Download presentation
Presentation is loading. Please wait.

1
Treatment approaches in the addiction field Professor John Strang National Addiction Centre, London, UK 2MMF conference Palermo, September 2008

2
declaration F * DH, NTA, Home Office, NACD, WHO, UNODC F * Diamo, Reckitt-Benkiser, Schering-Plough, Genus- Britannia, GW, Napp, Titan, Catalent, Auralis F * Phoenix House, Clouds House, Action on Addiction, Society for the Study of Addiction

3
NHS University

4
Development and pilot testing of new Prevention and Treatment Interventions Research into the causes, consequences and influences upon Addictions Policy analysis and input into Policy formation

5
Structure of todays talk F Some initial thoughts F Old wine in old bottles F Old wine in new bottles F New wine, well worth drinking F Wine still in development

6
Structure of todays talk F Some initial thoughts F Old wine in old bottles F Old wine in new bottles F New wine, well worth drinking F Wine still in development

7
… from Faith to Science …

8
How do we define drug? les drogues sont des substances qui provoquent des comportements irrationnels et deliriants ….. …chez ceux qui nen prennent jamais. (Timothy Leary) Opiate, stimulant, hallucinogen, sedative, alcohol, nicotine
 Opiate, stimulant, hallucinogen, sedative, alcohol, nicotine.")
9
Outcome measures OutcomeMeasures Drug use UDS & self-report ((Treatment retention)) Clinic records (& self report) Injecting practices Frequency, risk & complications Psychosocial functioning & Quality of Life Measures SF-36, EQ-5D, OTI ((Crime)) Self-report (drug related expenditure & criminal activity) ((Cost effectiveness)) Service costs (internal & external) ((Community Impact Evaluation)) Nuisance issues for local community
) Clinic records (& self report) Injecting practices Frequency, risk & complications Psychosocial functioning & Quality of Life Measures SF-36, EQ-5D, OTI ((Crime)) Self-report (drug related expenditure & criminal activity) ((Cost effectiveness)) Service costs (internal & external) ((Community Impact Evaluation)) Nuisance issues for local community")
10
benefit matrix HealthSocialEconomic Individual Community Societal

11
Which harms and benefits are the most important? F Scientist must measure F Society must assign weightings

12
Structure of todays talk F Some initial thoughts F Old wine in old bottles F Old wine in new bottles F New wine, well worth drinking F Wine still in development

