic examination of the spine may be necessary to exclude neuologic causes MCUG may be needed to R/O VUR & to assess the status of the urethra Urodynamics studies: To describe the physiologic parameters involved in bladder mechanics during filling & voiding

51
Urodynamics (cont.) Uroflow
In children, normal flow rate are different from adults Usually there is poor correlation betw. Qmax & outflow resistance Bcs the detrusor is able to exert much stronger contractions to counteract any increased resistance Pattern of flow curve is important

52
Patterns of uroflow curve:
Bell shape : normal Tower shape : produced by explosive voiding contractions which is seen in overactive bladder Low plateau : representative of outlet obstruction Staccato pattern : seen with sphincteric overactivity during voiding with peak and throughs throughtout voiding Interrupted voiding : seen in a contractile or underactive bladder

53
Urodynamics (cont.) Conventional fill urodynamic studies
Bladder catheter introduced transurethrally or suprapubically The use of SPC has been suggested as a better alternative to transurethral catheterization Natural fill urodynamic studies The child is asked to drink to allow the bladder to fill up on its own rate Artificial filling may inhibit the detrusor response and attenuate its maximum contractile potential, making detrusor instability less pronounced & undetectable Natural fill cystometry is the preferred technique in children The combined use of artificial & natural filling CMG is helpful to accurately delineate the underlying bladder dysfunction

54
Ambulatory urodynamic studies

55
Management of Non-Neuropathic Bladder-Sphincter Dysfunction
Behavior Modification & standard Urotherapy Urotherapy is a nonpharmacologic nonsurgical combination of cognitive, behavioural, & physical therapy to normalize micturiton pattern & prevent functional disturbances of lower tract Children & parents education on proper voiding mechanics Instructions how and when to void Teaching children correct positions during voiding

56
Behavior Modification & standard Urotherapy (cont.)
Teaching how to relax the pelvic floor and avoid straining Modification of drinking and voiding habits to include proper hydration with timed voiding Assessment of their bowel function

57
Urotherapy. Pelvic floor rehabilitation with real time biofeedback monitoring

58
Biofeedback and pelvic floor rehabilitation
Biofeedback is based on the concept of building self perception on detrusor contractions and pelvic floor relaxation in the pt By combining uroflow with real time monitoring, child is able to see how well he / she is voiding Biofeedback is proven to be highly effective either on its own or in combination with standard urotherapy

59
Urotherapy. Biofeedback with real time uroflowmetry

60
Neuromodulation Recent studies reported that transcutaneous electrical nerve stimulation (TENS) is simple, cost effective, noninvasive treatment modality The use of low frequency electrical current to inhibit detrusor activity in adults is common Appears to modulate excitatory & inhibitory components of bladder control
 is simple, cost effective, noninvasive treatment modality. The use of low frequency electrical current to inhibit detrusor activity in adults is common. Appears to modulate excitatory & inhibitory components of bladder control.")
61
Bowel management Principles include rectal emptying of impacted stool and maintenance of regular soft stools Oral laxatives or rectal enemas Dietary modification Correct toilet posture & correct recruitment of abdominal muscles in the defecation process Parental education

62
Medications Antimuscarinic agents
These agents are the gold standard in Rx of overactive bladder Muscarinic receptors are found in detrusor muscle Bladder contractions are initiated by stimulation of these receptors with the release of Ach from cholinergic n. Main action of antimuscarinic drugs on M1 & M3 receptor subtypes, thought to be responsible of detrusor overactivity

63
Antimuscarinic agents (cont.)
Antimuscarinic, such as Oxybutynin, act by reducing the frequency & intensity of involuntary contractions causing increase in functional bladder capacity The nonselective pattern of activity and penetration of BBB are known to induce systemic & central S/E

64
Alpha adrenergic blockers
The density of the noradrenergic nerves increases markedly toward the bladder neck particularly in males The normal response to NE is relaxation & contraction of the bladder neck Alpha blockers used in pts with evidence of bladder neck dysfunction for relaxation of bladder neck

65
Other medications Tricyclic antidepressents E.g. impiramine
Effective in increasing urine storage by decreasing detrusor contractility & increasing outlet resistance Precise mechanism is not clear Possible effect on bladder by inhibition of NE reuptake, producing alpha adrenergic stimulation Associated with high S/E

