Download presentation
Presentation is loading. Please wait.

1
By Dr.Aiman AL Solumany (R2) King Fahd General Hospital
Urinary stone disease By Dr.Aiman AL Solumany (R2) King Fahd General Hospital
 King Fahd General Hospital.")
2
In General Urinary calculi are the third most common problem of the urinary tract, exceeded only by urinary tract Infections and pathologic conditions of the prostate. 1-Renal calculi 2- medical evaluation

3
EPIDEMIOLOGY OF RENAL CALCULI
Incidence The lifetime prevalence of kidney stone disease is estimated at 1% to 15%, with the probability of having a stone varying according to age, gender, race, and geographic location Recurrence rate – with out ttt 10% at 1 yr, 50% at 10 yrs. Factors :. 1- intrinsic factor. 2- extrinsic factors

4
EPIDEMIOLOGY OF RENAL CALCULI
Intrinsic Factors genetics: FHx and race rare in Natives, blacks common in Asians and whites about 25% of patients with kidney stones have a family history of kidney stones. Age and Sex Peak years old M : F - 3:1 F > M - stones 2nd to infections or abN

5
EPIDEMIOLOGY OF RENAL CALCULI
Extrinsic Factors: 1. Geography The prevalence of urinary calculi is higher in those who live in mountainous, desert, or tropical areas. increased incidence: US, UK, Scandanavia, Mediterranean, northern India/Pakistan, northern Australia, central Europe, and China.

6
EPIDEMIOLOGY OF RENAL CALCULI
2-climate and seasonal factors : incidence highest in July, Aug, Sep: 1-2 months after maximal mean annual temperature dehydration, increased exposure to sunlight and increased vitamin D production w/ increased urinary Ca excretion. 3-water intake: decreases average time of residence of free crystal particles in urine and dilutes components.

7
EPIDEMIOLOGY OF RENAL CALCULI
4-Diet:. .high protein and Na ca stones .high purine pH hyperuricosuria .low Vit B12 formation and excretion of oxalate. The risk of stone disease correlates with weight and body mass index.

8
EPIDEMIOLOGY OF RENAL CALCULI
5-occupation: stones more likely to be found in pts w/ sedentary lifestyles professional and managerial groups, affluent countries/regions/societies 6-stress: lower family income, mortgage problems, emotional life events associated w/ stone disease

9
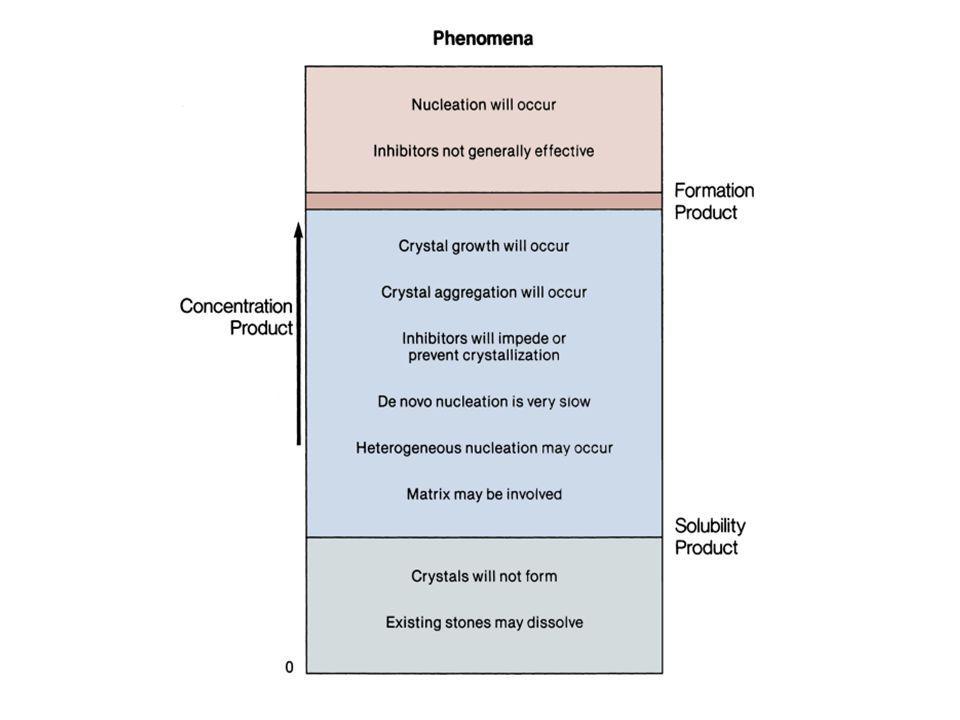
PHYSICOCHEMISTRY State of Saturation:
The physical process of stone formation is a complex cascade of events. It begins with urine that becomes supersaturated with respect to stone-forming salts, such that dissolved ions or molecules precipitate out of solution and form crystals or nuclei. Once formed, crystals may flow out with the urine or become retained in the kidney at anchoring sites that promote growth and aggregation, ultimately leading to stone formation.

10
PHYSICOCHEMISTRY A solution containing ions or molecules of a soluble salt is described by the concentration product, which is a mathematical expression of the product of the concentrations of the pure chemical components (ions or molecules) of the salt. A pure aqueous solution of a salt is considered saturated when it reaches the point at which no further added salt crystals will dissolve.
 of the salt. A pure aqueous solution of a salt is considered saturated when it reaches the point at which no further added salt crystals will dissolve.")
11
PHYSICOCHEMISTRY The concentration product at the point of saturation is called the thermodynamic solubility product, Ksp, Ksp, which is the point at which the dissolved and crystalline components are in equilibrium for a specific set of conditions. At this point, addition of further crystals to the saturated solution will cause the crystals to precipitate unless the conditions of the solution, such as pH or temperature, are changed.

12
PHYSICOCHEMISTRY In urine, despite concentration products of stone- forming salt components, such as calcium oxalate, that exceed the solubility product, crystallization does not necessarily occur because of the presence of inhibitors and other molecules . In this state of saturation, urine is considered to be metastable with respect to the salt.

13
PHYSICOCHEMISTRY As concentrations of the salt increase further, the point at which it can no longer be held in solution is reached and crystals form. this point is called the formation product, Kf. Ksp and Kf differentiate the three major states of saturation in urine: undersaturated, metastable, and unstable.

14
PHYSICOCHEMISTRY Below the solubility product, crystals will not form under any circumstances. above the formation product, the solution is unstable and crystals will form. In metastable range, in which the concentration products of most common stone components reside, spontaneous nucleation or precipitation does not occur despite urine that is supersaturated. in this area that modulation of factors controlling stone formation can take place and therapeutic intervention is directed.

16
PHYSICOCHEMISTRY Nucleation and Crystal Growth, Aggregation, and Retention: In normal urine, the concentration of calcium oxalate is four times higher than its solubility in water calcium oxalate precipitation in urine occurs only when its supersaturation is 7 to 11 times its solubility. Precip occurs due to the following factors :. 1-Low urinary volumes. 2-High rates of calcium, oxalate, phosphate, or urate excretion. 3- Low citrate and magnesium excretion .

17
PHYSICOCHEMISTRY Nuclei are the earliest crystal structure that will not dissolve. Homogenous nucleation - process of nuclei formation in pure solution Heterogenous nucleation - nuclei form on existing surfaces - eg epithelial cells, cell debris, urinary casts, crystals - Lower concentration needed Most of CaOx is heterogenous

18
PHYSICOCHEMISTRY Another concept necessary for understanding the genesis of urinary calculi is that of aggregation. Crystal nuclei cannot grow large enough to attach to and occlude renal tubular lumens within the 5 to 7 minutes that it takes for them to pass through tubules and enter the renal pelvis. They can, aggregate into large clumps within a minute

19
PHYSICOCHEMISTRY Inhibitors:.
Whole urine, when added to a solution of calcium phosphate, raises the supersaturation level required to initiate calcium phosphate crystallization. Citrate, Magnesium, and pyrophosphate together were account for 20% of the inhibitory activity of whole urine, with citrate comprising the most important factor of the three. no specific inhibitors are known that affect uric acid crystallization.

20
PHYSICOCHEMISTRY Citrate
acts as an inhibitor of calcium oxalate and calcium phosphate stone formation by a variety of actions: 1- it complexes with calcium, reducing the availability of ionic calcium to interact with oxalate or phosphate

21
PHYSICOCHEMISTRY 2- It directly inhibits the spontaneous precipitation of calcium oxalate and prevents the agglomeration of calcium oxalate crystals. it has limited inhibitory effect on calcium oxalate crystal growth , more potent activity in reducing calcium phosphate growth. 3- citrate prevents heterogeneous nucleation of calcium oxalate by monosodium urate .

22
PHYSICOCHEMISTRY Magnesium:. Its complexe with oxalate, which reduces ionic oxalate concentration and calcium oxalate supersaturation. In addition, magnesium reduces the rate of calcium oxalate crystal growth in vitro. Inorganic pyrophosphate:. responsible for 25% to 50% of the inhibitory activity of whole urine against calcium phosphate crystallization.

