Download presentation
Presentation is loading. Please wait.

1
Promising Models and Practices with Southeast Asian American Communities
Zha Blong Xiong University of Minnesota Yorn Yan United Cambodian Association of Minnesota

2
Overview of Presentation
Context of Southeast Asian (SEA) Americans in Minnesota. The Citizen Health Care Model to build collaboration between the University and Southeast Asian communities. The Statewide Tobacco Education and Education Project (STEEP) Model. Some evaluation data testing the model. Lessons learned.
 Americans in Minnesota. The Citizen Health Care Model to build collaboration between the University and Southeast Asian communities. The Statewide Tobacco Education and Education Project (STEEP) Model. Some evaluation data testing the model. Lessons learned.")
3
SEA Resettlement in the United States, 1975-1994
40,000 35,000 30,000 25,000 20,000 15,000 10,000 5,000 1975- 1976 1977- 1978 1979- 1980 1981- 1982 1983- 1984 1985- 1986 1987- 1988 1989- 1990 1991- 1992 1993- 1994

4
U.S. Southeast Asian Population
Asian Indians Filipino Hmong = %; Asian Indian = %; Chinese = 23.36%; Vietnamese = 10.81%; Korean = 9.94%; Filipino = 17.84%; Laotian = 1.33%; Cambodian = %; Others = 13.53%

5
Minnesota Southeast Asian Population
Cambodian = 8,140; Hmong = 55,915; Lao = 10,070; and Vietnamese = 22,923 (Total MN Asian Pop = 214,234)
")
6
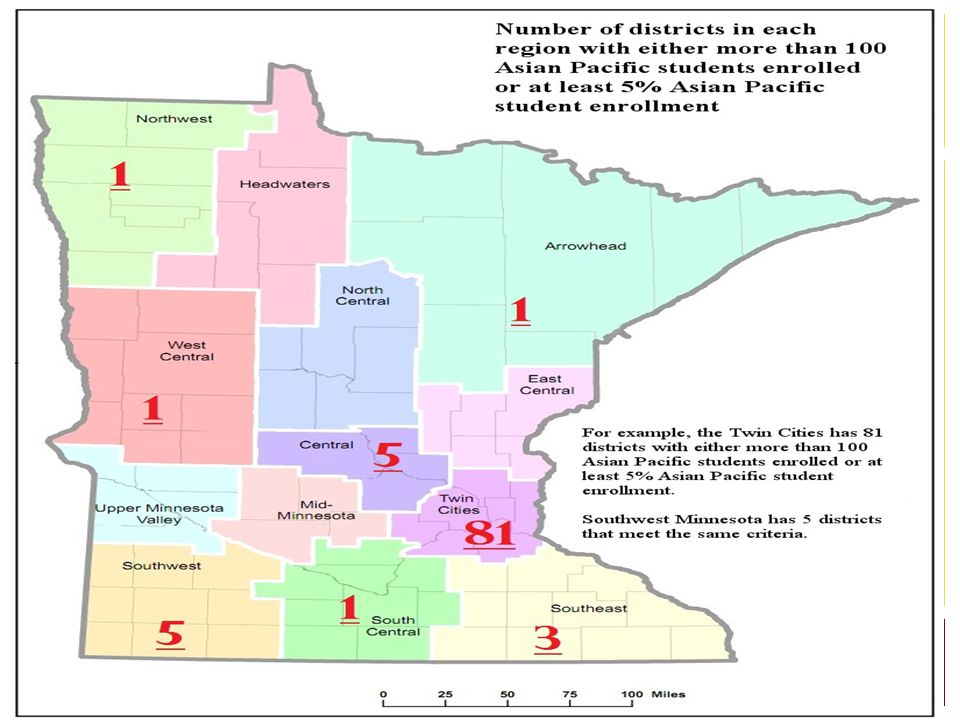
Hmong Vietnamese One county (Ramsey) near Minneapolis, MN, had concentrations of the Asian-alone-or-in-combination population between 10.0 percent and 24.9 percent of the total population. Counties with concentrations of 5.0 percent to 9.9 percent of the Asian alone-or-in-combination population were near all of the metropolitan statistical areas (Minneapolis-St. Paul, Bloomington (MN) mentioned above.
 near Minneapolis, MN, had concentrations of the Asian-alone-or-in-combination population between 10.0 percent and 24.9 percent of the total population. Counties with concentrations of 5.0 percent to 9.9 percent of the Asian alone-or-in-combination population were near all of the metropolitan statistical areas (Minneapolis-St. Paul, Bloomington (MN) mentioned above.")
8
Most Southeast Asians in Minnesota concentrated in urban and poor areas
53% of Minnesota’s Hmong population lives in Ramsey County and 45% within the City of St. Paul. The Hmong comprise 57% of all Asians in Ramsey County nd 65% of Asians in St. Paul ( American Community Survey 5-Year Estimates).
.")
9
Percentage of Household Income below the Poverty Line in St
Percentage of Household Income below the Poverty Line in St. Paul, Ramsey and Hennepin Counties, MN by Race Caucasian African American Hispanic American Indian Asian-non Hmong Hmong St. Paul 3.4 19.2 12.8 17.8 25.8 33.9 Ramsey County 2.6 18.7 12.3 14.1 12.6 31.9 Hennepin County 1.7 19.5 12.7 20.2 6.3 33.7