66
Beta-Adrenergic agonists
Can cause significant increase in bladder capacity Bt can also cause significant CVS S/E Parasympathicomimetics / Ca antagonists / K Ch. Openers / PG inhibitors Rarely used in children due to unfavorable S/E or to lack of proven efficacy

67
Clean intermittent Catheterization
Necessary in pts with decompensated bladders or lazy bladder syndrome Regular emptying of the bladder to achieve low pressure emptying which improves detrusor contractility & bladder emptying function Some of these children may be able to eventually be weaned from use of this procedure

68
Surgery Indicated when conservative management with nonpharmacologic & pharmacologic Rx fails Bladder augmentation may be performed to to produce low pressure system with increased bladder capacity Augmentation using intestinal segments such as colon / ileum / stomach Augmentation has its metabolic complications

69
Surgery (cont.) Surgical means has been employed to reduce urethral / sphincteric pressure as alternative to alpha blockers Ballon dilatation of bladder neck & botulinum A toxin injection into the sphincter has been used Requires repeated attempts ? Long term effect & efficacy

70
Neuropathic Dysfunction of Lower Urinary Tract

71
Neuropathic Dysfunction of Lower Urinary Tract
Neurospinal dysraphisms Myelodysplasia Lipomeningocele & other spinal dysraphisms Sacral agenesis Central nervous system insults Cerebral palsy Traumatic injuries to the spine

72
Neurospinal dysraphisms
Myelodysplasia The most common cause of neurogenic bladder dysfunction in children Formation of spinal cord & vertebral column begins at 18th day of gestation Closure of canal proceeds in caudal direction Closure complete at 35 days ? Mechanism that results in closure and wt produces dysraphism

73
Incidence reported 1 / 1000 births
Incidence increases with more than one member affected The medical Research Council Vitamin Study Group recommends that women of childbearing age take 4mg/d of folic acid beginning at least 2/12 before pregnancy Folate deficiency can lead to myelodysplastic abnormality

74
Relationship Incidence General population Mother with one affected child 20-50 Mother with two affected children 100 Patient with myelodysplasia 40 Mother older than 35 years 30 Sister of mother with affected child 10 Sister of father with affected child 3 Nephew who is affected 2

75
Lipomyelomeningocele
Myelodysplasia various abnormal conditions of the vertebral column that affect spinal cord function Meningocele Occurs when just the meninges ( no neual elements ) extend beyond the confines of vertebral canal Myelomeningocele Neural tissue, either nerve root or portions of spinal cord has evaginated with the meningocele Lipomyelomeningocele Fatty tissue has developed with the cord structures and both extend with the protruding sac
 extend beyond the confines of vertebral canal. Myelomeningocele. Neural tissue, either nerve root or portions of spinal cord has evaginated with the meningocele. Lipomyelomeningocele. Fatty tissue has developed with the cord structures and both extend with the protruding sac.")
76
Cervical-high thoracic
Myelomeningocele accounts for > 90% of all open spinal dysraphic states Most spinal defects at lumber vertebrae Location Incidence (%) Cervical-high thoracic 2 Low thoracic 5 Lumbar 26 Lumbosacral 47 Sacral 20
 Cervical-high thoracic. 2. Low thoracic. 5. Lumbar. 26. Lumbosacral. 47. Sacral. 20.")
78
It may be opened with CSF leak
Usually, the meningocele is made of flimsy covering of transparent tissue It may be opened with CSF leak For this reason, urgent repair is necessary Sterile precautions should be applied after birth till time of repair 85 % associated with Arnold-Chiari malformation Cerebral tonsils herniate down through the foramen magnum Herniation causes obstruction of the 4th ventricle & preventing the CSF from entering the subarchnoid space

79
Neurologic lesion produced by this condition varies
It’s possible that leakage of CSF from the open spinal column accounts for herniation of posterior brain stem down the foramen magnum hydrocephalus Neurologic lesion produced by this condition varies Depending on what neural element have everted with the meningocele sac The bony vertebral level often provides little or no clue to the exact neurologic lesion produced 10% of newborn with MM exhibit no abnormality in CMG 24% of children with normal lower tract at birth, develop upper motor neuron changes over time

80
Newborn assessment Renal U/S with measurement of post void residual is performed as early as possible after birth Before / after closure of spinal defect CMG is delayed until it’s safe to transport the child to the urodynamic suit and place him on the back or side for the test If the infant cannot empty the bladder after spontaneous void or with Crede maneuver, CIC is begun even before CMG is done If Crede maneuver is effective in emptying the bladder, it’s performed at regular basis instead of CIC until lower tract is fully evaluated