13
Old wine in old bottles F MMT (and, more recently, BMT) F … but …
 F … but …")
14
(a) Methadone maintenance Major treatment for heroin dependence: highly effective 40 years of experience Oral, long half-life (daily), cross-tolerant: prevents withdrawal symptoms universal anodyne psychological effect To some extent it blocks euphoric effects of heroin Reduces illicit heroin use more than no treatment (USA, Australia), drug-free treatment (Sweden), placebo (Hong Kong, USA) and detoxification (Thailand, USA) in RCTs Better retention than placebo, drug-free treatment, detoxification and wait-list controls (Mattick, 2002)
 Methadone maintenance Major treatment for heroin dependence: highly effective 40 years of experience Oral, long half-life (daily), cross-tolerant: prevents withdrawal symptoms universal anodyne psychological effect To some extent it blocks euphoric effects of heroin Reduces illicit heroin use more than no treatment (USA, Australia), drug-free treatment (Sweden), placebo (Hong Kong, USA) and detoxification (Thailand, USA) in RCTs Better retention than placebo, drug-free treatment, detoxification and wait-list controls (Mattick, 2002)")
15
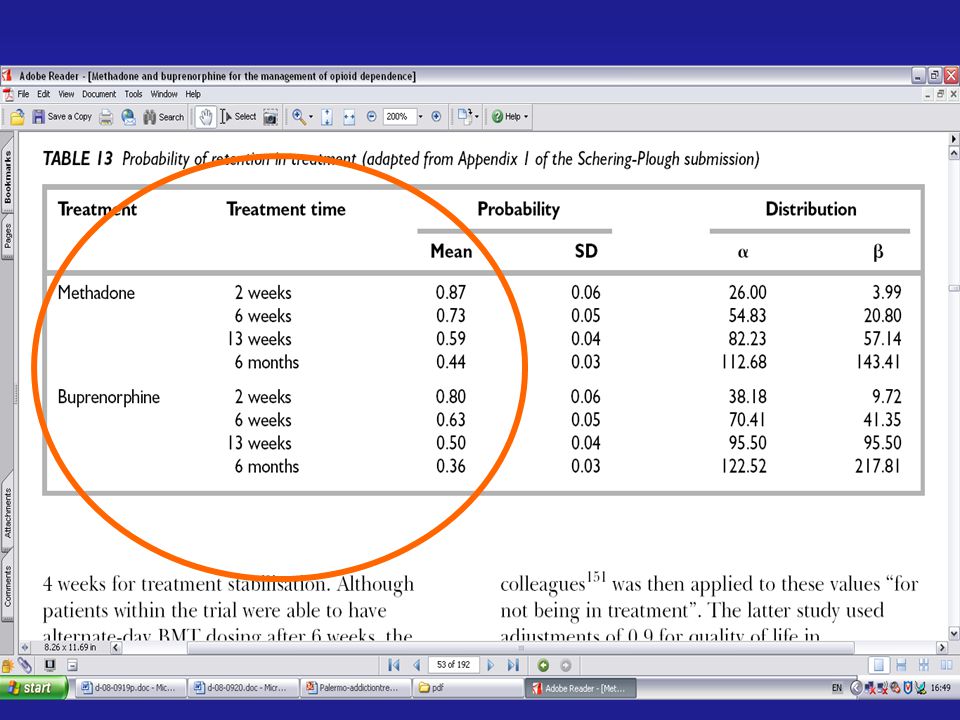
Evidence and interpretation: Clinical effectiveness F Most trials used a fixed-dose design 3MTD 50-150mg/day 3BP 1-15mg/day F 2 main outcomes reported: 3Retention in treatment 3Illicit use of opioids [proportion of people taking illicit opioids, mean rate of heroin intake assessed by self- report and/or urinalysis]
![Evidence and interpretation: Clinical effectiveness F Most trials used a fixed-dose design 3MTD mg/day 3BP 1-15mg/day F 2 main outcomes reported: 3Retention in treatment 3Illicit use of opioids [proportion of people taking illicit opioids, mean rate of heroin intake assessed by self- report and/or urinalysis]](http://images.slideplayer.com/4/1472359/slides/slide_15.jpg "Evidence and interpretation: Clinical effectiveness F Most trials used a fixed-dose design 3MTD mg/day 3BP 1-15mg/day F 2 main outcomes reported: 3Retention in treatment 3Illicit use of opioids [proportion of people taking illicit opioids, mean rate of heroin intake assessed by self- report and/or urinalysis]")
16
Gunne & Gronbladh (1981) RCT: Methadone versus no methadone 34 subjects using heroin by injection 17 experimental (methadone) 17 controls (no methadone) Controls not allowed to enter MMT for 2 years Followed up at 2 years and again at 4 years
 RCT: Methadone versus no methadone 34 subjects using heroin by injection 17 experimental (methadone) 17 controls (no methadone) Controls not allowed to enter MMT for 2 years Followed up at 2 years and again at 4 years")
17
Gunne & Gronbladh (1981): Baseline Experimental Group (methadone) Control group (no methadone) UUUUUUUU UUUUUUUU UUUUUUUU UUUUUUUU UU U – ongoing daily heroin Use