10
Linguistically Isolated
A recent study found that 81% of first generation respondents reported using a language other than English as their primary language, while 20% of second generation respondents also reported this (Robynn el al., 2010). Source: Census 2000 Data for Minnesota Population.
. Source: Census 2000 Data for Minnesota Population.")
11
Smoking rates Smoking rates in the general population are declining since 2004 (stalled at 20%) Smoking rates in the SEA communities are still high. Some studies show that the prevalence rates for SEAs ages 18 and over ranged from 34% to 70% (Bautista, Ednacot, & Wong, 2005; Chen, 2001; McPhee et al., 1995). A 2009 study of 2,856 Hmong youth and adults in Wisconsin found that 15% of the youth ages reported daily use and 32% ever use. The American Legacy Foundation (2001) reported that the number of Asian American teens who smoke increased from 4.4% in middle school to 33.1% by 12th grade. Blue Cross and Blue Shield of Minnesota’s (2009) SEA study found that men are more likely to smoke (30%) than women (7%).
. A 2009 study of 2,856 Hmong youth and adults in Wisconsin found that 15% of the youth ages reported daily use and 32% ever use. The American Legacy Foundation (2001) reported that the number of Asian American teens who smoke increased from 4.4% in middle school to 33.1% by 12th grade. Blue Cross and Blue Shield of Minnesota’s (2009) SEA study found that men are more likely to smoke (30%) than women (7%).")
12
Engaging the Southeast Asian Communities to Address the Tobacco Use Problem
Community Engagement: Buy-in & Planning Capacity Building Culturally Tailored, Multi-Approached Education Embedding and Systems Change

13
Engaging the Southeast Asian Communities to Address the Tobacco Use Problem
STEEP Collaborative Executive Team (CET) Lao Family Community of Minnesota Lao Advancement Organization of America United Cambodian Association of Minnesota, Inc. Association for the Advancement of Hmong Women in Minnesota Department of Family Social Science, University of Minnesota Association for Nonsmokers-Minnesota
 Lao Family Community of Minnesota. Lao Advancement Organization of America. United Cambodian Association of Minnesota, Inc. Association. for the Advancement of Hmong Women in Minnesota. Department of Family Social Science, University of Minnesota. Association for Nonsmokers-Minnesota.")
14
Community Engagement Buy-in & Planning Model
Citizen Health Care Model’s Principles: The greatest untapped resource for strengthening families and communities is the knowledge, wisdom, and lived experience of community members/citizens. Citizens must be included in the engagement process as producers and contributors, and not a clients or consumers of services. Researchers must come to the collaboration as citizen professionals to identify challenges, sources and nature of the problem, mobilize resources, and generate plans of action together. Source: Doherty & Carroll, 2002; Doherty & Mendenhall, 2006.