81
The normal bladder capacity in newborn is 10-15ml
Residual urine of <5 ml is acceptable Other tests should be performed Urinanalysis & culture Serum creatinine Careful neurologic examination of LL Once spinal closure has healed sufficiently Renal U/S & renal scan for reassessment of upper tract VCUG CMG

82
Findings 15-20% of newborns have abnormal urinary tract on radiological exam. when first evaluated 3% have hydro 2ndry to spinal shock, probably from spinal canal closure 15% have abnormalities that develop in utero as result of abnormal lower tract due to outlet obstruction CMG in newborn showed that 63% have bladder contractions A combination of bladder contractility & external sphincter activity results in synergic (26%) Dyssynergic with / out poor detrusor compliance (37%) Complete denervation (36%)
 Dyssynergic with / out poor detrusor compliance (37%) Complete denervation (36%)")
83
This categorization of lower tract function has been useful bcs it reveals
Which child is at risk for urinary tract changes Who should be treated prophylactically Who needs close surveillence Who can be monitored at great intervals It appears that outlet obstruction is a major contributor to the development of urinary tract deterioration

84
Recommendations Expectant management revealed that infants with outlet obst. in the form of DSD are at considerable risk for urinary tract deterioration These pts should be treated prophylactically CIC alone OR in combination with anticholinergic when Detrusor filling pressures > 40 cm H2O Voiding pressures > cm H2O Resulted in an incidence of urinary tract deterioration of only 8-10%

85
Oxybutynin hydrochloride administered in a dose of 1 mg / year of age BID
In neonates & children < 1year, dose < 1mg & increase proportionally as the age reaches 1 year On rare occasions when overactive or poor compliant bladder fails to respond, augmentation cystoplasty may be needed

86
Neurologic findings & recommendations
Neurologic lesion in myelodysplasia is a dynamic disease process in which changes take place throughout childhood When a change is noted on neurologic, orthopedic, or urodynamic assessment, radiologic investigation of the CNS often reveals Tethering of the spinal cord A syrinx or hydromyelia of the cord Increased intracranial pressure due shunt malfunction Partial herniation of the brain stem and cerebellem

87
MRI is the test of choice as it reveals anatomic details of the spinal column & CNS
Sequential urodynamics testing on yearly basis beginning in the newborn period and continuing until 5 yrs old It may be necessary to repeat CMG if upper tract dilates 2ndry to impaired drainage from a poor compliant detrusor

88
Surveillance in infants with myelodysplasia
Sphincter Activity Recommended Tests Frequency Intact-synergic Postvoid residual volume q 4 mo IVP or renal echo q 12 mo UDS Intact-dyssynergic† VCUG or RNC‡ Partial denervation UDS§ Complete denervation q 6 mo Renal echo

89
Management of VUR VUR occurs in 3-5 % of newborns with myelodysplasia
Usually associated with poor detrusor compliance, detrusor overactivity or DSD If untreated, incidence of VUR in these infants at risk increases with time until 30-40% affected by 5 years of age

90
Children with poor detrusor compliance with / out hydro
VUR grade 1-3 who void spontaneously or who have complete lesions with little or no outlet resistance with good bladder emptying Prophylactic Abx only High grade reflux CIC to ensure complete emptying Children who cannot empty their bladder spontaneously regardless of the grade Treated with CIC Children with poor detrusor compliance with / out hydro To add anticholenergic drugs to lower intravesical pressure and ensure adequate upper tract decompensation

91
Bacteriuria occurs in 56% of children with CIC & not harmful
Except in presence of high grade reflux Symptomatic UTI & renal scarring rarely occurs in lesser grades of reflux Crede maneuver should be avoided in children with reflux, especially those with reactive external sphincter It results in a reflex response in external sphincter that increases urethral resistance & raises the pressure needed to expel urine from bladder Aggravating the degree of reflux & accentuating its water hammer effect on kidneys

92
Vesicostomy drainage rarely required today but indicated in
Infants who has severe reflux that CIC & anticholenergic fail to improve upper tract drainage Parents cannot adapt to catheterization program Who are not good candidates for augmentation cystoplasty

