Download presentation
Presentation is loading. Please wait.

1
Dr Γιώργος Κρασόπουλος MD, PhD, MRCS(Eng), FRCS-CTh(Eng) Καρδιοχειρουργός www. καρδιοχειρουργός.gr www. καρδιοχειρουργός.gr

2
Surgical pulmonary valve replacement: Surgical pulmonary valve replacement: >30 years, >5000 papers Trans-femoral pulmonary valve implantation Trans-femoral pulmonary valve implantation Melody – Medtronic: 9-10 years of experience, <40 papers SAPIEN – Edwards: 2-3 years of experience, <<10 papers Trans-ventricular pulmonary valve implantation: Trans-ventricular pulmonary valve implantation: <1year, <<5 papers

4
Indications for Use: Indications for Use: The Melody TPV is indicated for use as an adjunct to surgery in the management of pediatric and adult patients with the following clinical conditions: Existence of a full (circumferential) RVOT conduit that was equal to or greater than 16 mm in diameter when originally implanted and Dysfunctional RVOT conduits with a clinical indication for intervention, and either: regurgitation: moderate regurgitation, or stenosis: mean RVOT gradient 35 mm Hg Contraindications: Contraindications: None known.
 RVOT conduit that was equal to or greater than 16 mm in diameter when originally implanted and Dysfunctional RVOT conduits with a clinical indication for intervention, and either: regurgitation: moderate regurgitation, or stenosis: mean RVOT gradient 35 mm Hg Contraindications: Contraindications: None known.")
5
Indications for Use: Indications for Use: The Melody TPV is indicated for use as an adjunct to surgery in the management of pediatric and adult patients with the following clinical conditions: Existence of a full (circumferential) RVOT conduit that was equal to or greater than 16 mm in diameter when originally implanted and Dysfunctional RVOT conduits with a clinical indication for intervention, and either: regurgitation: moderate regurgitation, or stenosis: mean RVOT gradient 35 mm Hg Contraindications: Contraindications: None known. Very specific indications

6
Indications for Use: Indications for Use: The Melody TPV is indicated for use as an adjunct to surgery in the management of pediatric and adult patients with the following clinical conditions: Existence of a full (circumferential) RVOT conduit that was equal to or greater than 16 mm in diameter when originally implanted and Dysfunctional RVOT conduits with a clinical indication for intervention, and either: regurgitation: moderate regurgitation, or stenosis: mean RVOT gradient 35 mm Hg Contraindications: Contraindications: None known. Everything else is off label & it should be treated as such! it should be treated as such! Very specific indications

8
Policlinico San Donato

9
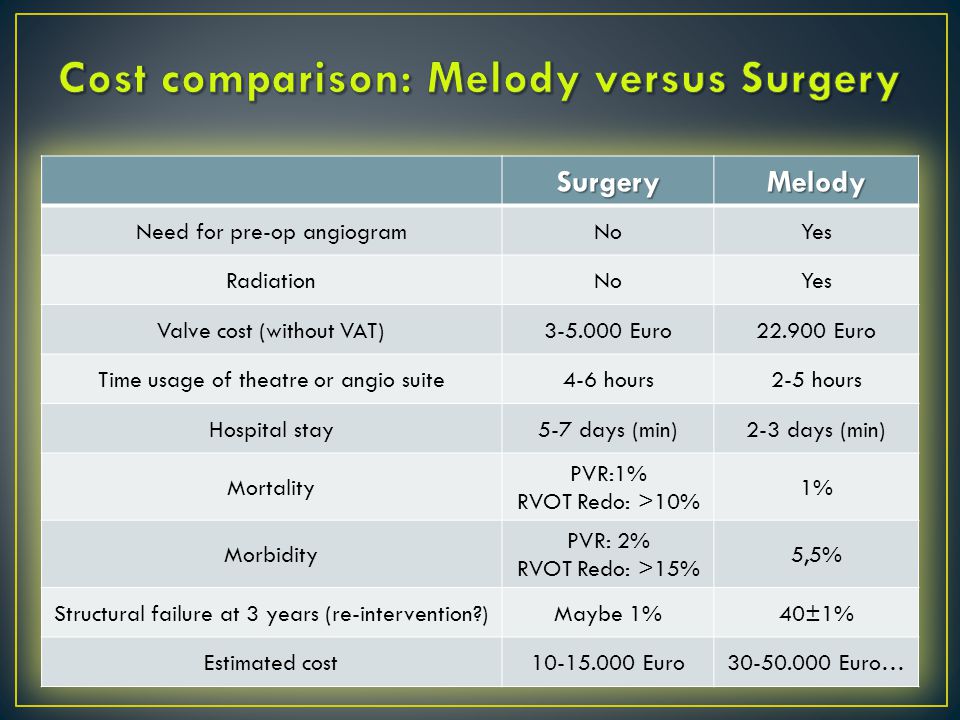
Post implantation cost for the first year well over 4000 Euros for Melody & Just two ECHOs for surgery! Policlinico San Donato