23
PHYSICOCHEMISTRY Two urinary glycoproteins, nephrocalcin and Tamm- Horsfall glycoprotein, are potent inhibitors of calcium oxalate monohydrate crystal aggregation . 1-Nephrocalcin is an acidic glycoprotein containing predominantly acidic amino acids that is synthesized in the proximal renal tubules and the thick ascending limb. In simple solution, nephrocalcin strongly inhibits the growth of calcium oxalate monohydrate crystals .

24
PHYSICOCHEMISTRY 2. Tamm-Horsfall glycoprotein: . syn - thick ascending limb & distal tubule . inhibits aggregation CaOx- most potent . Under specific condition, THP can promote aggregation (high ionic strength, high calcium and low pH) . Citrate can increase THP and its inhibitory effect
 . Citrate can increase THP and its inhibitory effect")
25
PHYSICOCHEMISTRY 3. Osteopontin (uropontin):
Osteopontin has been shown to inhibit nucleation, growth, and aggregation of calcium oxalate crystals as well as to reduce binding of crystals to renal epithelial cells in vitro

26
PHYSICOCHEMISTRY Matrix: Renal calculi consist of both crystalline and noncrystalline components. The noncrystalline component is termed matrix, which typically accounts for about 2.5% of the weight of the stone In some cases reached up to 65%.

27
PHYSICOCHEMISTRY chemical analysis reveals a heterogeneous mixture consisting of 65% protein, 9% non-amino sugars, 5% glucosamine, 10% bound water, and 12% organic ash . Non–urease-producing bacteria such as E. coli may play a role in stone formation by increasing the production of urinary matrix substances, thereby increasing crystal adherence to the renal epithelium.

28
MINERAL METABOLISM Calcium:.
30% to 40 % of dietary calcium is absorbed from small intestine (the jejunum and the proximal portion of the ileum) and only approximately 10% absorbed in the colon. absorption of calcium varies with calcium intake. with low calcium intake, calcium absorption is enhanced; during high calcium intake absorption is reduced.
 and only approximately 10% absorbed in the colon. absorption of calcium varies with calcium intake. with low calcium intake, calcium absorption is enhanced; during high calcium intake absorption is reduced.")
29
MINERAL METABOLISM (Calcium)
Calcium in Plasma in three form : 1) combined with plasma proteins (40%) 2) combined with other substances but diffusible through capillaries (10%) 3) Ca++ (50%) active
 combined with plasma proteins (40%) 2) combined with other substances but diffusible through capillaries (10%) 3) Ca++ (50%) active.")
30
MINERAL METABOLISM (Calcium)
the net absorption of calcium 100 to 300 mg/Day. Calcium is absorbed in the ionic state; therefore, substances that complex calcium, such as phosphate, citrate, sulfate, oxalate, and fatty acids, reduce the availability of ionic calcium for absorption. The most important factor that mediates active or transcellular calcium absorption is 1,25- dihydroxyvitamin D3, or calcitriol.

31
MINERAL METABOLISM (Calcium)
The active form of vitamin D, 1,25(OH)2D3, is the most potent stimulator of intestinal calcium absorption. After conversion of 7-dehydrocholesterol in the skin to previtamin D3 promoted by sunlight, previtamin D3 is hydroxylated in the liver to 25- hydroxyvitamin D3, which is further hydroxylated in the proximal renal tubule to 1,25(OH)2D3. The conversion of 25-hydroxyvitamin D3 to 1,25(OH)2D3 is stimulated by parathyroid hormone (PTH) and by hypophosphatemia.
2D3, is the most potent stimulator of intestinal calcium absorption. After conversion of 7-dehydrocholesterol in the skin to previtamin D3 promoted by sunlight, previtamin D3 is hydroxylated in the liver to 25- hydroxyvitamin D3, which is further hydroxylated in the proximal renal tubule to 1,25(OH)2D3. The conversion of 25-hydroxyvitamin D3 to 1,25(OH)2D3 is stimulated by parathyroid hormone (PTH) and by hypophosphatemia.")
32
MINERAL METABOLISM (Calcium)
A decrease in serum calcium increases secretion of PTH, which in turn directly stimulates the enzyme 1α- hydroxylase, which is located in the mitochondria of the proximal renal tubule. After transport via the bloodstream to the intestine, 1,25(OH)2D3, binds to the vitamin D receptor in the brush border membrane epithelial cells to enhance calcium absorption.
2D3, binds to the vitamin D receptor in the brush border membrane epithelial cells to enhance calcium absorption.")
33
MINERAL METABOLISM (Calcium)
Calcitriol also acts on the bone and kidney in addition to its action in increasing calcium absorption from the intestine. PTH increases renal calcium reabsorption and enhances phosphate excretion, leading to a net increase in serum calcium, which ultimately suppresses further PTH secretion and synthesis of 1,25(OH)2D3. Only mature PTH is secreted from the parathyroid gland, and the most potent stimulus for its secretion is a decrease in serum calcium.
2D3. Only mature PTH is secreted from the parathyroid gland, and the most potent stimulus for its secretion is a decrease in serum calcium.")
34
MINERAL METABOLISM (phosphorus)
Phosphorus: is transported across the intestine through active and passive mechanisms. Approximately 60% of the phosphate in the diet is absorbed by the intestine. 1,25-Dihydroxyvitamin D3 stimulates phosphorus absorption in the duodenum and jejunum through a sodium-dependent active transport process . The transport of phosphate is pH dependent: A decrease in luminal pH inhibits phosphate transport, and an increase in pH stimulates phosphate transport.

35
MINERAL METABOLISM (phosphorus)
phosphorus is secreted by the ileum and colon. About 65% of the absorbed phosphate is excreted by the kidney and the remainder by the intestine. Under normal conditions, approximately 20% of the filtered load is excreted, the other 80% being absorbed by the proximal tubule.

36
MINERAL METABOLISM (phosphorus)
PTH is the major hormonal regulator of renal phosphate reabsorption. Daily, about 150 to 200 mmol of calcium and about 100 mmol of phosphorus are filtered: Only 5 mmol of calcium and 10 mmol of phosphorus are excreted in the urine. So, 97% to 99% of calcium and 85% to 90% of phosphorus are reabsorbed by the kidney.

37
MINERAL METABOLISM (Magnesium)
Magnesium is also absorbed via active and passive mechanisms by the intestine. About 35% to 40% of ingested magnesium is absorbed. Although magnesium is absorbed mostly in the small intestine, some is absorbed by the large bowel also. Both vitamin D and PTH increase magnesium absorption.

38
MINERAL METABOLISM (Oxalate)
Oxalic acid is present in many foods and beverages. poorly absorbed in N pts, with Ca in diet. Oxalate absorption is markedly increased in patients with small bowel resection and an intact colon or inflammatory bowel disease . stomach and distal bowel may be the primary sites for oxalate absorption.

39
MINERAL METABOLISM (Oxalate)
Oxalobacter formigenes, utilize oxalate as an energy source and consequently reduce intestinal oxalate absorption. Recent studies have demonstrated that stone formers have reduced levels or absent colonization with Oxalobacter compared with non—stone-forming. those individuals lacking the bacteria have higher urinary oxalate levels.

40
MINERAL METABOLISM (Oxalate)
Intestinal oxalate absorption is influenced by luminal calcium, magnesium, and oxalate- degrading bacteria. Eighty percent of the oxalate found in urine comes from endogenous production in the liver (40% from ascorbic acid, 40% from glycine), and 10% comes from dietary sources.
, and 10% comes from dietary sources.")
41
Pathopysiology of Stone Formation

42
Calcium-Containing Stones Calcium oxalate 60 Hydroxyapatite 20
Stone Composition Occurrence (%) Calcium-Containing Stones Calcium oxalate 60 Hydroxyapatite 20 Brushite 2 Non–Calcium-Containing Stones Uric acid 7 Struvite Cystine 1-3 Triamterene >1 Silica 2,8-Dihyroxyadenine Stone Composition and Relative Occurrence
 Calcium-Containing Stones. Calcium oxalate. 60. Hydroxyapatite. 20. Brushite. 2. Non–Calcium-Containing Stones. Uric acid. 7. Struvite. Cystine Triamterene. >1. Silica. 2,8-Dihyroxyadenine. Stone Composition and Relative Occurrence.")
43
Pathopysiology of Stone Formation (calcium stone )
Hypercalciuria is the most common abnormality identified in calcium stone formers. Between 35% and 65% of all patients with calcium oxalate kidney stones have increased urinary calcium excretion in the absence of raised serum calcium levels. Pak (1987), who defined it as the excretion of greater than 200 mg of calcium per 24 hours after 1 week's adherence to a 400-mg calcium, 100-mEq sodium diet.
, who defined it as the excretion of greater than 200 mg of calcium per 24 hours after 1 week s adherence to a 400-mg calcium, 100-mEq sodium diet.")
44
Pathopysiology of Stone Formation (calcium stone )
Parks and Coe (1986) defined hypercalciuria as excretion of calcium of greater than 4 mg/kg/day or greater than 7 mmol/day (men) or 6 mmol/day (women). Calcium transport is regulated at three sites: intestine, bone, and kidney. Dysregulation at any of these sites can lead to hypercalciuria.
 defined hypercalciuria as excretion of calcium of greater than 4 mg/kg/day or greater than 7 mmol/day (men) or 6 mmol/day (women). Calcium transport is regulated at three sites: intestine, bone, and kidney. Dysregulation at any of these sites can lead to hypercalciuria.")
45
Pathopysiology of Stone Formation (calcium stone )
hypercalciuria divided into three subtypes: 1- Absorptive hypercalciuria due to increased intestinal absorption of calcium. 2- Renal hypercalciuria due to primary renal leak of calcium. 3- Resorptive hypercalciuria due to increased bone demineralization.