: Baseline Experimental Group (methadone) Control group (no methadone) UUUUUUUU UUUUUUUU UUUUUUUU UUUUUUUU UU U – ongoing daily heroin Use")
18
Gunne & Gronbladh (1981): 2 years Experimental group (methadone) Control group (no methadone) UUUA UUUU UUUU UUUD D A – Abstinent U – on-going daily Use D – Deceased
: 2 years Experimental group (methadone) Control group (no methadone) UUUA UUUU UUUU UUUD D A – Abstinent U – on-going daily Use D – Deceased")
19
Gunne & Gronbladh (1981): 2 years Experimental group (methadone) Control group (no methadone) AAAAUUUA AAAAUUUU AAAAUUUU UUUUUUUD UD A – Abstinent U – on-going daily Use D – Deceased
: 2 years Experimental group (methadone) Control group (no methadone) AAAAUUUA AAAAUUUU AAAAUUUU UUUUUUUD UD A – Abstinent U – on-going daily Use D – Deceased")
20
Gunne & Gronbladh (1981): 4 years Experimental Group (methadone) Control group (methadone) Control group (no methadone) UA UU UD DD D A – Abstinent U – on-going daily Use D – Deceased
: 4 years Experimental Group (methadone) Control group (methadone) Control group (no methadone) UA UU UD DD D A – Abstinent U – on-going daily Use D – Deceased")
21
Gunne & Gronbladh (1981): 4 years Experimental Group (methadone) Control group (methadone) Control group (no methadone) AAAAUA AAAAUU AAAAUD UUUADD UD A – Abstinent U – on-going daily Use D – Deceased
: 4 years Experimental Group (methadone) Control group (methadone) Control group (no methadone) AAAAUA AAAAUU AAAAUD UUUADD UD A – Abstinent U – on-going daily Use D – Deceased")
22
Gunne & Gronbladh (1981): 4 years Experimental Group (methadone) Control group (methadone) Control group (no methadone) AAAAUUUA AAAAAAUU AAAAAAUD UUUAAADD UD A – Abstinent U – on-going daily Use D – Deceased
: 4 years Experimental Group (methadone) Control group (methadone) Control group (no methadone) AAAAUUUA AAAAAAUU AAAAAAUD UUUAAADD UD A – Abstinent U – on-going daily Use D – Deceased")
23
% of DATOS Sample (N=727) USA - Outpatient Methadone Treatment Changes from Before to After Treatment *p<.001 Hubbard, Craddock, Flynn, Anderson, & Etheridge 1997, PAB
 USA - Outpatient Methadone Treatment Changes from Before to After Treatment *p<.001 Hubbard, Craddock, Flynn, Anderson, & Etheridge 1997, PAB")
24
% of DATOS Sample (N=727) USA - Outpatient Methadone Treatment Changes from Before to After Treatment *p<.001 Hubbard, Craddock, Flynn, Anderson, & Etheridge 1997, PAB
 USA - Outpatient Methadone Treatment Changes from Before to After Treatment *p<.001 Hubbard, Craddock, Flynn, Anderson, & Etheridge 1997, PAB")
25
% of DATOS Sample (N=727) USA - Outpatient Methadone Treatment Changes from Before to After Treatment *p<.001 Hubbard, Craddock, Flynn, Anderson, & Etheridge 1997, PAB
 USA - Outpatient Methadone Treatment Changes from Before to After Treatment *p<.001 Hubbard, Craddock, Flynn, Anderson, & Etheridge 1997, PAB")
26
The benefit of retaining patients in treatment - HIV infection rates in and out of methadone maintenance treatment (Metzger et al. 1993) Out of tx % In tx %