10
Stent fracture resulting in recurrent obstruction Endocarditis Embolization or migration of the device Valvular dysfunction (stenosis or regurgitation) Paravalvular leak Valvular thrombosis Pulmonary thromboembolism Haemolysis Conduit-induced distortion of the initial implant
 Paravalvular leak Valvular thrombosis Pulmonary thromboembolism Haemolysis Conduit-induced distortion of the initial implant")
11
J Am Coll Cardiol. 2009 Oct 27;54(18):1722-9. J Am Coll Cardiol. 2011 Nov 15;58(21):2248-56.
: J Am Coll Cardiol Nov 15;58(21):")
12
Eur Radiol 2011; 21:36-45

14
Semin Thorac Cardiovasc Surg Pediatr Card Surg Annu 2009; 12:112-7

17
When does it stop!

18
150 patients Freedom from a diagnosis of metal stent fracture was: 77±4% at 14 months (after the 1-year evaluation window) and 60±9% at 39 months (3-year window). Among patients with a MSF, freedom from RVOT re-intervention after metal stent fracture diagnosis was 49±10% at 2 years. New prestent, or bioprosthetic valve (combined variable) was associated with longer freedom from MSF (P<0.001). Valve compression (P=0.01) and apposition to the anterior chest wall (P=0.02) were associated with shorter freedom from MSF. Circ Cardiovasc Interv. 2011 Dec 1;4(6):602-14. Epub 2011 Nov 9.
 was associated with longer freedom from MSF (P<0.001). Valve compression (P=0.01) and apposition to the anterior chest wall (P=0.02) were associated with shorter freedom from MSF. Circ Cardiovasc Interv Dec 1;4(6): Epub 2011 Nov 9..")
19
150 patients Freedom from a diagnosis of metal stent fracture was: 77±4% at 14 months (after the 1-year evaluation window) and 60±9% at 39 months (3-year window). Among patients with a MSF, freedom from RVOT re-intervention after metal stent fracture diagnosis was 49±10% at 2 years. New prestent, or bioprosthetic valve (combined variable) was associated with longer freedom from MSF (P<0.001). Valve compression (P=0.01) and apposition to the anterior chest wall (P=0.02) were associated with shorter freedom from MSF. Circ Cardiovasc Interv. 2011 Dec 1;4(6):602-14. Epub 2011 Nov 9. Big problem that gets bigger with time!
 was associated with longer freedom from MSF (P<0.001). Valve compression (P=0.01) and apposition to the anterior chest wall (P=0.02) were associated with shorter freedom from MSF. Circ Cardiovasc Interv Dec 1;4(6): Epub 2011 Nov 9. Big problem that gets bigger with time!.")
20
150 patients Freedom from a diagnosis of metal stent fracture was: 77±4% at 14 months (after the 1-year evaluation window) and 60±9% at 39 months (3-year window). Among patients with a MSF, freedom from RVOT re-intervention after metal stent fracture diagnosis was 49±10% at 2 years. New prestent, or bioprosthetic valve (combined variable) was associated with longer freedom from MSF (P<0.001). Valve compression (P=0.01) and apposition to the anterior chest wall (P=0.02) were associated with shorter freedom from MSF. Circ Cardiovasc Interv. 2011 Dec 1;4(6):602-14. Epub 2011 Nov 9.
 was associated with longer freedom from MSF (P<0.001). Valve compression (P=0.01) and apposition to the anterior chest wall (P=0.02) were associated with shorter freedom from MSF. Circ Cardiovasc Interv Dec 1;4(6): Epub 2011 Nov 9..")
21
150 patients Freedom from a diagnosis of metal stent fracture was: 77±4% at 14 months (after the 1-year evaluation window) and 60±9% at 39 months (3-year window). Among patients with a MSF, freedom from RVOT re-intervention after metal stent fracture diagnosis was 49±10% at 2 years. New prestent, or bioprosthetic valve (combined variable) was associated with longer freedom from MSF (P<0.001). Valve compression (P=0.01) and apposition to the anterior chest wall (P=0.02) were associated with shorter freedom from MSF. Circ Cardiovasc Interv. 2011 Dec 1;4(6):602-14. Epub 2011 Nov 9. Big problem that gets bigger with time! & We have to do it again!
 was associated with longer freedom from MSF (P<0.001). Valve compression (P=0.01) and apposition to the anterior chest wall (P=0.02) were associated with shorter freedom from MSF. Circ Cardiovasc Interv Dec 1;4(6): Epub 2011 Nov 9. Big problem that gets bigger with time. & We have to do it again!.")