46
Pathopysiology of Stone Formation (calcium stone )
Absorptive hypercalciuria:. AH is increased intestinal absorption of calcium, which occurs in approximately 55% of stone formers ( Menon, 1986 ). AH is classified as :. type I when urinary calcium remains high despite a low calcium diet (400 mg dietary calcium daily). type II when urinary calcium normalizes with a restricted calcium intake.
. AH is classified as :. type I when urinary calcium remains high despite a low calcium diet (400 mg dietary calcium daily). type II when urinary calcium normalizes with a restricted calcium intake.")
47
Pathopysiology of Stone Formation (calcium stone )
1,25-dihydroxyvitamin D3levels are elevated in up to 50% of patients with absorptive hypercalciuria, suggesting that, at least in some individuals, this condition is secondary to increased production of or increased sensitivity to vitamin D metabolites. Another etiology of AH is renal phosphate wasting leading to a subsequent increase in active vitamin D.

48
Pathopysiology of Stone Formation (calcium stone )
Mechanisms of absorptive hypercalciuria :

49
Pathopysiology of Stone Formation (calcium stone )
Renal hypercalciuria:. The kidney filters approximately 270 mmol of calcium and must reabsorb more than 98% of it to maintain calcium homeostasis. Approximately 70% of calcium reabsorption occurs in the proximal tubule. In renal hypercalciuria, impaired renal tubular reabsorption of calcium results in elevated urinary calcium levels leading to secondary hyperparathyroidism.

50
Pathopysiology of Stone Formation (calcium stone )
the underlying abnormality is primary renal wasting of calcium. The consequent reduction in circulating serum calcium stimulates PTH production

51
Pathopysiology of Stone Formation (calcium stone )
High fasting urinary calcium levels with a normal serum calcium value are characteristic of renal hypercalciuria. The elevated fasting urinary calcium and serum PTH levels differentiate renal from absorptive hypercalciuria.

52
Pathopysiology of Stone Formation (calcium stone )
Resorptive hypercalciuria:. is an infrequent abnormality most commonly associated with primary hyperparathyroidism. Primary hyperparathyroidism is the cause of nephrolithiasis in about 5% of cases .

53
Pathopysiology of Stone Formation (calcium stone )
Excessive PTH secretion from a parathyroid adenoma leads to excessive bone resorption and increased renal synthesis of 1,25(OH)2D3. which in turn enhances intestinal absorption of calcium. the net effect is elevated serum and urine calcium levels and reduced serum phosphorus levels.
2D3. which in turn enhances intestinal absorption of calcium. the net effect is elevated serum and urine calcium levels and reduced serum phosphorus levels.")
54
Idiopathic hypercalciuria occurs in 5% to 10% of healthy people and in about half of patients with calcium nephrolithiasis.

55
Calcium Load Test. After 7 days of a low-calcium, low-sodium diet, patients fast for 12 hours from 9 PM. Distilled water is provided at 9 PM and midnight. At 7 AM the next day, patients completely empty the bladder and discard the urine. They drink an additional 600 mL of distilled water. Urine is collected from 7 to 9 AM. This is the fasting sample.

56
At 9 AM, 1 g of calcium mixed in a liquid synthetic meal is given orally.
Urine is collected from 9 AM to 1 PM. This is the postload sample. Both urine samples are analyzed for calcium, creatinine, and cAMP . cAMP measurements are used as an indirect estimate of parathyroid function because most PTH assays are insensitive to rapid changes in serum calcium.

58
Pathopysiology of Stone Formation (calcium stone )
Additional, rare causes of resorptive hypercalciuria include hypercalcemia of malignancy, sarcoidosis, thyrotoxicosis, and vitamin D toxicity. Many granulomatous diseases including tuberculosis, sarcoidosis, histoplasmosis, leprosy, and silicosis have been reported to produce hypercalcemia. Sarcoidosis is most commonly associated with urolithiasis.

59
Pathopysiology of Stone Formation (calcium stone )
The sarcoid granuloma produces 1,25(OH)2D3, causing increased intestinal absorption of calcium, hypercalcemia, and hypercalciuria. primary hyperparathyroidism is the most common cause of hypercalcemia in an outpatient setting, malignancy is the main cause of hypercalcemia in hospitalized patients. Lung and breast cancers account for about 60% of malignancy-associated hypercalcemia, whereas renal cell (10% to 15%), head and neck (10%).
2D3, causing increased intestinal absorption of calcium, hypercalcemia, and hypercalciuria. primary hyperparathyroidism is the most common cause of hypercalcemia in an outpatient setting, malignancy is the main cause of hypercalcemia in hospitalized patients. Lung and breast cancers account for about 60% of malignancy-associated hypercalcemia, whereas renal cell (10% to 15%), head and neck (10%).")
60
Pathopysiology of Stone Formation (calcium stone )
Primary Hyperparathyroidism the prevalence of stone disease in hyperparathyroidism is only about 1%. The diagnosis is difficult ,it requires a demonstration of hypercalcemia in the absence of any other disorder that elevates serum calcium .

61
Pathopysiology of Stone Formation (calcium stone )
Glucocorticoid-Induced Hypercalcemia: Glucocorticoids can alter calcium metabolism through their actions on bone, intestine, and parathyroid glands. Their most potent effect is related to calcium metabolism in bones, where glucocorticoids promote bone resorption and reduce bone formation, leading to osteopenia with chronic use. stimulate release of PTH . inhibit intestinal absorption of calcium . common in patients with Cushing's syndrome.

62
Pathopysiology of Stone Formation (calcium stone )
Hyperoxaluria, defined as urinary oxalate greater than 40 mg/day, leads to increased urinary saturation of calcium oxalate and subsequent promotion of calcium oxalate stones. oxalate has been implicated in crystal growth and retention by means of renal tubular cell injury mediated by lipid peroxidation and the generation of oxygen free radicals .

63
Pathopysiology of Stone Formation (calcium stone )
Causes of hyperoxaluria :. Disorders in biosynthetic pathways (primary hyperoxaluria). Intestinal malabsorptive states associated with inflammatory bowel disease, celiac sprue, or intestinal resection (enteric hyperoxaluria). Excessive dietary intake or high substrate levels (vitamin C) (dietary hyperoxaluria).
. Intestinal malabsorptive states associated with inflammatory bowel disease, celiac sprue, or intestinal resection (enteric hyperoxaluria). Excessive dietary intake or high substrate levels (vitamin C) (dietary hyperoxaluria).")
64
Pathopysiology of Stone Formation (calcium stone )
Primary hyperoxaluria is the result of a rare autosomal recessive disorder in glyoxylate metabolism by which the normal conversion of glyoxylate to glycine alanine glyoxylate aminotransferase (AGT), is prevented, leading to oxidative conversion of glyoxylate to oxalate, an end product of metabolism . mutation of the AGT gene (AGXT) results in a substitution of glycine by arginine at position 170.
, is prevented, leading to oxidative conversion of glyoxylate to oxalate, an end product of metabolism . mutation of the AGT gene (AGXT) results in a substitution of glycine by arginine at position 170.")
65
Pathopysiology of Stone Formation (calcium stone )
markedly high levels of urinary oxalate(>100 mg/day), leading to increased saturation of calcium oxalate, aggressive stone formation, and marked nephrocalcinosis untreated, primary hyperoxaluria leads to end-stage renal failure, which occurs by age 15 in 50% of affected patients and is associated with an overall death rate of approximately 30% Primary hyperoxaluria is treated with pyridoxine supplements (200 to 400 mg/day), which lower oxalate production in some patients.
, leading to increased saturation of calcium oxalate, aggressive stone formation, and marked nephrocalcinosis. untreated, primary hyperoxaluria leads to end-stage renal failure, which occurs by age 15 in 50% of affected patients and is associated with an overall death rate of approximately 30% Primary hyperoxaluria is treated with pyridoxine supplements (200 to 400 mg/day), which lower oxalate production in some patients.")
66
Pathopysiology of Stone Formation (calcium stone )
Enteric Hyperoxaluria:. The most common cause of acquired hyperoxaluria is enteric hyperoxaluria. Malabsorption from any cause, including small bowel resection intrinsic disease, or jejunoileal bypass increases the colonic permeability of oxalate as the result of exposure of the colonic epithelium to bile salts. Furthermore, loss of calcium in the feces results in the presence of less calcium in the intestinal lumen, allowing oxalate to exist in a soluble form.