15
Community Engagement Buy-in & Planning Process
The Engagement Process for the Statewide Tobacco Education and Engagement Project (STEEP) took 2 Years (supported by ClearWay Minnesota: ): Action plans & program development: Retreat. Data collection: Focus groups. Data collection: Stakeholder interviews. Community leadership groups. The researcher and representatives of the four organizations met to establish roles and expectations, to review goals of the research project, and to draft and finalize the job descriptions for the community facilitators and the research assistant Identified stakeholders for the community leadership groups. Capacity building for the collaborative & staff. Shared decision making and partnership building.
 took 2. Years (supported by ClearWay Minnesota: ): Action plans & program development: Retreat. Data collection: Focus groups. Data collection: Stakeholder interviews. Community leadership groups. The researcher and representatives of the four organizations met to establish roles and expectations, to review goals of the research project, and to draft and finalize the job descriptions for the community facilitators and the research assistant. Identified stakeholders for the community leadership groups. Capacity building for the collaborative & staff. Shared decision making and partnership building.")
16
The STEEP Project Mr. Yorn Yan

17
Dandelion Systems Change

18
Capacity Building Model: LAAMPP Approach: Train-the-trainers
Community Engagement: Buy-in & Planning Capacity Building Culturally Tailored, Multi-Approached Education Embedding and Systems Change Model: LAAMPP Leadership and Advocacy Institute to Advance Minnesota’s Priority Populations project (Lew, Honma, Portugal, & Baezconde-Garbanati, 2008). Build community and cross-cultural capacity for tobacco control Developing a pool of Coaches Approach: Train-the-trainers (Corelli et al., 2007; Orfaly et. el., 2005). Capacity building of the collaboration Staff/Tobacco Educators Volunteers: Community fellows Allies: Community leaders Community members This approach is based on the work of ClearWay Minnesota’s LAAMPP (Leadership and Advocacy Institute to Advance Minnesota’s Parity for Priority Populations) project (Lew, Honma, Portugal, & Baezconde-Garbanati, 2008) and the train-the-trainers model (Corelli et al., 2007; Orfaly, Frances, Campbell, Whittemore, Joly, & Koh, 2005).
. Build community and cross-cultural capacity for tobacco control. Developing a pool of Coaches. Approach: Train-the-trainers. (Corelli et al., 2007; Orfaly et. el., 2005). Capacity building of the collaboration. Staff/Tobacco Educators. Volunteers: Community fellows. Allies: Community leaders. Community members. This approach is based on the work of ClearWay Minnesota’s LAAMPP (Leadership and Advocacy Institute to Advance Minnesota’s Parity for Priority Populations) project (Lew, Honma, Portugal, & Baezconde-Garbanati, 2008) and the train-the-trainers model (Corelli et al., 2007; Orfaly, Frances, Campbell, Whittemore, Joly, & Koh, 2005).")
19
Culturally Tailored, Multi-Approached Education
Community Engagement: Buy-in & Planning Capacity Building Culturally Tailored, Multi-Approached Education Embedding and Systems Change Setting: Places of congregation (“if we build it, people will come” is not working ) Community events Temples Multi-housing units Community-based organizations Materials: Posters, objects, tools, etc. (see samples) Pedagogies: Story telling, demonstrations, and role playing. Evaluation: Pre- and post-tests; retrospective
 Community events. Temples. Multi-housing units. Community-based organizations. Materials: Posters, objects, tools, etc. (see samples) Pedagogies: Story telling, demonstrations, and role playing. Evaluation: Pre- and post-tests; retrospective.")
20
Chemical Poster What it is:
A poster depicting the chemicals present in cigarettes. Why it is used: It is used to alert observers to the dangerous chemicals found in cigarettes. Its message: The chemicals pictured in this poster are chemicals that many observers will recognize. This poster encourages smokers to ask themselves, “If these chemicals are used in each cigarette, why am I still smoking? Retailer: Nimco Inc., , Fax: Its message: The chemicals pictured in this poster are chemicals that many observers will recognize. This poster encourages smokers to ask themselves, “If these chemicals are used in each cigarette, why am I still smoking?