22
150 patients Freedom from a diagnosis of metal stent fracture was: 77±4% at 14 months (after the 1-year evaluation window) and 60±9% at 39 months (3-year window). Among patients with a MSF, freedom from RVOT re-intervention after metal stent fracture diagnosis was 49±10% at 2 years. New prestent, or bioprosthetic valve (combined variable) was associated with longer freedom from MSF (P<0.001). Valve compression (P=0.01) and apposition to the anterior chest wall (P=0.02) were associated with shorter freedom from MSF. Circ Cardiovasc Interv. 2011 Dec 1;4(6):602-14. Epub 2011 Nov 9.
 was associated with longer freedom from MSF (P<0.001). Valve compression (P=0.01) and apposition to the anterior chest wall (P=0.02) were associated with shorter freedom from MSF. Circ Cardiovasc Interv Dec 1;4(6): Epub 2011 Nov 9..")
23
150 patients Freedom from a diagnosis of metal stent fracture was: 77±4% at 14 months (after the 1-year evaluation window) and 60±9% at 39 months (3-year window). Among patients with a MSF, freedom from RVOT re-intervention after metal stent fracture diagnosis was 49±10% at 2 years. New prestent, or bioprosthetic valve (combined variable) was associated with longer freedom from MSF (P<0.001). Valve compression (P=0.01) and apposition to the anterior chest wall (P=0.02) were associated with shorter freedom from MSF. Circ Cardiovasc Interv. 2011 Dec 1;4(6):602-14. Epub 2011 Nov 9. Big problem that gets bigger with time! & We have to do it again! & It works better if we put a bioprosthesis first!
 was associated with longer freedom from MSF (P<0.001). Valve compression (P=0.01) and apposition to the anterior chest wall (P=0.02) were associated with shorter freedom from MSF. Circ Cardiovasc Interv Dec 1;4(6): Epub 2011 Nov 9. Big problem that gets bigger with time. & We have to do it again. & It works better if we put a bioprosthesis first!.")
24
150 patients Freedom from a diagnosis of metal stent fracture was: 77±4% at 14 months (after the 1-year evaluation window) and 60±9% at 39 months (3-year window). Among patients with a MSF, freedom from RVOT re-intervention after metal stent fracture diagnosis was 49±10% at 2 years. New prestent, or bioprosthetic valve (combined variable) was associated with longer freedom from MSF (P<0.001). Valve compression (P=0.01) and apposition to the anterior chest wall (P=0.02) were associated with shorter freedom from MSF. Circ Cardiovasc Interv. 2011 Dec 1;4(6):602-14. Epub 2011 Nov 9.
 was associated with longer freedom from MSF (P<0.001). Valve compression (P=0.01) and apposition to the anterior chest wall (P=0.02) were associated with shorter freedom from MSF. Circ Cardiovasc Interv Dec 1;4(6): Epub 2011 Nov 9..")
25
150 patients Freedom from a diagnosis of metal stent fracture was: 77±4% at 14 months (after the 1-year evaluation window) and 60±9% at 39 months (3-year window). Among patients with a MSF, freedom from RVOT re-intervention after metal stent fracture diagnosis was 49±10% at 2 years. New prestent, or bioprosthetic valve (combined variable) was associated with longer freedom from MSF (P<0.001). Valve compression (P=0.01) and apposition to the anterior chest wall (P=0.02) were associated with shorter freedom from MSF. Circ Cardiovasc Interv. 2011 Dec 1;4(6):602-14. Epub 2011 Nov 9. Big problem that gets bigger with time! & We have to do it again! & It works better if we put a bioprosthesis first! & We need a specialist team approach!
 was associated with longer freedom from MSF (P<0.001). Valve compression (P=0.01) and apposition to the anterior chest wall (P=0.02) were associated with shorter freedom from MSF. Circ Cardiovasc Interv Dec 1;4(6): Epub 2011 Nov 9. Big problem that gets bigger with time. & We have to do it again. & It works better if we put a bioprosthesis first. & We need a specialist team approach!.")
26
1. J Thorac Cardiovasc Surg. 2011 Aug;142(2):351-8. Epub 2011 Feb 1. 2. J Thorac Cardiovasc Surg. 1999 Jan;117(1):141-6; discussion 46-7. 3. Ann Thorac Surg. 2003 Feb;75(2):399-410; discussion 410-1.
:141-6; discussion Ann Thorac Surg Feb;75(2): ; discussion")
27