67
Pathopysiology of Stone Formation (calcium stone )
Treatment:. oral hydration and a low-oxalate, low-fat diet. Calcium carbonate by mouth, 1 to 4 g with each meal, binds oxalate in the gut so that it cannot be absorbed Cholestyramine, a nonabsorbable resin that binds fatty acids, bile salts, and oxalate, can be used at doses of 1 to 4 g with each meal and at bedtime.

68
Pathopysiology of Stone Formation (calcium stone )
Dietary Hyperoxaluria. In oxalate-rich foods such as nuts, chocolate, brewed tea, spinach, broccoli and strawberries can result in hyperoxaluria in normal patients. Increased animal protein can also increase urinary levels of calcium and oxalate . Severe calcium restriction may result in reduced intestinal binding of oxalate and increased intestinal oxalate absorption. Ascorbic acid supplementation has been shown to increase urinary oxalate levels by in vivo conversion to oxalate.

69
Pathopysiology of Stone Formation (calcium stone )
Idiopathic Hyperoxaluria :. Several studies have suggested that mild hyperoxaluria is as important a factor as hypercalciuria in the pathogenesis of idiopathic calcium oxalate stones . Baggio and associates (1986) detected a higher rate of oxalate flux across the red blood cell membrane at steady state in 114 patients with a history of calcium oxalate kidney stones compared with control subjects.
 detected a higher rate of oxalate flux across the red blood cell membrane at steady state in 114 patients with a history of calcium oxalate kidney stones compared with control subjects.")
70
Pathopysiology of Stone Formation (calcium stone )
The treatment of mild hyperoxaluria is difficult. Dietary restriction of oxalate results in decreased oxalate excretion, but the decrease may not be significant Dietary calcium restriction is counterproductive because urinary oxalate excretion rises. Pyridoxine decreases urinary oxalate excretion in 50% of patients with mild metabolic hyperoxaluria. Administration of thiazides causes a decrease in urinary oxalate excretion and normalizes erythrocyte oxalate fluxes

71
Pathopysiology of Stone Formation (calcium stone )
Hyperuricosuria:. is defined by urinary uric acid exceeding 600 mg/day. Up to 10% of calcium stone formers have high urinary uric acid levels as the only abnormality . Hyperuricosuria increases urinary levels of monosodium urate, which in turn promotes calcium oxalate stone formation. At pH greater than 5.5, sodium urate formation promotes calcium oxalate stone formation through heterologous nucleation .

72
Pathopysiology of Stone Formation (calcium stone )
Uric acid may reduce the effectiveness of naturally occurring inhibitors of crystallization. uric acid crystals can bind urinary glycosaminoglycans such as heparin that inhibit crystallization of calcium oxalate. Excessive dietary purine intake is the main cause of hyperuricosuria . Between 80% and 90% of patients with hyperuricosuric nephrolithiasis are men.

73
Pathopysiology of Stone Formation (calcium stone )
Management of Hyperuricosuric Calcium Nephrolithiasis:. Dietary purine restriction, should prevent hyperuricosuria and nephrolithiasis. This requires limiting consumption of red meat, poultry, and fish Allopurinol inactivates xanthine oxidase and decreases uric acid synthesis

74
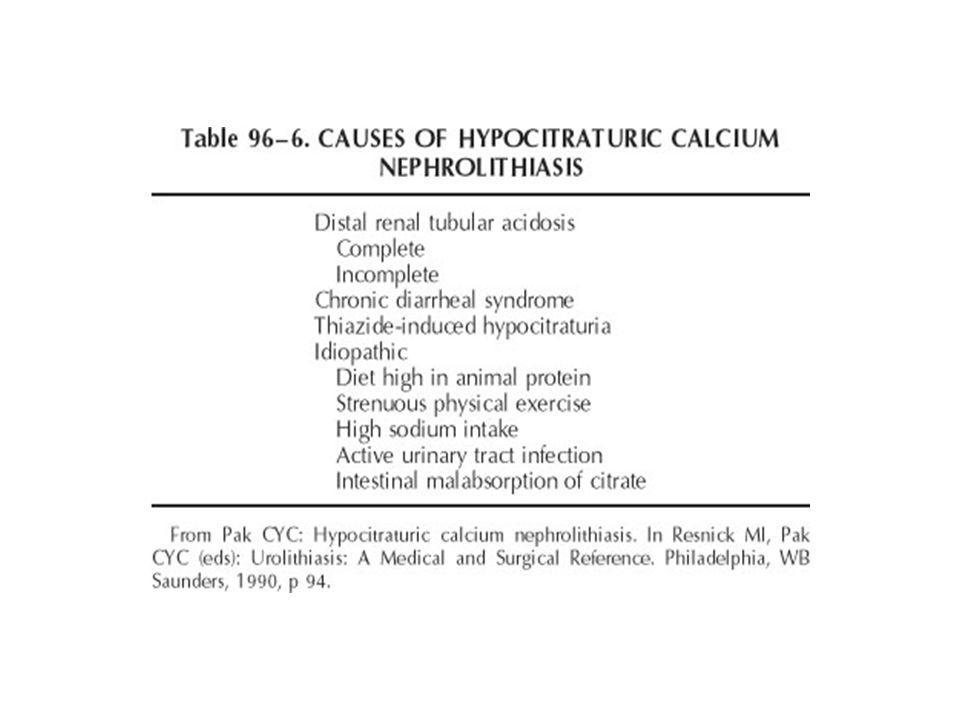
Pathopysiology of Stone Formation (calcium stone )
Hypocitraturia:. is defined as a urinary citrate level less than 320 mg/day ( Pak, 1987 ) or less than 0.6 mmol (men) or 1.03 mmol (women) daily is an important and correctable abnormality associated with nephrolithiasis that exists as an isolated abnormality in up to 10% of calcium stone formers and is associated with other abnormalities in 20% to 60% Citrate is an important inhibitor that can reduce calcium stone formation by several mechanisms. First, reduces urinary saturation of calcium salts by complexing with calcium
 or less than 0.6 mmol (men) or 1.03 mmol (women) daily. is an important and correctable abnormality associated with nephrolithiasis that exists as an isolated abnormality in up to 10% of calcium stone formers and is associated with other abnormalities in 20% to 60% Citrate is an important inhibitor that can reduce calcium stone formation by several mechanisms. First, reduces urinary saturation of calcium salts by complexing with calcium.")
75
Pathopysiology of Stone Formation (calcium stone )
Second, prevents spontaneous nucleation of calcium oxalate. Third, citrate inhibits agglomeration and sedimentation of calcium oxalate crystals as well as the growth of calcium oxalate and calcium phosphate crystals. Finally, normal urinary citrate levels can enhance the inhibitory effect of Tamm-Horsfall glycoprotein Metabolic acidosis reduces urinary citrate levels secondary to enhanced renal tubular reabsorption and decreased synthesis of citrate in peritubular cells

77
Pathopysiology of Stone Formation (calcium stone )
Renal Tubular Acidosis (RTA) :. Is a clinical syndrome that results from specific defects in renal tubular H+ secretion and urinary acidification. There are three types of RTA: 1, 2, and 4 Type 1 (distal) RTA is of particular significance to urologists not only because it is the most common form of RTA but also because it is the form of RTA most frequently associated with stone formation, which occurs in up to 70% of affected individuals.
 :. Is a clinical syndrome that results from specific defects in renal tubular H+ secretion and urinary acidification. There are three types of RTA: 1, 2, and 4. Type 1 (distal) RTA is of particular significance to urologists not only because it is the most common form of RTA but also because it is the form of RTA most frequently associated with stone formation, which occurs in up to 70% of affected individuals.")
78
Pathopysiology of Stone Formation (calcium stone )
the kidney must reabsorb or regenerate nearly all of the filtered bicarbonate each day (approximately 4500 mmol) to maintain its buffering capacity. the kidney must excrete excess acid, which accumulates from the breakdown of carbohydrates, fats, and proteins and as a result of bicarbonate loss in the stool . A defect in either bicarbonate reabsorption or acid excretion will lead to metabolic acidosis.
 to maintain its buffering capacity. the kidney must excrete excess acid, which accumulates from the breakdown of carbohydrates, fats, and proteins and as a result of bicarbonate loss in the stool . A defect in either bicarbonate reabsorption or acid excretion will lead to metabolic acidosis.")
79
Pathopysiology of Stone Formation (calcium stone )
Type 1 (Distal) Renal Tubular Acidosis :. Distal RTA is characterized by hypokalemic, hyperchloremic, non–anion gap metabolic acidosis and a urinary pH consistently above 6. The primary abnormality is the inability of the distal nephron to establish and maintain a proton gradient between tubular fluid and blood. Profound hypocitraturia, perhaps the most important factor in stone formation, is due to impaired citrate excretion as a result of metabolic acidosis
 Renal Tubular Acidosis :. Distal RTA is characterized by hypokalemic, hyperchloremic, non–anion gap metabolic acidosis and a urinary pH consistently above 6. The primary abnormality is the inability of the distal nephron to establish and maintain a proton gradient between tubular fluid and blood. Profound hypocitraturia, perhaps the most important factor in stone formation, is due to impaired citrate excretion as a result of metabolic acidosis.")
81
Pathopysiology of Stone Formation (calcium stone )
four major pathogenic mechanisms have been identified: a permeability defect. a proton pump secretory defect. a voltage-dependent defect. a carbonic anhydrase deficiency.