21
Tar Jar What it is: This jar shows the amount of tar a smoker
consumes in one year from smoking a pack (20 cigarettes) a day. Why it is used: It provides a visual picture of the tar that turns the lungs black. Its message: This educational tool teaches the effects of tobacco use on health. Retailer: Nimco Inc., , Fax:
 a day. Why it is used: It provides a visual picture of the tar that turns. the lungs black. Its message: This educational tool teaches the effects of tobacco. use on health. Retailer: Nimco Inc., , Fax:")
22
Community Engagement: Getting Communities & Institutions to Commit to Change
Community Engagement: Buy-in & Planning Capacity Building Culturally Tailored, Multi-Approached Education Embedding and Systems Change Embedding practices and policies Healthy living messages and practices become part of each agency’s programs. Co-presentations and team-focused programs. Systems change practices and policies Develop appropriate language for policies Adopt policies Implement and enforce adopted policies Educate and inform existing state and local policies

23
Commit to Embedding and Systems Change
Community Engagement: Buy-in & Planning Capacity Building Culturally Tailored, Multi-Approached Education Embedding and Systems Change Action taken: Date Initiated Date Completed Comments Initial contact w/ member who knows someone in the entity. Talk with representative(s) of the entity about potential policy. Conversation with and/or present to group about potential policy. Have a conversation with the decision maker or the executive group. Present idea and language of policy and what the entity wants to cover. Help draft policy idea and language to the entity. Revise policy statement. Policy adopted.
 of the entity about potential policy. Conversation with and/or present to group about potential policy. Have a conversation with the decision maker or the executive group. Present idea and language of policy and what the entity wants to cover. Help draft policy idea and language to the entity. Revise policy statement. Policy adopted.")
24
NUMBER OF POLICIES PASSED
TYPE OF POLICY SYSTEMS TOBACCO COMMUNITY BASED ORG. TEMPLE GROUP MULTI- UNIT HOUSING OTHERS Hmong Soccer Tournament (1) Tobacco X No Tobacco Funding (5) Strengthening Comprehensive Policy (5) World Refugee Day (1) Multi-unit Housing (1) Cambodian Temple (1) Lao Temple (1) 20% healthy options (5) Healthy Eating 20% healthy options (1) 20% healthy options (1) Bike racks (5) Active Living
 Tobacco. X. No Tobacco Funding (5) Strengthening Comprehensive Policy (5) World Refugee Day (1) Multi-unit Housing (1) Cambodian Temple (1) Lao Temple (1) 20% healthy options (5) Healthy Eating. 20% healthy options (1) 20% healthy options (1) Bike racks (5) Active Living.")
25
Lessons Learned Collaboration Staff
Shared vision about the community well-being. Trust and respect one another as professional citizens. Commitment from the top of the organizations (i.e., executive directors). Shared leadership and sacrifice at the collaborative level (chair committees, rally, petition, cost to pay grant writer, etc.). The role of the University in the collaboration is key to our program success (i.e., model development, grant writing, and evaluation). The ongoing contributions of the TAs, consultants, and funders to guide, support, and strengthen the collaboration. Staff Capacity building is critical (i.e., demonstrate credibility, buy-in, and trust in the community, esp. with young, second-generation staff). Mentoring and coaching staff play an important role in our successes. Organizational flexibility (in office vs. in the field).
. Shared leadership and sacrifice at the collaborative level (chair committees, rally, petition, cost to pay grant writer, etc.). The role of the University in the collaboration is key to our program success (i.e., model development, grant writing, and evaluation). The ongoing contributions of the TAs, consultants, and funders to guide, support, and strengthen the collaboration. Staff. Capacity building is critical (i.e., demonstrate credibility, buy-in, and trust in the community, esp. with young, second-generation staff). Mentoring and coaching staff play an important role in our successes. Organizational flexibility (in office vs. in the field).")
26
Lessons Learned Evaluation
Evaluation is a challenge when working with low literacy population. The need to balance between delivering the program vs. collecting data An hour training with pre- and post-tests The challenge of using survey to collect data (i.e., response options; right and wrong answers). Reliable vs. practical measures.
. Reliable vs. practical measures.")
27
Lessons Learned Volunteers Program Challenge of retaining volunteers.
Challenge of getting volunteers to commit to advanced training (tier three – two week training and a mentored project). Program Build relationship with people is key to engagement, education, and systems change. If we move too quickly into systems change, the buy-in is not there in the community to pass policies. People need to personalize the problem before they can commit to change.
. Program. Build relationship with people is key to engagement, education, and systems change. If we move too quickly into systems change, the buy-in is not there in the community to pass policies. People need to personalize the problem before they can commit to change.")
28
Please don’t hesitate to contact us if you want to…
Learn more about the Citizen Health Care Model to engage other immigrant and/or low SES communities; Learn more about our STEEP’s Dandelion and Systems Change Model; Have access to our evaluation data; or Know more about our lessons learned and other success stories.