1. J Thorac Cardiovasc Surg. 2011 Aug;142(2):351-8. Epub 2011 Feb 1. 2. J Thorac Cardiovasc Surg. 1999 Jan;117(1):141-6; discussion 46-7. 3. Ann Thorac Surg. 2003 Feb;75(2):399-410; discussion 410-1.
:141-6; discussion Ann Thorac Surg Feb;75(2): ; discussion")
28
1. J Thorac Cardiovasc Surg. 2011 Aug;142(2):351-8. Epub 2011 Feb 1. 2. J Thorac Cardiovasc Surg. 1999 Jan;117(1):141-6; discussion 46-7. 3. Ann Thorac Surg. 2003 Feb;75(2):399-410; discussion 410-1.
:141-6; discussion Ann Thorac Surg Feb;75(2): ; discussion")
29
Surgery is the gold standard technique for pulmonary valve replacement. Surgery is the gold standard technique for pulmonary valve replacement. Percutaneous valve implantation: Percutaneous valve implantation: Has only, very specific indications It is very expensive It has a very high percentage of complications For some patients the percutaneous option can be the only option. For some patients the percutaneous option can be the only option. The decision making on, which technique to deploy to which patient should be a matter of: The decision making on, which technique to deploy to which patient should be a matter of: Specialist centres only Properly trained subspecialists Team work (multidisciplinary meetings) Recorded results which are regularly put under auditing & peer review
 Recorded results which are regularly put under auditing & peer review.")
30
Surgery is the gold standard technique for pulmonary valve replacement. Surgery is the gold standard technique for pulmonary valve replacement. Percutaneous valve implantation: Percutaneous valve implantation: Has only, very specific indications It is very expensive It has a very high percentage of complications For some patients the percutaneous option can be the only option. For some patients the percutaneous option can be the only option. The decision making on, which technique to deploy to which patient should be a matter of: The decision making on, which technique to deploy to which patient should be a matter of: Specialist centres only Properly trained subspecialists Team work (multidisciplinary meetings) Recorded results which are regularly put under auditing & peer review
 Recorded results which are regularly put under auditing & peer review.")
31
Surgery is the gold standard technique for pulmonary valve replacement. Surgery is the gold standard technique for pulmonary valve replacement. Percutaneous valve implantation: Percutaneous valve implantation: Has only, very specific indications It is very expensive It has a very high percentage of complications For some patients the percutaneous option can be the only option. For some patients the percutaneous option can be the only option. The decision making on, which technique to deploy to which patient should be a matter of: The decision making on, which technique to deploy to which patient should be a matter of: Specialist centres only Properly trained subspecialists Team work (multidisciplinary meetings) Recorded results which are regularly put under auditing & peer review
 Recorded results which are regularly put under auditing & peer review.")
32
Surgery is the gold standard technique for pulmonary valve replacement. Surgery is the gold standard technique for pulmonary valve replacement. Percutaneous valve implantation: Percutaneous valve implantation: Has only, very specific indications It is very expensive It has a very high percentage of complications For some patients the percutaneous option can be the only option. For some patients the percutaneous option can be the only option. The decision making on, which technique to deploy to which patient should be a matter of: The decision making on, which technique to deploy to which patient should be a matter of: Specialist centres only Properly trained subspecialists Team work (multidisciplinary meetings) Recorded results which are regularly put under auditing & peer review
 Recorded results which are regularly put under auditing & peer review.")
33
www. καρδιοχειρουργός.gr www. καρδιοχειρουργός.gr

Similar presentations





: doi: /jama Figure Legend:>")








 for surgical mitral valve replacement in infants and children Luis G. Quiñonez, MD, Roger Breitbart,>")