82
Pathopysiology of Stone Formation (calcium stone )
More than two thirds of patients with distal RTA are adults; the rest are children, mostly infants. Infants generally present with vomiting or diarrhea, failure to thrive, and growth retardation. Children present with metabolic bone disease and renal stones. Adults present with symptoms attributable to nephrolithiasis and nephrocalcinosis.

83
Pathopysiology of Stone Formation (calcium stone )
Up to 70% of adults with distal RTA have kidney stones. up to 80% of the patients are women. The most common type of stone associated with distal RTA is calcium phosphate as a result of hypercalciuria, hypocitraturia, and increased urinary pH.

85
Pathopysiology of Stone Formation (calcium stone )
Type 2 (Proximal) Renal Tubular Acidosis:. The primary defect here is a failure of bicarbonate resorption in the proximal tubule leading to urinary bicarbonate excretion. The defect in proximal tubular bicarbonate absorption results in increased urinary citrate excretion. Thus, most individuals believe that nephrolithiasis and nephrocalcinosis do not occur in patients with classic proximal RTA.
 Renal Tubular Acidosis:. The primary defect here is a failure of bicarbonate resorption in the proximal tubule leading to urinary bicarbonate excretion. The defect in proximal tubular bicarbonate absorption results in increased urinary citrate excretion. Thus, most individuals believe that nephrolithiasis and nephrocalcinosis do not occur in patients with classic proximal RTA.")
86
Pathopysiology of Stone Formation (calcium stone )
Type 4 RTA is associated with chronic renal damage, usually seen in patients with interstitial renal disease and diabetic nephropathy. Chronic renal parenchymal damage results in moderate reductions in glomerular filtration rate, hyperkalemia, and hyperchloremic metabolic acidosis with reduced net acid excretion . Nephrolithiasis and nephrocalcinosis are uncommon. patients with type 4 RTA do not make uric acid stones because their uric acid excretion is low, and they do not make calcium stones because their calcium excretion is low.

87
Pathopysiology of Stone Formation (calcium stone )
Diagnosis of Type 1 RTA:. The patient has hypokalemia, hyperchloremia, metabolic acidosis, and a urine pH of 5.5 or higher. Urinary citrate is low, usually less than 50 mg per 24 hours. Hypercalciuria is seen often.

88
Pathopysiology of Stone Formation (calcium stone )
")
89
Pathopysiology of Stone Formation (calcium stone )
therapy of RTA :. Alkali therapy decreases stone growth and new stone formation, delays the development of nephrocalcinosis, normalizes retarded growth in children, corrects the metabolic changes of hypokalemia

90
Pathopysiology of Stone Formation (calcium stone )
Potassium bicarbonate or citrate (1 to 2 mmol/kg daily in two to three divided doses) corrects systemic acidosis and normalizes urinary citrate. The goal of treatment is to restore urinary citrate to high normal levels and not simply to correct metabolic acidosis. If hypercalciuria persists with alkali therapy, a thiazide diuretic is added to the therapeutic regimen.
 corrects systemic acidosis and normalizes urinary citrate. The goal of treatment is to restore urinary citrate to high normal levels and not simply to correct metabolic acidosis. If hypercalciuria persists with alkali therapy, a thiazide diuretic is added to the therapeutic regimen.")
91
Pathopysiology of Stone Formation (calcium stone )
Hypomagnesuria:. is a rare cause of nephrolithiasis, affecting less than 1% of stone formers as an isolated abnormality, with other abnormalities in 6% to 11%. Magnesium complexes with oxalate and calcium salts, and therefore such low magnesium levels result in reduced inhibitory activity. Low urinary magnesium is also associated with decreased urinary citrate levels, which may further contribute to stone formation).
.")
92
Pathopysiology of Stone Formation (calcium stone )
Whether low magnesium is the cause or an effect of low citrate is not clear. Low magnesium levels occur with poor dietary intake or as a result of reduced intestinal absorption associated with intestinal abnormalities producing chronic diarrheal syndrome. magnesium citrate may be the ideal agent for the treatment of hypomagnesuric calcium nephrolithiasis

93
Pathopysiology of Stone Formation (uric acid stone)
two forms: free uric acid and urate salt, which forms a complex mostly with sodium. Sodium urate is approximately 20 times more soluble in water than free uric acid and does not crystallize under normal conditions.

94
Pathopysiology of Stone Formation (uric acid stone)
Predominantly affects middle-aged men 5 - 8% of stones are pure uric acid stone (they are often orange, small round and smooth) or % of uric acid stones are mixed with calcium. The stones are usually radiolucent but can be opaque if mixed with calcium or if they are very large (staghom) they can be faintly radiopaque even if pure uric acid.
 or % of uric acid stones are mixed with calcium. The stones are usually radiolucent but can be opaque if mixed with calcium or if they are very large (staghom) they can be faintly radiopaque even if pure uric acid.")
95
Pathopysiology of Stone Formation (uric acid stone)
Uric acid is the major metabolic end product of purine metabolism in men. The three main factors of uric acid stone formation are low pH, low urine volume, and hyperuricosuria . The most important pathogenetic factor is low urine pH, because most patients with uric acid stones have normal uric acid excretion but invariably demonstrate persistent low urine pH

96
Pathopysiology of Stone Formation (uric acid stone)
three factors are involved in uric acid urolithiasis:. First, patients tend to excrete excessively acidic urine at a relatively fixed, low urinary pH. Second, they may absorb, produce, or excrete more uric acid than patients without gout or uric acid stones. Third, urinary volume is diminished in these patients. The combination of these factors is ideal for the crystallization of uric acid in the urine.

97
Pathopysiology of Stone Formation (uric acid stone)
The principal cause of uric acid crystallization is the supersaturation of urine with respect to undissociated uric acid . There is no known inhibitor of uric acid crystallization. Dissociation proportional to pH

98
Pathopysiology of Stone Formation (uric acid stone)
Pts with uric acid stones have prolonged periods of acidity in urine. Almost 100% of the UA is dissociated at pH of 6.5 Patients with gout excrete relatively less ammonium and more titratable acid than do normal subjects Patients with gout or uric acid stones exhibit two other metabolic defects—overproduction of uric acid and impaired renal uric acid excretion. The exact cause of uric acid overproduction in primary gout is unknown

99
Pathopysiology of Stone Formation (uric acid stone)
The frequency of uric acid stones in gout is about 20%. Myeloproliferative disorders such as acute leukemia are an important cause of severe hyperuricosuria, particularly in childhood.

100
Pathopysiology of Stone Formation (uric acid stone)
")
101
Pathopysiology of Stone Formation (uric acid stone)
Evaluation:. observation of daily urinary pH . determining the serum and urinary uric acid levels, assessing the degree of ingestion of dietary purines. If the patient has evidence of hyperuricemia, evaluation should include a brief survey to rule out myeloproliferative or neoplastic disease . microscopic examination of the urine

102
Pathopysiology of Stone Formation (uric acid stone)
Therapy:. instructing the patient to drink enough fluids to ensure urinary output in excess of 1500 to 2000 mL/day The urine should be alkalinized to a level between 6.5 and 7. NaHCO3 650mg qid or Kcitrate meq qid Polycitrate K – 15cc qid or crystals 1pk qid Attempts at alkalinization of the urine to a pH higher than 7.0 should be avoided. At a higher pH, there is a danger of increasing the risk of calcium phosphate stone formation.

103
Pathopysiology of Stone Formation (uric acid stone)
If the patient has hyperuricemia, or if urinary uric acid excretion is greater than 1200 mg/day, the patient should be additionally treated with allopurinol, 300 to 600 mg/day. Complications of allopurinol include skin rash, drug fever, and attack of acute gout. Rarely, an exfoliative skin reaction with hemorrhagic skin lesions and systemic vasculitis .

104
Pathopysiology of Stone Formation Cystine stones
Cystine stones account for about 1% of all urinary calculi and occur only in patients who have cystinuria . Cystinuria is an autosomal recessive disorder characterized by a defect in intestinal and renal tubular transport of dibasic amino acids, resulting in excessive urinary excretion of cystine .