93
The indications of antireflux surgery are not very different from those with normal bladder
Recurrent symptomatic UTI while receiving adequate Abx therapy & appropriate CIC techniques Persistent hydro despite effective emptying of the bladder & lowering of intravesical pressure Severe reflux with anatomic abnormality at the UVJ Reflux that persists into puberty Presence of reflux in any child undergoing surgery to increase outlet resistance

94
Antireflux surgery can be very effective in children with neurogenic bladder dysfunction as long as it’s combined with measures to ensure complete bladder emptying Since the advent of CIC, success rate for antireflux surgery approached 95 % The endoscopic injection of Deflux has altered the management of reflux in children with MM Its long term effects are yet to be appreciated

95
Continence Initial attempts at achieving continence include CIC & drug therapy to maintain low intravesical pressure Drugs Glycopyrrolate (Robinol) : most potent oral anticholenergic drug available today same other S/E Tolteradine (Detrol): newly approved, equally effective as oxybutynin with fewer S/E Hyoscyamine (levsin) : potency less, fewer S/E Intravesical oxybutynin : fewer S/E compared to oral
 : most potent oral anticholenergic drug available today same other S/E. Tolteradine (Detrol): newly approved, equally effective as oxybutynin with fewer S/E. Hyoscyamine (levsin) : potency less, fewer S/E. Intravesical oxybutynin : fewer S/E compared to oral.")
96
Alpha sympathomimetic agents
Botulinum roxin A injected into the detrusor muscle has been effectively used Paralyzes the bladder for varying period of time May become viable Rx in the future Alpha sympathomimetic agents If CMG reveals that urethral resistance is inadequate to maintain continence Phenylpropanolamine is the most effective agent

97
Surgery Viable option when drug therapy fails to achieve continence
Generally intervention is delayed till 5 yrs old Enterocystoplasty using sigmoid, cecum & small intestine If bladder neck or urethral resistance is insufficient to allow adequate storage, bladder neck reconstruction is considered

98
Currently, Deflux injections at the bladder neck are being advocated
enhances outlet resistance Alternative to bladder neck reconstruction No long term data Continent urinary diversion with closure of bladder neck has been used to provide better quality of life for intractable urethral incompetence

99
Sexuality In several studies, 28-40% of MM had one or more sexual encounters All of them had a desire to marry & to bear children In one study, 72% of male subjects have erection, 2/3 were able to ejeculate Other studies revealed 70-80% of MM women were able to become pregnant

100
The degree of sexuality is inversely proportional to the level of neuologic dysfunction
Boys reach puberty at age similar to normal boys In MM Girls, breast development & menarche start 2 yrs earlier than usual normal girls

101
Bowel function The external anal sphincter i innervated by the same nerves that modulate the external urethral sphincter The internal anal sphincter is influenced by more proximal n. from sympathatic nervous system The internal sphincter reflexively relaxes in response to anal distension Consequently, bowel incontinence is frequently unpredictable Incontinence not associated with the attainment of urinary incontinence

102
Lipomeningocele & other Spinal dysraphism
Group of congenital defects that affects the formation of spinal column but do not result in open vertebral canal Incidence of lipomeningocele in families 0.043% Lesion have no obvious outward signs

103
Types of occult spinal dysraphisms
Lipomeningocele Intradural lipoma Diastematomyelia Tight filum terminale Dermoid cyst/sinus Aberrant nerve roots Anterior sacral meningocele Cauda equina tumor

104
>90% have cutaneous abnormalities overlying the spines
Small dimple Skin tag to a tuft of hair Dermal vascular malformation Very noticeable subcutaneous lipoma Asymmetrically curving gluteal cleft Careful inspection of the legs may show high arched foot / alterations in the configuration of the toes / discrepancy in muscle size / shortness / decreased strength in one leg typically the ankle / gait abnormality

105
Small lipomeningocele
Hair patch dimple Dermal vascular malformation Abnormal gluteal cleft

106
Abnormal lower tract function in 40-90%
Absent perineal sensation / back pain / secondary incontinence may be noted Abnormal lower tract function in 40-90% Abnormality increase with age Difficulty with toilet training Urinary incontinence after period of dryness Recurrent UTI Fecal soiling

107
Majority perfectly normal neurologic examination CMG
Abnormal lower tract function in 1/3 of infants < 18/12 Most likely abnormality is UMN lesion characterized by overactive bladder &/or hyperactive sacral reflexes Rarely, mild form of DSD LMN signs occurs in 10% only