29
CDC’s Program Evaluation Framework Framework for Program Evaluation in Public Health. MMWR 1999;48(No. RR-11) JH: this graphic summarizes the main points of the Steps in Program Evaluation and has the CDC stamp on it. It also references the AEA Evaluation Standards updated document which we can include in their electronic “packet.”

30
American Evaluation Association Evaluation Standards
Utility: credible, negotiated, timely Feasibility: practical, context, efficient Propriety: formal agreements, conflict of interest, transparency, inclusive Accuracy: valid, reliable, justified Accountability: documentation; internal & external metaevaluation Yarbrough, D. B., Shulha, L. M., Hopson, R. K., and Caruthers, F. A. The program evaluation standards: A guide for evaluators and evaluation users (3rd ed.). Thousand Oaks, CA: Sage; JH: This is a very brief summary of the AEA Evaluation Standards document and I don’t think we need to read every word. This is the skeleton of a 3-page document, which is on your thumb drives. The standards have been under revision for the past couple of years in committee and we are showing you this just to make the point that AEA evaluators continuously try to professionalize their evaluation practice, and hold practitioners to high standards of excellence. [One of the HELI participants asked about “standards.”]
. Thousand Oaks, CA: Sage; JH: This is a very brief summary of the AEA Evaluation Standards document and I don’t think we need to read every word. This is the skeleton of a 3-page document, which is on your thumb drives. The standards have been under revision for the past couple of years in committee and we are showing you this just to make the point that AEA evaluators continuously try to professionalize their evaluation practice, and hold practitioners to high standards of excellence. [One of the HELI participants asked about standards. ]")
31
Evaluation Address four evaluative questions:
How much have we been reaching out to the SEA communities? How much do the people in the community know about STEEP? How much have we made a difference in the SEA communities? How much have we made a difference to the people we educated?

32
How much have we been penetrating the SEA communities?
Conducted 65 events, delivered educational tools to 40,000 people in three target SEA locations: Twin Cities, Rochester, & St. Cloud. Recruited and trained over 120 volunteers; 20 of them delivered the education in their respective community. Networked/partnered with over 72 agencies and/or groups working on a variety of projects/activities in Minnesota. Recruited and trained 120 volunteers. Of the 120 trained volunteers, 20 had delivered the education using STEEP’s educational tools into their respective community. Networked and partnered with 72 agencies working on a variety of projects and activities in Minnesota. Engaged in several policy-related activities:

33
How much do the people in the community know about STEEP?
Nearly 97% of all survey respondents reported having seen STEEP at community events in the past year. More than 50% of the survey respondents indicated hearing people talking “quite often” about STEEP’s work in their communities within the past year ( ).
.")
34
How much have we made a difference in the SEA communities?