105
Pathopysiology of Stone Formation Cystine stones
accumulation of cystine causes crystallization when concentrations rise above the saturation point (approximately 250 mg cystine per liter of urine) Cystine stones are radiopaque. The stones are yellowish and have a waxy appearance. They are often multiple, are large, and may form staghorns. Cystinuria can cause renal stones in childhood, but the peak of clinical expression is in the 2nd and 3rd decades of life.
 Cystine stones are radiopaque. The stones are yellowish and have a waxy appearance. They are often multiple, are large, and may form staghorns. Cystinuria can cause renal stones in childhood, but the peak of clinical expression is in the 2nd and 3rd decades of life.")
106
Pathopysiology of Stone Formation Cystine stones
Diagnosis:. The first-morning urine specimen should be examined for the presence of typical benzene ring or hexagonal cystine crystals sodium nitroprusside spot test, which turned purple in the presence of cystine If the screening test is positive, urinary cystine excretion should be quantitated with amino acid chromatography. A level of greater than 250 mg per 24 hours is usually diagnostic of cystinuria.

107
Pathopysiology of Stone Formation Cystine stones
Treatment:. The goal of therapy is to lower cystine concentration in urine below its level of solubility Diet : Cystine is produced from the essential amino acid methionine, which is abundant in meat, poultry, fish, and dairy products. Thus, a low-methionine diet decreases urinary cystine excretion.

108
Pathopysiology of Stone Formation Cystine stones
Oral Hydration and Alkalinization:. increasing the urinary output to 3 L/day allows dissolution of existing stones and prevention of new cystine stones at urinary cystine excretion of up to 750 mg/day. fruit juices may have a dual benefit because they provide not only water, but also alkali Because the pKa of cystine is 8.3, alkalinization above 7.5 is necessary for the dissolution of cystine crystals.

109
Pathopysiology of Stone Formation Cystine stones
Sodium bicarbonate (15 to 25 g/day) and potassium citrate (15 to 20 mmol two to three times a day) are commonly used for alkalinizing urine. Acetazolamide (250 mg three times a day) increases urinary bicarbonate excretion by inhibiting carbonic anhydrase. It can be used to augment the alkalinization achieved with bicarbonate or citrate Urinary cystine excretion can be reduced by the administration of glutamine (2 g/day in three divided doses)
 and potassium citrate (15 to 20 mmol two to three times a day) are commonly used for alkalinizing urine. Acetazolamide (250 mg three times a day) increases urinary bicarbonate excretion by inhibiting carbonic anhydrase. It can be used to augment the alkalinization achieved with bicarbonate or citrate. Urinary cystine excretion can be reduced by the administration of glutamine (2 g/day in three divided doses)")
110
Pathopysiology of Stone Formation Cystine stones
Pharmacologic Agents:. Two agents can be used: D-penicillamine or alpha- mercaptopropionylglycine (MPG). Both agents bind cystine, forming a complex that is soluble in urine. In many patients, cystine stones are so large and so obstructive that procedural therapy should be used initially to debulk or remove the stone.
. Both agents bind cystine, forming a complex that is soluble in urine. In many patients, cystine stones are so large and so obstructive that procedural therapy should be used initially to debulk or remove the stone.")
111
Pathopysiology of Stone Formation Struvite Stones
Struvite Stones (Infection Stones) The stone is composed of magnesium, ammonium, and phosphate, mixed with carbonate. Struvite calculi have also been commonly referred to as infection or triple-phosphate stones and account for 2% to 20% of all stones 60-90% of staghorns -F:M 2:1
 The stone is composed of magnesium, ammonium, and phosphate, mixed with carbonate. Struvite calculi have also been commonly referred to as infection or triple-phosphate stones and account for 2% to 20% of all stones % of staghorns. -F:M 2:1.")
112
Pathopysiology of Stone Formation Struvite Stones
Pathogenesis Two conditions must coexist for the crystallization of struvite—urine pH of 7.2 or above and ammonia in the urine. The driving force behind struvite stones is infection of the urine with urease-producing bacteria. the hydrolysis of urea releases both an acid (carbonic acid) and a base (ammonia). Because two molecules of ammonia are produced from one molecule of urea, neutralization of the base is incomplete. As a result, the urinary pH rises.
 and a base (ammonia). Because two molecules of ammonia are produced from one molecule of urea, neutralization of the base is incomplete. As a result, the urinary pH rises.")
113
Pathopysiology of Stone Formation Struvite Stones
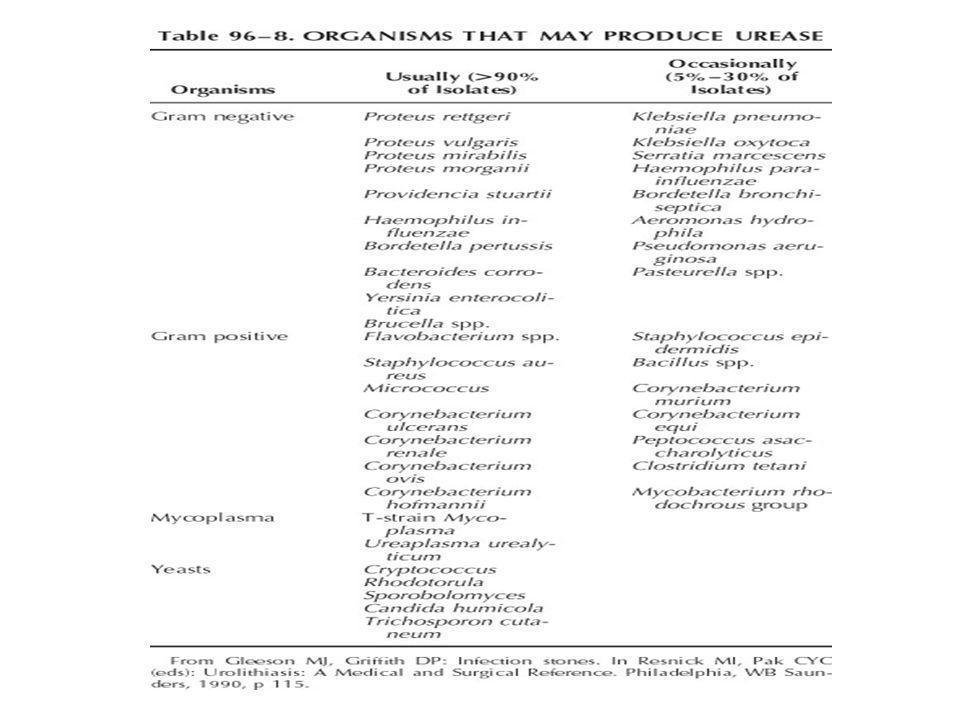
The most common urease-producing pathogens are Proteus, Klebsiella, Pseudomonas, and Staphylococcus. Proteus mirabilis the most common Bacteria may be involved in stone formation by damaging the mucosal layer of the urinary tract, resulting in both increased bacterial colonization and crystal adherence. It has been proposed that ammonium, may alter the glycosaminoglycan layer present on the surface of the transitional cell layer and significantly increase bacterial adherence to normal bladder mucosa.

115
Pathopysiology of Stone Formation Struvite Stones
Risk Factor:. Chronic indwelling catheters Urinary diversion Neurogenic bladder Anatomic abnormalities FB Female Sex

116
Pathopysiology of Stone Formation Struvite Stones
Clinical Presentation :. the symptoms of acute pyelonephritis, including fevers, chills, flank pain, dysuria, frequency, urgency, and malodorous, cloudy urine. Women are more often affected with struvite calculi than are men, probably because of an increased susceptibility to urinary tract colonization. This stone type accounts for the majority of all staghorn calculi.

117
Pathopysiology of Stone Formation Struvite Stones
Xanthogranulomatous pyelonephritis pure struvite calculi were significantly less likely to have metabolic anomalies on 24-hour urine evaluation than were those patients with mixed compositions of struvite and calcium oxalate.

118
Pathopysiology of Stone Formation Struvite Stones
The preferred management of struvite calculi involves aggressive surgical approaches. followed by supportive medical therapy to prevent recurrent urinary tract infection. The American Urological Association Guidelines Committee has released updated guidelines that strongly recommend endoscopy-based therapy (i.e., percutaneous nephrolithotomy) as the first-line therapy for management of complex renal staghorn calculi. This report noted that complete elimination of all infected stone material is essential for the prevention of recurrent struvite stone formation.
 as the first-line therapy for management of complex renal staghorn calculi. This report noted that complete elimination of all infected stone material is essential for the prevention of recurrent struvite stone formation.")
119
Pathopysiology of Stone Formation Struvite Stones
Procedural Therapy :. To cure infection stones, needs to remove them completely. Percutaneous nephrolithotomy has been used increasingly for the treatment of staghorn calculi and has replaced open stone surgery in all but the rarest of instances. anatrophic nephrolithotomy is relegated to the few patients who have a complete staghorn calculus associated with infundibular stenosis or distortion of intrarenal anatomy.

