Download presentation
Presentation is loading. Please wait.

1
Fire-Based EMS The Next Generation
Fire Chief Harry Beck Mesa Fire and Medical Department Gary Smith, MD Medical Director, Mesa Fire and Medical Department

2
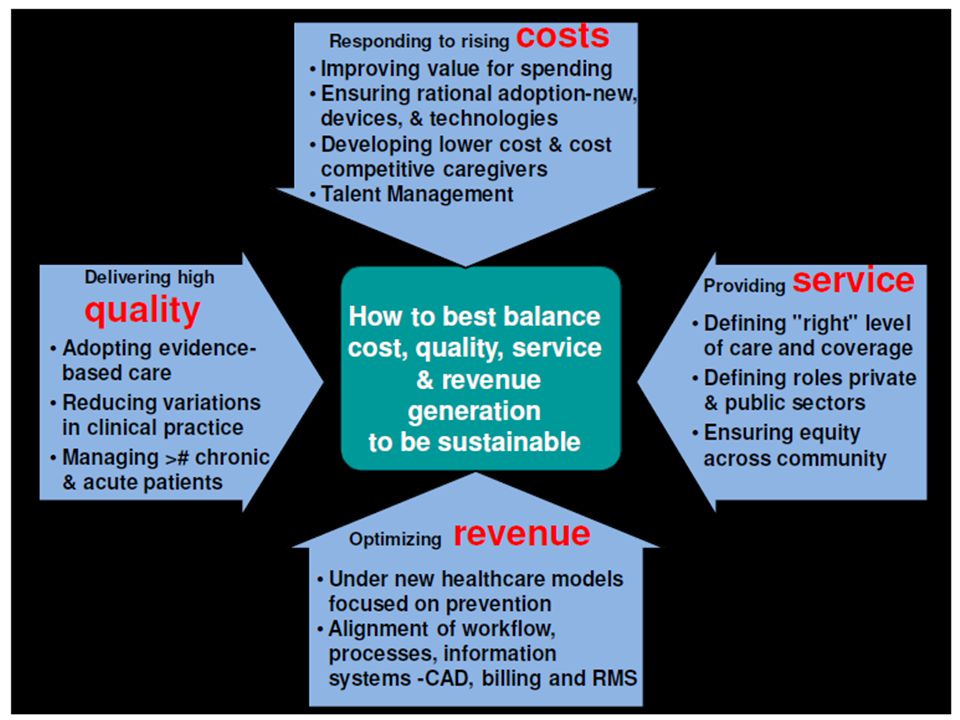
Purpose Describe a model of Fire-Based EMS for proven performance and efficiencies under the Affordable Care Act.

3
City of Mesa, Arizona 137 square miles 75,000+ > 62 years of age
440,000 residents (2010) 85,000 winter visitors (2010) 75,000+ > 62 years of age Diverse Population
 85,000 winter visitors (2010) 75,000+ > 62 years of age. Diverse Population.")
4
Mesa Fire and Medical Department
21 ALS Engines 5 ALS Ladders Community Paramedics Private Ambulance 2 Community Care Units 20 Fire Stations 55,938 Total Calls 80 % Fire Based EMS

5
Mesa Fire and Medical Dispatch Analysis 2013
Mesa 911 Calls 55,938 Medical Emergency Calls 45,854 Low Acuity Calls 10,061

6
Community Care Initiative

7
Low Emergency Response Model Features
Improves Availability for Response to High Emergencies Improves Availability of Ambulances and ERs 911 Based Operated from Fire and Medical Response Model Integrates Partnerships

8
Low Emergency Response Model Features
Allows Partner Billing No City Billing at This Time No change in PM Scope of Practice Tiered Triage and Deployment Alternate Destination/Admission Avoidance PCP Referral

9
Community Paramedic Unit (TRV)
Captain Paramedic & Firefighter Two Response Units Low Acuity Patients Peak Time Deployment Priority Dispatch Triage Treat and Refer

10
Community Care Nurse Practitioner Unit
Captain Paramedic & Nurse Practitioner Nurse Practitioner Provided by Mountain Vista Hospital Treat and Refer to PCP CLIA Waived Laboratory Tests Provide Alternative Destination Patient Follow-up Peak Time Deployment Provide Support to Law Enforcement

11
Community Care Behavioral Health Unit
Captain Paramedic and Behavioral Health Specialist Dispatch to Definitive Care in 1-Hour 45-Minutes Alternate Destination Video

12
Proven Model Air Date: January 2013, KSAZ-TV

13
Emergency Room Costs 2013 Cost Comparison
Source: Kliff,S. An Average Emergency Department Visit Costs More Than an Average Month’s Rent. The Washington Post. 2 March 2013

14
Emergency Care Charges Low Acuity Medical Patients
Past Model New Model Savings Transport to ER $1,000 $0 $1,000 Registration $525 $0 $525 Physician Assessment $325 $150 $175 Decision Making $950 $0 $950 MFMD Cost $375 $375 $0 $2,650 Total Savings per Patient

15
Emergency Care Charges Behavioral Health Patients
Past Model New Model Savings Transport to ER $1,000 $0 $1,000 Initial Evaluation $3,500 $150 $3,350 3-Day ER Hold $6,000 $0 $6,000 Inter-Facility Transport $1,000 $0 $1,000 MFMD Cost $375 $375 $0 $11,350 Total Savings per Patient

16
Unit Insurance Coverage
2013 Community Care Response Behavioral Health Community Care Response Behavioral Health Medicare 28% 44% Medicaid 37% 36% Private 15% 19% None 20% 1%