 Out of tx % In tx %.")
27
The benefit of retaining patients in treatment - HIV infection rates in and out of methadone maintenance treatment (Metzger et al. 1993) Out of tx % In tx %
 Out of tx % In tx %.")
28
The benefit of retaining patients in treatment - HIV infection rates in and out of methadone maintenance treatment (Metzger et al. 1993) Out of tx % In tx %
 Out of tx % In tx %.")
29
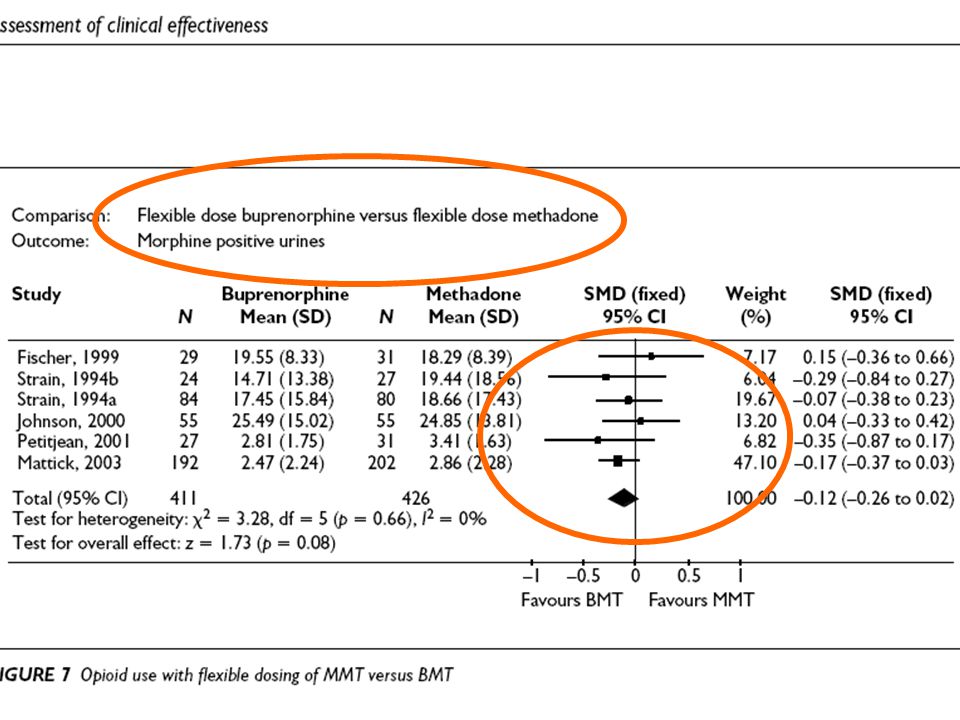
(b) Buprenorphine maintenance Agonist with very high affinity for opiate receptor (heroin cannot compete at opioid receptor) Similar treatment retention as methadone, but not quite as good (MMT: 63%, Bup:53%; Mattick, 2002) No significant difference between methadone and buprenorphine in reducing heroin use, cocaine use, benzodiazepine use or crime (Mattick, 2002) Probably less overdose risk (but not yet firmly demonstrated how much better)
 Buprenorphine maintenance Agonist with very high affinity for opiate receptor (heroin cannot compete at opioid receptor) Similar treatment retention as methadone, but not quite as good (MMT: 63%, Bup:53%; Mattick, 2002) No significant difference between methadone and buprenorphine in reducing heroin use, cocaine use, benzodiazepine use or crime (Mattick, 2002) Probably less overdose risk (but not yet firmly demonstrated how much better)")
32
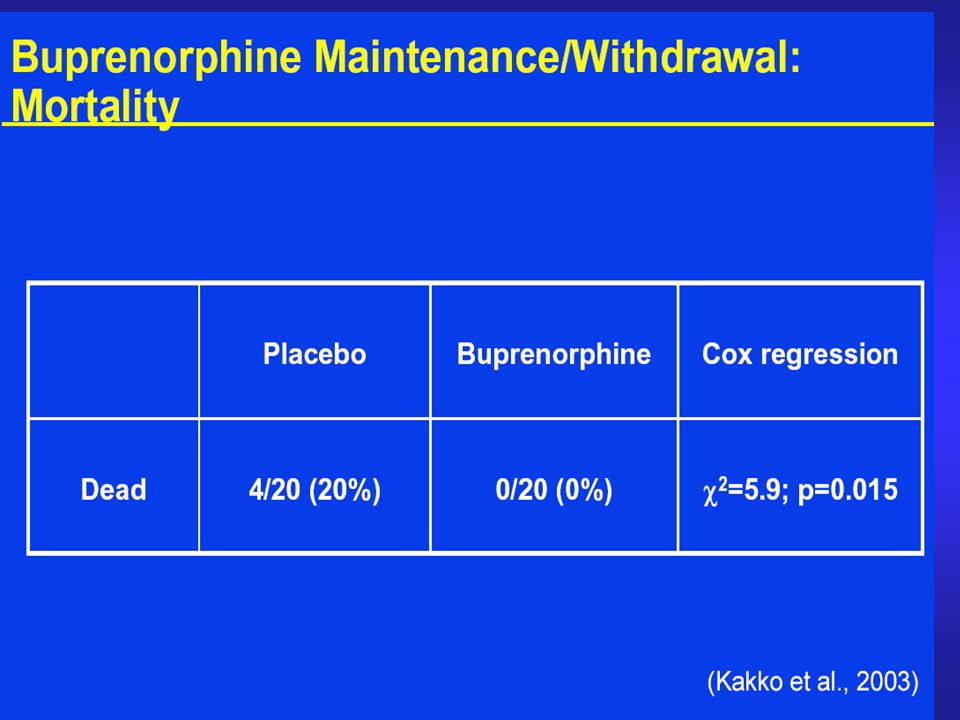
1 year retention during buprenorphine maintenance (16 mg qd) Kakko et al. (2003) Treatment duration (days) # Remaining in treatment 0 5 10 15 20 050100150200250300350 Control (6 day taper) buprenorphine maintained 75% retained at 1 year; no deaths 75% of urine drug screens negative
 Treatment duration (days) # Remaining in treatment Control (6 day taper) buprenorphine maintained 75% retained at 1 year; no deaths 75% of urine drug screens negative.")
34
012481632 10 11 12 13 14 15 16 17 Breaths/Minute PLBuprenorphine (mg, sl) Human respiratory rate Adapted from Walsh et al., 1994 Ceiling effect on respiratory depression
 Human respiratory rate Adapted from Walsh et al., 1994 Ceiling effect on respiratory depression")
45
(c) Levo-alpha-acetylmethadol (LAAM) Full opiate agonist with longer duration of action than methadone (48 or 72 hours or longer), 3x week dosing 10 cases of life threatening cardiac arrhythmias: withdrawn (Europe) and not be used as first line therapy (US) Need to clarify risks of LAAM treatment, particularly cardiac arrhythmia from QT prolongation
 Levo-alpha-acetylmethadol (LAAM) Full opiate agonist with longer duration of action than methadone (48 or 72 hours or longer), 3x week dosing 10 cases of life threatening cardiac arrhythmias: withdrawn (Europe) and not be used as first line therapy (US) Need to clarify risks of LAAM treatment, particularly cardiac arrhythmia from QT prolongation")
46
Retention in treatment: methadone, buprenorphine, LAAM maintenance