35
How much have we made a difference to the people we educated
How much have we made a difference to the people we educated? (Knowledge) Do you think smoking contributes to mouth cancers, poor vision, skin damage, ear ached. Now, think back to before you knew STEEP, would you say your answer to these questions (REPEAT) be (1) “the same now compared to before you knew STEEP,” ( 2) “a little different now compared to before you knew STEEP, or (3) “much different now compared to before you knew STEEP.”
 Do you think smoking contributes to mouth cancers, poor vision, skin damage, ear ached. Now, think back to before you knew STEEP, would you say your answer to these questions (REPEAT) be (1) the same now compared to before you knew STEEP, ( 2) a little different now compared to before you knew STEEP, or (3) much different now compared to before you knew STEEP.")
36
Graph 11. Rules about not smoking inside the home
How much have we made a difference to the people we educated? (Smoking norms inside the home) Graph 11. Rules about not smoking inside the home . Changing smoking norms inside the home
 Graph 11. Rules about not smoking inside the home. . Changing smoking norms inside the home.")
37
How much have we made a difference to the people we educated
How much have we made a difference to the people we educated? (see smoking now vs. a year ago in the community) In your observation, do you see smoking in the following places NOW compared to A YEAR AGO in your community? Please answer Yes or No to each place
 In your observation, do you see smoking in the following places NOW compared to A YEAR AGO in your community Please answer Yes or No to each place.")
38
How much have we made a difference to the people we educated
How much have we made a difference to the people we educated? (see smoking now vs. a year ago in the community)
")
39
References Bautista, R., Ednacot, E., & Wong, A. (2005, September). Asian Americans and Tobacco 101. An invitational workshop presented to the Minnesota Asian and Pacific Islanders Community, St. Paul, Minnesota. Blue Cross and Blue Shield of Minnesota, ClearWay Minnesota, Asian Pacific Tobacco Coalition of Minnesota, & Southeast Asian Refugee Community Home (2009). Tobacco use in Minnesota: A quantitative survey of Cambodian, Hmong, Lao, and Vietnamese community members. Minneapolis, MN: ClearWay Minnesota. Bostrom, R. P., Anson, R., & Clawson, V. K. (1993). Group facilitation and group support systems. Group Support Systems: New Perspectives, Brimmer, D. J., McCleary, K. K., Lupton, T. A., Faryna, K. M., Hynes, K., & Reeves, W. C. (2008). A train-the-trainer education and promotion program: Chronic fatigue syndrome--a diagnostic and management challenge. BMC Medical DREGAN (2010). Burcum, J. (2008, May 7th). Breathe deeply and ponder this anniversary. Star tribune. Retrieved from: opinion/commentary/ html?page=2&c=y Centers for Disease Control and Prevention (1999). Cigarette smoking among adults in the United States. MMWR, 48(43),
. Tobacco use in Minnesota: A quantitative survey of Cambodian, Hmong, Lao, and. Vietnamese community members. Minneapolis, MN: ClearWay Minnesota. Bostrom, R. P., Anson, R., & Clawson, V. K. (1993). Group facilitation and group support. systems. Group Support Systems: New Perspectives, Brimmer, D. J., McCleary, K. K., Lupton, T. A., Faryna, K. M., Hynes, K., & Reeves, W. C. (2008). A train-the-trainer education and promotion program: Chronic fatigue syndrome--a diagnostic and management challenge. BMC Medical DREGAN (2010). Burcum, J. (2008, May 7th). Breathe deeply and ponder this anniversary. Star tribune. Retrieved from: opinion/commentary/ html page=2&c=y. Centers for Disease Control and Prevention (1999). Cigarette smoking among adults in. the United States. MMWR, 48(43),")
40
References Centers for Disease Control and Prevention (CDCP). (2004). New surgeon general’s report expands list of diseases caused by smoking. Retrieved at from January 8, 2006 from Centers for Disease Control and Prevention (CDCP). (2007). Reducing youth exposure to tobacco Influences, Best Practices: For Comprehensive Tobacco Control Programs. U.S. Department of Health and Human Services. Chen, M. S. (2001). The status of tobacco cessation research for Asian Americans and Pacific Islanders. Asian American and Pacific Islander Journal of Health, 9(1), Council on Asian-Pacific Minnesotans and Minnesota Asian/American Health Coalition. (2009). Health Disparities: An Asian American & Pacific Islander Community Response. Diverse Racial Ethnic Groups and Nations (DREGAN). (2006). Tobacco Use in Minnesota: Perspectives from Cambodian, Hmong, Laotian, and Vietnamese Communities, Asian Pacific Tobacco-Free Coalition of Minnesota, Blue Cross and Blue Shield of Minnesota, Minnesota Partnership for Action Against Tobacco, Southeast Asian Refugee Community Home, March 2006. Doherty, W. J., & Carroll, J. S. (2002). The families and democracy project. Family Process, 41, 579–589.