120
Pathopysiology of Stone Formation Struvite Stones
Extracorporeal shock-wave lithotripsy (ESWL) is a less invasive procedure than percutaneous nephrolithotomy. stone-free results ranging from 30% to 66% have been achieved Most clinicians use a combination of percutaneous nephrolithotomy and ESWL for the treatment of patients with large staghorn calculi, particularly if many branches of the collecting system are involved.
 is a less invasive procedure than percutaneous nephrolithotomy. stone-free results ranging from 30% to 66% have been achieved. Most clinicians use a combination of percutaneous nephrolithotomy and ESWL for the treatment of patients with large staghorn calculi, particularly if many branches of the collecting system are involved.")
121
Pathopysiology of Stone Formation Struvite Stones
Medical Treatment Antibiotics Long-term, culture-specific antimicrobials often reduce the bacterial burden, even if they do not completely sterilize the urine Bacteria are still located on the surface or within the lattice of the stones, however, and thus reinfection is common with cessation of antibiotic therapy.

122
Pathopysiology of Stone Formation Struvite Stones
The majority of urease-producing infections are caused by P. mirabilis, more than 90% of which are sensitive to penicillin or ampicillin Tetracyclines or fluoroquinolones such as ciprofloxacin or norfloxacin can be used for the treatment of patients with Pseudomonas or Ureaplasma urinary tract infections Antibiotics are an adjunct to procedural therapy and should be used to prevent stone recurrences or growth after operative procedures.

123
Pathopysiology of Stone Formation Struvite Stones
acetohydroxamic acid potent irreversible inhibitor of urease and clinically is effective in lowering pH and ammonia level. acetohydroxamic acid be used in conjunction with antibiotic therapy in patients with infection stones in whom surgical intervention is contraindicated. Diet :. A low-calcium, low-phosphorus diet with aluminum gels was recommended

124
Pathopysiology of Stone Formation Struvite Stones
Irrigation and Chemolysis:. Important aspect of medical treatment is the dissolution of calculi with irrigation. no irrigation be attempted until the urine is completely sterile. nephrostomy tube is left in place postoperatively. a percutaneous nephrostomy catheter may be inserted if pt not fit for surg.

125
Pathopysiology of Stone Formation Struvite Stones
the renal pelvis is first irrigated with sterile saline solution at a rate of 120 mL/hr for 24 to 48 hours, beginning on the fourth or fifth postoperative day. The patient is observed carefully for development of fever or any flank discomfort and for elevation of serum creatinine, magnesium, or phosphate levels.

126
Pathopysiology of Stone Formation Struvite Stones
If, after 48 hours, the patient's condition remains satisfactory and if there is no infection, no leakage, and no fever or flank discomfort, irrigation is begun with an appropriate solution. Suby’s solution G (pH 4.0) hemiacidrin (pH 3.9) The progress of irrigation is followed by radiographic tomography of the calculi at intervals.
 hemiacidrin (pH 3.9) The progress of irrigation is followed by radiographic tomography of the calculi at intervals.")
127
Miscellaneous Stones Xanthine and Dihydroxyadenine Stones
Xanthine stones are a rare stone. confused with uric acid stones because both are radiolucent. result of an inherited disorder in the catabolic enzyme xanthine dehydrogenase (XDH) or xanthine oxidase, which catalyzes the conversion of xanthine to uric acid. Because xanthine is poorly soluble in urine, the high levels of xanthine that accumulate in XDH deficiency lead to xanthine stones
 or xanthine oxidase, which catalyzes the conversion of xanthine to uric acid. Because xanthine is poorly soluble in urine, the high levels of xanthine that accumulate in XDH deficiency lead to xanthine stones.")
128
Miscellaneous Stones Allopurinol, which inhibits XDH andwhich is used to treat hyperuricemia and hyperuricosuria, can, at very high levels, predispose to xanthine stones. This side effect is uncommon, because the drug causes only partial inhibition of the enzyme and rarely reduces serum uric acid to levels lower than 3 mg/dL. Children with inherited deficiencies of adenine phosphoribosyltransferase (APRT) can also present in infancy with renal complications and stones.
 can also present in infancy with renal complications and stones.")
129
Miscellaneous Stones Ammonium acid urate stones represent less than 1% of all stones. Conditions associated with ammonium acid urate crystallization include laxative abuse, recurrent urinary tract infection, recurrent uric acid stone formation, and inflammatory bowel disease. stone formation due to laxative abuse has been postulated to be the result of dehydration due to gastrointestinal fluid loss causing intracellular acidosis and enhanced ammonia excretion. Because urinary sodium is very low with laxative use, urate complexes with abundant ammonia, thereby leading to urinary supersaturation of ammonium acid urate.

130
Miscellaneous Stones Matrix calculi are found predominantly in individuals with infections caused by urease- producing organisms. The stones are radiolucent and may be confused with uric acid calculi. In most instances, surgical manipulation is required for their removal because they are not dissolved by any means yet known.

131
Miscellaneous Stones Medications That Directly Promote Stone Formation
Indinavir Stones. Indinavir sulfate is a protease inhibitor ,effective in increasing CD4+ cell counts and decreasing HIV-RNA titers in patients infected with (HIV) ,incidence of 4% to 13%. individuals taking indinavir on a regular basis are at high risk of producing indinavir stones due to the high urinary excretion and poor solubility of the drug at physiologic urinary pH. may not be visible on plain film radiography or CT. These calculi can be quite soft and often dissipate rapidly during endoscopy or shockwave lithotripsy.
 ,incidence of 4% to 13%. individuals taking indinavir on a regular basis are at high risk of producing indinavir stones due to the high urinary excretion and poor solubility of the drug at physiologic urinary pH. may not be visible on plain film radiography or CT. These calculi can be quite soft and often dissipate rapidly during endoscopy or shockwave lithotripsy.")
132
Miscellaneous Stones Guaifenesin and Ephedrine:.Individuals consuming large quantities of over-the-counter cough medicines containing ephedrine or guaifenesin are at risk of developing stones derived mainly from metabolites of these medicines. The stones are radiolucent on conventional radiography but radiopaque on computed tomography (CT). treated with a variety of methods, including shockwave lithotripsy, endoscopy, and alkalinization therapy
. treated with a variety of methods, including shockwave lithotripsy, endoscopy, and alkalinization therapy.")
133
Miscellaneous Stones Triamterene stones : triamterene is a potassium- sparing diuretic commonly used for the treatment of hypertension. It is a very uncommon stone composition, accounting for only 0.4% of 50,000 calculi in one report. Up to 70% of orally administered triamterene appears in urine, and a few patients have developed either pure or mixed triamterene stones. requiring cessation of this medication, triamterene is not recommended as an adjunct to thiazides during the treatment of hypercalciuric states.

134
Miscellaneous Stones Anatomic Predisposition to Stones:.
(UPJ) obstruction the incidence is nearly 20% patients with UPJ obstruction and concurrent renal calculi carry the same metabolic risks as other stone formers in the general population hypercalciuria in 46% of patients, hyperuricosuria in 11%, hypocitraturia in 13%, primary hyperpara- thyroidism in 13%, and RTA in 3%. Treatment of patients reduced their rate of recurrence.
 obstruction the incidence is nearly 20% patients with UPJ obstruction and concurrent renal calculi carry the same metabolic risks as other stone formers in the general population. hypercalciuria in 46% of patients, hyperuricosuria in 11%, hypocitraturia in 13%, primary hyperpara- thyroidism in 13%, and RTA in 3%. Treatment of patients reduced their rate of recurrence.")
135
Miscellaneous Stones Horseshoe kidneys occur with a prevalence of 0.25% but have an associated rate of renal calculi of 20% Because of the high insertion of the ureter into the renal pelvis, there is a relative impairment of renal drainage, predisposing to UPJ obstruction. the risk of stone formation due to urinary stasis rather than to metabolic derangements.

136
Miscellaneous Stones Caliceal diverticula are associated with stones in up to 40% of patients. Medullary sponge kidney (MSK) is a disorder characterized by ectasia of the renal collecting ducts. Nephrocalcinosis and renal calculi are frequent complications of MSK. RTA has not been firmly established as a major cause of stone formation in patients with MSK, and hypercalciuria and hypocitraturia are likely the primary risk factors.
 is a disorder characterized by ectasia of the renal collecting ducts. Nephrocalcinosis and renal calculi are frequent complications of MSK. RTA has not been firmly established as a major cause of stone formation in patients with MSK, and hypercalciuria and hypocitraturia are likely the primary risk factors.")
137
Miscellaneous Stones Stones in Pregnancy
Symptomatic stones during pregnancy occur at a rate of 1 in 250 pregnant women. The majority of symptomatic stones occur in the second and third trimester of pregnancy. symptoms of flank pain or hematuria. The diagnosis can be difficult; up to 28% of women are misdiagnosed.