108
All children > 3 yrs who have not been operated on OR whom occult dysraphism has been lately diagnosed Have upper or lower lesion or in combination on CMG (92%) within 2 yrs When observed expectantly from infancy after Dx was made, 58% deteriorate
 within 2 yrs. When observed expectantly from infancy after Dx was made, 58% deteriorate.")
109
Pathogenesis Various occult spinal dysraphic lesions produces different neuologic findings, Reasons: Compression on the cauda equina or sacral n. roots by expanding lipoma or lipomeningocele Tension on the cord from tethering 2ndry to differential growth rates in bony vertebrae and neural elements while the lower end of the cord is held in place by lipoma or thickened filum terminale Fixation of the split lumbosacral cord by intervertebral bony specule or fibrous band

110
Normally, the conus medullaris ends just below the L2 vertebraae at birth and recedes upward to T12 by adulthood When the cord does not rise or fixed in place bcs of these lesions, ischemic injury may ensue Correction of the lesion in infancy result not only in stabilization, bt also in improvement in the neurologic pictures in many instances

111
Recommendations MRI Spinal U/S in children < 3/12 At this age, vertebral bones have not ossified Useful screening tool for visualization of spinal canal Currently, most NS advocates laminectomy & removal of the intraspinal process as completely as possible, without injuring nerve roots or cord to release the tether and prevent further injury from subsequent growth

112
Sacral Agenesis The absence of part or all of 2 or more lower vertebral bodies Teratogenic factors play a role IDDM mothers have 1% of giving birth to a child with sacral agenesis 16% of children with sacral agenesis have a mother with IDDM Maternal insulin-Ab complexes noted to cross the placenta

113
Deletion of chr.7q36 has a role
Maternal drug exposure (Minoxidil) reported to cause sacral agenesis Familial cases if sacral agenesis associated with Curarino syndrome Presacral mass Sacral agenesis Anorectal malformation Deletion in chr.7, leading to HLXB9 genetic mutation
 reported to cause sacral agenesis. Familial cases if sacral agenesis associated with Curarino syndrome. Presacral mass. Sacral agenesis. Anorectal malformation. Deletion in chr.7, leading to HLXB9 genetic mutation.")
114
Diagnosis of sacral agenesis
Presentation bimodal ¾ at early infancy Remainder at 4-5 yrs can be Dx parentally due to frequent use of U/S If not detected prenatally or at birth, Dx is delayed May present with failed attempts at toilet training Sensation intact & lower limb function is normal usually

115
The only clue beside the high index of suspicion is
Flattened buttocks Low gluteal cleft Palpation of the coccyx is used to detect absent vertebrae Dx confirmed with a lateral film of lower spine MRI is diagnostic

116
Gluteal crease is short
and seen only inferiorly

118
Findings CMG UMNL UMNL - 35% LMNL - 40%
No signs of denervation at all - 25% UMNL Overactive detrusor Exaggerated sacral reflexes Absence of voluntary control over sphincter function DSD no sphincteric deenervation Bladder is thick wall (or trabeculated), with closed bladder neck on VCUG or U/S
, with closed bladder neck on VCUG or U/S.")
119
UTI present in 75% over time
LMN Acontractile detrusor Partial or complete denervation of external sphincter Diminished or absent sacral reflexes Bladder smooth and small with opened bladder neck The presence or absence of bulbocavernous reflex is an indicator of an UMNL / LMNL respectively UTI present in 75% over time VUR occurs in UMNL (75%) and in LMNL (40%)
 and in LMNL (40%)")
120
Recommendations CMG / Ultrasound / VCUG or nuclear cystography UMNL
Anticholinergic +/- CIC If anticholinergic ineffective in controlling overactive detrusor, augmentation cystoplasty required

121
LMNL + Rx bowel dysfunction
CIC & alpha sympathomimetics drugs for those who cannot empty the bladders or stay dry between CIC Injection of bulking agents Artificial urinary sphincter implantation + Rx bowel dysfunction