. (2007). Reducing youth exposure to. tobacco Influences, Best Practices: For Comprehensive Tobacco Control. Programs. U.S. Department of Health and Human Services. Chen, M. S. (2001). The status of tobacco cessation research for Asian Americans and. Pacific Islanders. Asian American and Pacific Islander Journal of Health, 9(1), Council on Asian-Pacific Minnesotans and Minnesota Asian/American Health Coalition. (2009). Health Disparities: An Asian American & Pacific Islander Community Response. Diverse Racial Ethnic Groups and Nations (DREGAN). (2006). Tobacco Use in. Minnesota: Perspectives from Cambodian, Hmong, Laotian, and Vietnamese Communities, Asian Pacific Tobacco-Free Coalition of Minnesota, Blue Cross and Blue Shield of Minnesota, Minnesota Partnership for Action Against Tobacco, Southeast Asian Refugee Community Home, March Doherty, W. J., & Carroll, J. S. (2002). The families and democracy project. Family Process, 41, 579–589.")
41
References Doherty, W. J., & Mendenhall, T. J. (2006). Citizen health care: A model for engaging patients, families, and communities as co-producers of health. Families, Systems, & Health, 24(3), Eastman, T. Are Tobacco Companies Targeting Asian Americans? Retrieved from: Asian-Americans Giovino, G. A. , Chaloupka, F. J., Hartman, A. M. et al. (2009). Cigarette Smoking Prevalence and Policies in the 50 States: An Era of Change—The Robert Wood Johnson Foundation Impact Teen Tobacco Chart Book. Buffalo, NY: University at Buffalo, State University of New York. Granner, M. L., & Sharpe, P. A. (2004). Evaluating community coalition characteristics and functionality: A summary of measurement tools. Health Education Research, 19(5), Hoskins, L. & Angelica, E. (2005). Forming Alliances: Working together to achieve mutual goals. Fieldstone Alliance. Jenkins, C. N. H., McPhee, S. J., Bonilla, N-T, Nam, T. V., & Chen A. (1995). Cigarette smoking among Vietnamese immigrants in California. American Journal of Health Promotion, 9, Jenkins, C. N. H., McPhee, S. J., Le, A., Pham, G. Q., Ha, N., & Stewart, S. (1997). The effectiveness of a media-led intervention to reduce smoking among Vietnamese-American men. American Journal of Public Health, 87(6), Lam, T. C. & Bengo, P. (2003). A comparison of three retrospective self-reporting methods of measuring change in instructional practice. American Journal of Evaluation, 24(1),
, Eastman, T. Are Tobacco Companies Targeting Asian Americans Retrieved from: Asian-Americans. Giovino, G. A. , Chaloupka, F. J., Hartman, A. M. et al. (2009). Cigarette Smoking Prevalence and Policies in the 50 States: An Era of Change—The Robert Wood Johnson Foundation Impact Teen Tobacco Chart Book. Buffalo, NY: University at Buffalo, State University of New York. Granner, M. L., & Sharpe, P. A. (2004). Evaluating community coalition characteristics and. functionality: A summary of measurement tools. Health Education Research, 19(5), Hoskins, L. & Angelica, E. (2005). Forming Alliances: Working together to achieve mutual goals. Fieldstone Alliance. Jenkins, C. N. H., McPhee, S. J., Bonilla, N-T, Nam, T. V., & Chen A. (1995). Cigarette smoking among Vietnamese immigrants in California. American Journal of Health Promotion, 9, Jenkins, C. N. H., McPhee, S. J., Le, A., Pham, G. Q., Ha, N., & Stewart, S. (1997). The. effectiveness of a media-led intervention to reduce smoking among Vietnamese-American men. American Journal of Public Health, 87(6), Lam, T. C. & Bengo, P. (2003). A comparison of three retrospective self-reporting methods of. measuring change in instructional practice. American Journal of Evaluation, 24(1),")
42