47
(d) Prolonged-release oral morphine F Oral, long duration of action (24 hours) F comparable retention and illicit drug use to methadone treatment and significantly lower depression, anxiety and physical complaints (Eder, 2005) F An open label 3-week study of 110 opioid dependent subjects showed high retention, reduced somatic complaints and reduced cravings (Kraigher, 2005) F MMT patients transferring to SROM (n=18) showed similar outcomes as methadone, improved social functioning, and less side-effects (Mitchell, 2004)
 Prolonged-release oral morphine F Oral, long duration of action (24 hours) F comparable retention and illicit drug use to methadone treatment and significantly lower depression, anxiety and physical complaints (Eder, 2005) F An open label 3-week study of 110 opioid dependent subjects showed high retention, reduced somatic complaints and reduced cravings (Kraigher, 2005) F MMT patients transferring to SROM (n=18) showed similar outcomes as methadone, improved social functioning, and less side-effects (Mitchell, 2004)")
48
(e) Codeine or dihydrocodeine
 Codeine or dihydrocodeine")
50
Naltrexone – the classic antagonist Opioid antagonist – oral, 24-hour, remarkably effective However - only rarely prescribed by doctors Widespread disappointment of poor uptake by patients Also - separately used (unlicensed) in opiate detox Also - long-acting depot form recently developed (2006) Separate alcohol interest in relapse-preventing benefit (perhaps ?? anti-craving effect for alcohol??)
.")
51
F … but …