122
Associated conditions with sacral agenesis
Imperforate anus Alone or part of anomalies ( VATER / VACTERL ) Male > female 1.5:1 Sacral agenesis occurs with spectrum of hindgut abnormalities in Currarino syndrome Associattion with fistula to the lower tract is common Most common findings on CMG UMNL with overactive bladder And or DSD
 Male > female 1.5:1. Sacral agenesis occurs with spectrum of hindgut abnormalities in Currarino syndrome. Associattion with fistula to the lower tract is common. Most common findings on CMG. UMNL with overactive bladder. And or DSD.")
123
CNS insults Cerebral palsy
Nonprogressive injury of the brain occurring in the perinatal period that produces either a neuromuscular disability, a specific symptom complex, or cerebral dysfunction Incidence is 1.5 / 1000 births Lesions classified according to which extremities involved and wt kind of dysfunction Spastic diplegia is the most common

124
With rectovaginal fistula Without fistula
Female Male High Anorectal agenesis With rectovaginal fistula Without fistula With rectourethral (prostatic) fistula Rectal atresia Without fistula Intermediate Rectovestibular fistula Rectovaginal fistula Rectovestibular urethral fistula Anal agenesis without fistula Low Anovestibular fistula Anocutaneous fistula Anal stenosis Rare malformation Cloacal malformation
 fistula. Rectal atresia. Without fistula. Intermediate. Rectovestibular fistula. Rectovaginal fistula. Rectovestibular urethral fistula. Anal agenesis without fistula. Low. Anovestibular fistula. Anocutaneous fistula. Anal stenosis. Rare malformation. Cloacal malformation.")
125
Most children has total urinary control
23.5% has persistent incontinence The presence of incontinence is often related to the extent of physical impairment Abnormal bladder & urethral sphincter function was found in almost all

126
Type Number % Upper motor neuron lesion 49 86 Mixed upper +lower motor neuron lesion 5 9.5 Incomplete lower motor neuron lesion 1 1.5 No urodynamic lesion 2 3

127
Uninhibited contractions 35 Detrusor sphincter dyssynergy 7
Type of Lesion No. of Patients Upper motor neuron Uninhibited contractions 35 Detrusor sphincter dyssynergy 7 Hyperactive sacral reflexes 6 No voluntary control 3 Small-capacity bladder 2 Hypertonia Lower motor neuron Excessive polyphasia 5 ↑ Amplitude +↑ duration potentials 4

128
Table 123-9. Perinatal Risk Factors in Cerebral Palsy
UMN (No. of Patients) LMN (No. of Patients) Prematurity 10 1 Respiratory distress/arrest/apnea 9 2 Neonatal seizures 5 - Infection Traumatic birth Congenital hydrocephalus 3 Placenta previa/abruption Hypoglycemia ± seizures Intracranial hemorrhage Cyanosis at birth No specific factor noted 15
 LMN (No. of Patients) Prematurity Respiratory distress/arrest/apnea Neonatal seizures Infection. Traumatic birth. Congenital hydrocephalus. 3. Placenta previa/abruption. Hypoglycemia ± seizures. Intracranial hemorrhage. Cyanosis at birth. No specific factor noted. 15.")
129
Recommendations Overactive bladder treated with anticholinergic
+/- CIC Dorsal rhizotomy in selected group of children who fail to respond to less invasive measures

130
Traumatic injuries to the spine
Rarely encountered in children Pts with upper thoracic or cervical lesion are likely to have autonomic dysreflexia with spontaneous discharge of alpha1 stimulants during bladder filling & with contraction of detrusor Monitoring of BP & availability of alpha blockers are mandatory during VCUG or CMG

131
Management If retention immediately after trauma, foley catheter is inserted and kept in place as short time as possible Until the pt is stable and aseptic CIC can be started safely on regular basis The goal is balanced voiding at pressures < 40 cmH2O, which reduces the 30% risk of urinary tract deterioration seen in poorly managed pts If cannot be achieved, CIC is continued

132
Anticholinergic drugs (P. O
Anticholinergic drugs (P.O. or intavesically) added as they are effective in reducing overactive bladder Alternative Rx External urethral sphincterotomy Urethral stent placement Injection of botulinum A toxin (Botox) into the external sphincter Continent catheterizable abdominal urinary stoma in pts with low cervical or upper thoracic lesions who cannot easily catheterize themselves
 added as they are effective in reducing overactive bladder. Alternative Rx. External urethral sphincterotomy. Urethral stent placement. Injection of botulinum A toxin (Botox) into the external sphincter. Continent catheterizable abdominal urinary stoma in pts with low cervical or upper thoracic lesions who cannot easily catheterize themselves.")
Similar presentations



















,MRCGP,MRCPE.>")