138
Miscellaneous Stones Important physiologic changes in the kidney occur during pregnancy that modulate urinary stone risk factors:. Renal blood flow increases, leading to a 30% to 50% rise in glomerular filtration rate, which subsequently increases the filtered loads of calcium, sodium, and uric acid. Hypercalciuria is enhanced by placental production of 1,25(OH)2D3, which increases intestinal calcium absorption and secondarily suppresses PTH. Hyperuricosuria has also been reported as a result of increased filtered load of uric acid
2D3, which increases intestinal calcium absorption and secondarily suppresses PTH. Hyperuricosuria has also been reported as a result of increased filtered load of uric acid.")
139
Clinical Presentation
Acute Stone Episode A urinary calculus usually presents with an acute episode of renal or ureteral colic as the result of a stone obstructing the urinary tract. There are five locations where stones can be impacted in the urinary tract. First, stones may become impacted in a calyx of the upper urinary tract. The second area in which a calculus may become impacted is the ureteropelvic junction.

140
Clinical Presentation
The third area of impaction is at or near the pelvic brim, where the ureter begins to arch over the iliac vessels posteriorly into the true pelvis. The fourth area, especially in females, is the posterior pelvis, where the ureter is crossed anteriorly by the pelvic blood vessels and by the broad ligament. Finally, the most constricted area through which the urinary calculus must pass is the ureterovesical junction, which is the most common site of impaction

141
Clinical Presentation
left: Ureteropelvic stone. Severe costovertebral angle pain from capsular and pelvic distention; acuterenal and urethral pain from hyperperistalsis of smooth muscl of calyces, pelvis, and ureter, with pain radiating along the course of the ureter (and into the testicle, since the nerve supply to the kidney and testis is the same.) The testis is hypersensitive. right: Midureteral stone. Same as abovebut with more pain in the lower abdominal quadrant.
 The testis is hypersensitive. right: Midureteral stone. Same as abovebut with more pain in the lower abdominal quadrant.")
142
Clinical Presentation
Low ureteral stone: Same as above, with pain radiating into bladder, vulva, or scrotum. The scrotal wall is hyperesthetic. Testicular sensitivity is absent. When the stone approaches the bladder, urgency and frequency with burning on urination develop as a result of inflammation of the bladder wallaround the ureteral orifice.

143
Clinical Presentation
Renal colic : Often at night or in morning, starts in flank and radiates to groin. If stone lower down often get lower abd pain . irritative voiding sy if at UVJ. Often nausea since autonomic N in celiac ganglion supply stomach and kidney for autonomic nerves Most pain from partially obstructing moving stones. Takes 4-6 hrs for initial pain episode to subside.

144
Clinical Presentation
Physical Signs:. Individuals with urinary lithiasis can rarely find comfort in any position. Fever is not present unless urinary infection occurs . Heart rate and blood pressure may be elevated because of pain. Examination of the abdomen reveals moderate, deep tenderness on palpation over the location of the calculus and the area of the loin.

145
URINALYSIS Uncomplicated stone,may reveals RBC with few WBC or Bacteria . Infected urine has RBC ,WBC and bacteria ,white cells cast are diagnostic of pyelonephritis . Normal does not rule out urological pathology . Crystals help to know the compostion of calculi.

146
Scanning electron micrographs of various urinary crystals
Scanning electron micrographs of various urinary crystals. A, Apatite; B, struvite; C, calcium oxalate dihydrate; D, calcium oxalate monohydrate; E, cystine; F, ammonium acid urate; G, brushite.

147
Radiographic Examination
Plain Abdominal Films: plain Kidney-Ureter-Bladder radiographs. Ca phos - apatite - most radiopaque. Nephrocalcinosis : stars on a dark night - in medulary spounge kidney. Staghorn : struvite, cystine, uric acid. Radiolucent :pure uric, xanthine, dehydroxyadenine, matrix, triamteren.

148
Radiographic Examination
Intravenous pyelography:. may be obtained to confirm the presence of radiolucent stones and also to identify any anatomic abnormalities that may predispose the patient to stone formation. Has limitations – radiolucent stones, small stones can be missed esp at UVJ, filling defect not always a stone, risk of dye allergy, x-ray exposure.

149
Radiographic Examination
Ultrasonography:. Ultrasound is a noninvasive method of demonstrating both the urinary stone and the consequent hydronephrosis. Color Doppler ultrasound examination may demonstrate increased resistive index in the obstructed kidney and asymmetry or absence of ureteral jets in the urinary bladder. Edema and small calculi missed on an IVP can be appreciated with such studies

150
Radiographic Examination
Computed tomography:. Spiral CT now investigation of choice in patients presenting with acute renal colic. Sens %, Spec % Advantages over IVP – quicker, no contrast, show up radiolucent calc, low rad dose, potential for other Dx, don’t need to wait for Cr, no dye to interfere with other imaging studies, able to measure stone more accurately Uric acid stones are visualized no differently from calcium oxalate stones. Matrix calculi have adequate amounts of calcium to be visualized easily by CT.

151
Radiographic Examination
Magnetic resonance imaging (MRI) specifically used to visualize the urinary tract has been termed magnetic resonance (MR) urography and has been reported to be effective in detecting urinary tract dilation . MRI is a poor study to document urinary stone disease.
 specifically used to visualize the urinary tract has been termed magnetic resonance (MR) urography and has been reported to be effective in detecting urinary tract dilation . MRI is a poor study to document urinary stone disease.")
152
Diagnostic and Treatment Decision Process
After a urolith is diagnosed, the first assessment is of the degree of seriousness of the disease process 20% to 40% of patients with stone attacks may need hospital admission. Most patients with RC pain relief from intramuscular injection of 50 to 100 mg of meperidine or 10 to 15 mg of morphine.

153
Admit if: 1. Pain not controlled with Po meds. 2. Calculus Anuria , usualy solitary kidney or bilat stones. 3. Infection , esp. when there is obstruction. 4. Emesis. Most calculi smaller than 4 to 5 mm pass spontaneously.

154
Analysis of Urinary Stones
Most medical therapy for stone disease is now based on analysis of calculi, and decisions about proper procedures for treatment require knowledge of stone composition

155
Medical evaluation History
Diet and fluid intake Medications Infection Activity level Systemic disease Genetics Anatomy Previous surgery

156
Medical evaluation Evaluation of the Patient with the First Stone
All patients should have excretory urography, urinalysis, urine culture, complete blood count, and SMA-20. All stones should be analyzed. If the stone cannot be recovered, a urine cystine screen should be performed. The presence of multiple stones or nephrocalcinosis on IVU indicates the need for a more detailed metabolic work-up and aggressive medical therapy

157
Medical evaluation Evaluation of the Patient with Multiple or Recurrent Stones

158
Medical evaluation Medical therapy for stone disease serves two purposes: treatment of the acute episode and prevention of stone recurrences or new stone formations Who Needs Medical Therapy? Between 25% and 75% of all patients who present with an initial stone develop a recurrent stone over prolonged follow-up, lasting from 10 to 20 years .

159
Medical evaluation Patients who have had only their first stone episode do not undergo a formal metabolic evaluation but rather have a urinalysis, a urine culture, and a blood chemical profile, including calcium, uric acid, electrolytes, and creatinine concentration

160
MEDICAL MANAGEMENT CONSERVATIVE MEDICAL MANAGEMENT
Fluid Recommendations: Patients should be strongly encouraged to consume enough fluids to produce 2 liters of urine per day. Water hardness is unlikely to play a significant role in recurrence risk. Carbonated water may confer some protective benefit. Soda flavored with phosphoric acid may increase stone risk, whereas soda with citric acid may decrease risk. Citrus juices (particularly lemon juice) may be a useful adjunct to stone prevention.
 may be a useful adjunct to stone prevention.")
161
MEDICAL MANAGEMENT CONSERVATIVE MEDICAL MANAGEMENT
DIETARY RECOMMENDATIONS Randomized studies have confirmed the advantage of a diet with moderate animal protein (meat) intake. In combination with animal protein restriction and moderate calcium ingestion, a reduced sodium diet will decrease stone episodes by approximately 50%. OBESITY is an independent risk factor for nephrolithiasis, particularly for women. Obese patients have a higher propensity for uric acid calculi. High-protein, low-carbohydrate diets may increase the risk of stone formation.
 intake. In combination with animal protein restriction and moderate calcium ingestion, a reduced sodium diet will decrease stone episodes by approximately 50%. OBESITY. is an independent risk factor for nephrolithiasis, particularly for women. Obese patients have a higher propensity for uric acid calculi. High-protein, low-carbohydrate diets may increase the risk of stone formation.")
162
MEDICAL MANAGEMENT CONSERVATIVE MEDICAL MANAGEMENT
ROLE OF DIETARY CALCIUM:. Dietary calcium avoidance actually increases stone recurrence risk. Calcium supplementation is likely to be safest when it is taken with meals. Calcium citrate appears to be a more stone-friendly calcium supplement because of the additional inhibitor action of citrate. OXALATE AVOIDANCE:. Avoidance of excess dietary oxalate loading is reasonable and intuitive. Vitamin C in large doses may increase the risk of stone recurrence. Doses should probably be limited to 2 g/day.

165
Urinary stone disease Thank you

Similar presentations

















 Calcium phosphate stones (2) Magnesium ammonium phosphate stones (3)Calcium oxalate stones >")









 Triple phosphate237 (26.4%) Phosphate119 (13.4%) Uric.>")