References Lew, R., Honma, J., Portugal, C., & Baezconde-Garbanati, L. (2008). The final evaluation report: Assessing the impact of Leadership and Advocacy Institute to Advance Minnesota’s Parity for Priority Populations [LAAMPP]. Minneapolis, MN: ClearWay Minnesota. Linn, R. L., & Slinde, J.A. (Winter 1977). The determination of the significance of change between pre- and post-testing periods. Review of Educational Research, XLVII, Marcotty, J. (December 11, 2007). Statewide ban motivating Minnesota smokers to quit. Star Tribune. Retrieved from: health/ html McPhee, S. J., Jenkins, C. N. H., Wong, C., et al. (1995). Smoking cessation intervention among Vietnamese Americans: A controlled trial. Tobacco Control, 4, Minnesota State Demographer Center (n.d.). Immigrants in Minnesota. Retrieved from January 8, 2006 at Orfaly, R. A., Frances, J. C., Campbell, P., Whittemore, B., Joly, B., & Koh, H. (2005). Train-the-trainer as an educational model in public health preparedness. Journal of Public Health Management and Practice, 11(6), S Pratt, C. C., McGuigan, W. M., & Katzev, A. R. (2000) Measuring program outcomes: Using retrospective pretest methodology. American Journal of Evaluation, 21(3), Eberle, Hogle, & Peterson (2011, June). Program evaluation and healthy equity research. Workshop presented to the 2nd Annual Health Equity & Leadership Institute (HELI), University of Wisconsin-Madison.
. The determination of the significance of change. between pre- and post-testing periods. Review of Educational Research, XLVII, Marcotty, J. (December 11, 2007). Statewide ban motivating Minnesota smokers to quit. Star. Tribune. Retrieved from: health/ html. McPhee, S. J., Jenkins, C. N. H., Wong, C., et al. (1995). Smoking cessation intervention. among Vietnamese Americans: A controlled trial. Tobacco Control, 4, Minnesota State Demographer Center (n.d.). Immigrants in Minnesota. Retrieved from. January 8, 2006 at Orfaly, R. A., Frances, J. C., Campbell, P., Whittemore, B., Joly, B., & Koh, H. (2005). Train-the-trainer as an educational model in public health preparedness. Journal of Public Health Management and Practice, 11(6), S Pratt, C. C., McGuigan, W. M., & Katzev, A. R. (2000) Measuring program outcomes: Using retrospective pretest methodology. American Journal of Evaluation, 21(3), Eberle, Hogle, & Peterson (2011, June). Program evaluation and healthy equity research. Workshop presented to the 2nd Annual Health Equity & Leadership Institute (HELI), University of Wisconsin-Madison.")
43
References Rumbaut, R. G. (1989). Portraits, patterns, and predictors of the refugee adaptation process: Results and reflections from the IHARP panel study. In D. W. Haines (Ed.), Refugees as immigrants: Cambodians, Laotians, and Vietnamese in America. Totowa, NJ: Rowman & Littlefield Publishers, Inc. Sellnow, G. (2008, March 1st). Bar patrons light up under “Freedom to Breath Act,” Rochester (MN) Post-Bulletin. Retrieved from: newsmanager/templates/localnews_story.asp Tobacco Law Center. (2009). Tracking tobacco laws: A Minnesota Digest, 2nd ed., Tobacco Law Center, St Paul, MN. U.S. Department of Health and Human Services.(2007). Best Practices: For Comprehensive Tobacco Control Programs. U.S. Department of Health and Human Services, Centers for Disease Control and Prevention. Xiong, Z. B., Tuicomepee, A., LaBlanc, L., & Rainey, J. (2006). Hmong immigrants’ perceptions of family secrets and recipients of disclosure. Families in Society: The Journal of Contemporary Social Services, 87(2), Yee, B. Health and health care of Southeast Asian American elders: Vietnamese, Cambodian, Hmong, and Laotian elders. University of Texas Medical Branch, Galveston. Retrieved from:
, Refugees as. immigrants: Cambodians, Laotians, and Vietnamese in America. Totowa, NJ: Rowman & Littlefield Publishers, Inc. Sellnow, G. (2008, March 1st). Bar patrons light up under Freedom to Breath Act, Rochester. (MN) Post-Bulletin. Retrieved from: newsmanager/templates/localnews_story.asp. Tobacco Law Center. (2009). Tracking tobacco laws: A Minnesota Digest, 2nd ed., Tobacco Law. Center, St Paul, MN. U.S. Department of Health and Human Services.(2007). Best Practices: For Comprehensive. Tobacco Control Programs. U.S. Department of Health and Human Services, Centers for. Disease Control and Prevention. Xiong, Z. B., Tuicomepee, A., LaBlanc, L., & Rainey, J. (2006). Hmong immigrants’ perceptions of family secrets and recipients of disclosure. Families in Society: The Journal of. Contemporary Social Services, 87(2), Yee, B. Health and health care of Southeast Asian American elders: Vietnamese, Cambodian, Hmong, and Laotian elders. University of Texas Medical Branch, Galveston. Retrieved from:")
Similar presentations


![[Imagine School at North Port] Oral Exit Report Quality Assurance Review Team School Accreditation.](/1/271987/big_thumb.jpg "[Imagine School at North Port] Oral Exit Report Quality Assurance Review Team School Accreditation.>")




215-5297>")






 Turning Information Into Health.>")

 The Massachusetts Child Care Resource & Referral.>")