17
Projected Cost vs. Benefit Detail

18
EMS Prevention Model Features
Reduces EMS Calls Supported by Call Center RN Tiered Triage Coordinates with Providers Integrates Partnerships

19
EMS Prevention Model Features
Incorporates City Billing Assists with Sustainability Provides Post-Hospital Services Provides “GAP” Services Reduces Hospital Admissions

20
Loyalty Customer Program
Proactive Service Reduction of EMS Calls Partnership with ACO

21
Transitional Care Program
72-Hour Post-Discharge Contact Partnership with Physician (PCP/Specialist) Proactive Service Reduces Readmissions Transition to Home Health Sustainable
 Proactive Service. Reduces Readmissions. Transition to Home Health. Sustainable.")
22
Hospice Comfort Pack Program
Coordinated with Hospice Provider Maintains Patient Qualification Improves/Maintains Care Eliminates Transport Sustainable

23
Crisis Prevention Outreach Programs
Target Populations Facilitates Access to Appropriate Service Facilitates Intervention Behavioral Health Partnership

24
Community Based EMS Programs
Direct Community Involvement Partnership with Good Samaritans Awareness/Education/Training MICR/CPR Training First Aid Training Hospital Partnerships Immunizations School Partnerships

25
What… When… Where… Why…

26
The Reason We Are Still Needed

27
…and Needed Less

28
The Fire Service is Getting More Expensive…

31
Mobile Integrated Healthcare Programs
Pilot programs focus on Patient Navigation 9-1-1 Nurse Triage “EMS Loyalty” Programs Readmission Avoidance Hospice Revocation Avoidance 23-hour Observation Avoidance Require Agility

32
Core Reform Strategies
Public Reporting: engaging consumers and other stakeholders Health Information Technology: enabling improvement Value-Based Payment: rewarding achievement Clinically Integrated Delivery Systems: achieving patient centered care

33
A Future System Affordable Accessible – to care and to information
Seamless and Coordinated High Quality – timely, equitable, safe Person and Family-Centered Supportive of Clinicians in serving their patients’ needs Engaged with the community and fulfilling its population’s unique needs

34
Developmental Needs Cost Recovery Shared Savings Pay-For-Performance
Capitation ACO Involvement Fire Station Based Clinics 72 hr. Patient Follow-Ups Research Evidenced-Based Quality Assurance

35
To view a copy of this presentation…
Find us: mesafiredept East Valley Wellness AZ

36
Mountain Vista Medical Center
Public-Private Partnership Mountain Vista Medical Center IASIS Healthcare (One of the largest healthcare organizations in the US) 176 Beds 15 Bed Emergency Department 55,000 ED visits a year Level 3 Trauma, Stroke Center, Cardiac Center
 176 Beds. 15 Bed Emergency Department. 55,000 ED visits a year. Level 3 Trauma, Stroke Center, Cardiac Center.")
37
Mesa Fire and Medical Model
Evolving Issues National Health Care Major Issue Cost of Health Care % GDP Impact of Affordable Care Act Resulting Changes to CMS Creation of Accountable Care Organizations CMS Grant Opportunity

38
Community Care Initiative: Aims and Drivers
Affordable Care Act Community Care Initiative: Aims and Drivers

39
Dispatch to Definitive Care
Behavioral Health Dispatch to Definitive Care in 1 hr 45 min Video

40
Citywide BLS Calls 2013

41
Behavioral Health/Substance Abuse
2013

42
Behavioral Health/Suicide Threat
2013

43
2012/13 Community Care Response Pilot
Community Care Response Unit 2012/13 Community Care Response Pilot 2012/13 CCR Responses 1,250 Directed to Appropriate Care (40%) 2012/13 Low Acuity Response Analysis (based on current dispatch protocols) Medicaid 3,723 Medicare 2,817 Private ,509 Uninsured 2,012 Directed to Appropriate Care (potential) 4,024
 2012/13 Low Acuity Response Analysis. (based on current dispatch protocols) Medicaid 3,723. Medicare 2,817. Private 1,509. Uninsured 2,012. Directed to Appropriate Care (potential) 4,024.")
44
Cost Average Per Patient Total $375 Human Resource Supplies/Equipment
Community Care Response Unit Cost Human Resource Captain Paramedic and Nurse Practitioner or Behavioral Specialist) $310 Supplies/Equipment $20 Response Apparatus $45 Average Per Patient Total $375
 $310. Supplies/Equipment. $20. Response Apparatus. $45. Average Per Patient Total. $375.")
45
Medicare 18% Medicaid 15% Private 8% None 1% No Information 59%
Behavioral Health Unit Insurance Coverage Including Patients with no Insurance Information 2013 Medicare 18% Medicaid 15% Private 8% None 1% No Information 59%

46
Behavioral Health Unit Insurance Coverage
2013 Medicare 44% Medicaid 36% Private 19% None 1%

47
Private 23% Medicare 3% Uninsured 29%
Billing Information for Behavioral Health Unit Information Provided by the Mental Health Provider 2013 Private % Medicare % Uninsured % Medicaid/Medicare/Magellan 45%

48
Community Care Response Unit
Expansion of the model Public-Private Partnerships Higher Education for Members Enhance public access Fire Station Based Clinics Determine demographics

49
The Next Generation Public School Partnerships Communication Center
Centralized Medical Direction On site medical direction Telemedicine Business/Special Events Integrate into health care systems

50
The Next Generation Post Surgical Checks Injury Prevention
Community Based EMS Behavioral Health Intervention Sustainability Healthcare Information Exchange

51
Primary Care Physician
Not to replace the Primary Care Physician

Similar presentations