52
Retention in treatment: methadone, buprenorphine, LAAM maintenance

53
Retention in treatment methadone, buprenorphine & LAAM vs. naltrexone

54
F Move to NICE slides

56
U.K. Methadone treatment: benefits in the first month (Strang, Finch et al, Addiction Research)
")
58
U.K. Methadone maintenance – changes in heroin use over time Source: Finch 2000 MD thesis

59
U.K. Methadone maintenance – changes in heroin use over time Source: Finch 2000 MD thesis

61
Opioid Overdose Deaths 1964-1997 (per million Australian adults, 15-44 years) (Hall, Degenhardt & Lynskey, 1999)
 (Hall, Degenhardt & Lynskey, 1999)")
62
Structure of todays talk F Some initial thoughts F Old wine in old bottles F Old wine in new bottles F New wine, well worth drinking F Wine still in development

63
Old wine in new bottles F (Naltrexone in alcohol field) F (Disulfiram with cocaine) F Heroin maintenance (re-conceptualisation) F Naloxone technology transfer
 F (Disulfiram with cocaine) F Heroin maintenance (re-conceptualisation) F Naloxone technology transfer")
69
WHAT INJECTABLE PRODUCTS? F Two products: F -heroin ampoules (dry amps) (1%) -methadone ampoules (wet amps) (3-10%)
 (1%) -methadone ampoules (wet amps) (3-10%).")
70
What is the RIOTT trial?

72
Results F …… to follow …… F However, as a clinician I can tell you … 3We are seeing some transformational changes 3Enough to guide policy-making process? 3Retention approx 85% at 6/12 (vs 50% typical) 3Follow-up approx 95% (vs 75% typical)
 3Follow-up approx 95% (vs 75% typical).")
76
Opioid Overdose Deaths 1964-1997 (per million Australian adults, 15-44 years) (Hall, Degenhardt & Lynskey, 1999)
 (Hall, Degenhardt & Lynskey, 1999)")
77
Oxygen saturation: IV versus IM

78
Oxygen saturation: case study

79
Actions on Discovering Overdose CALL AMBULANCE Check Airway – clear if blocked, Check breathing. If breathing, place in recovery position – if not breathing, begin basic life support or place in recovery position to maintain a good airway and prevent them from choking Administer naloxone

80
Naloxone Administration F Quickest route of injection is intravenous F However INTRAMUSCULAR injection recommended as easier. F Inject into a muscle F Upper outer buttock, thigh area or upper arm. F Hold needle 90 degree above skin F Insert needle into muscle F Slowly and Steadily push plunger all the way down

81
Client confidence in administering naloxone

85
F Interviews in confidence (n=1009) F Face-to-face F Independent research staff F Enquiry about sexual and injecting behaviours F Now; recent past; distant past
 F Face-to-face F Independent research staff F Enquiry about sexual and injecting behaviours F Now; recent past; distant past")
86
Table 1. Persistence of drug use on imprisonment Ever used (n=557 out of 1009) Year before prison Month before prison Heroin (n=324)63% a (n=204) 52% (n=169) Cocaine (n=387) 72% (n=280) 54% (n=209) Amphetamines (n=417) 52% (n=216) 30% (n=125) a All percentages are calculated based on the numbers who have ever used
 Year before prison Month before prison Heroin (n=324)63% a (n=204) 52% (n=169) Cocaine (n=387) 72% (n=280) 54% (n=209) Amphetamines (n=417) 52% (n=216) 30% (n=125) a All percentages are calculated based on the numbers who have ever used.")
87
Table 1. Persistence of drug use on imprisonment Ever used (n=557 out of 1009) Year before prison Month before prison Heroin (n=324)63% a (n=204) 52% (n=169) Cocaine (n=387) 72% (n=280) 54% (n=209) Amphetamines (n=417) 52% (n=216) 30% (n=125) a All percentages are calculated based on the numbers who have ever used
 Year before prison Month before prison Heroin (n=324)63% a (n=204) 52% (n=169) Cocaine (n=387) 72% (n=280) 54% (n=209) Amphetamines (n=417) 52% (n=216) 30% (n=125) a All percentages are calculated based on the numbers who have ever used.")
88
Table 1. Persistence of drug use on imprisonment Ever usedYear before prison Month before prison First month in prison Ever used it in prison Ever injected it in prison Amphetamines (n=417) 52% (n=216) 30% (n=125) 5% (n=19) 26% (n=108) 4% (n=15) a All percentages are calculated based on the numbers who have ever used
 52% (n=216) 30% (n=125) 5% (n=19) 26% (n=108) 4% (n=15) a All percentages are calculated based on the numbers who have ever used.")
89
Table 1. Persistence of drug use on imprisonment Ever usedYear before prison Month before prison First month in prison Ever used it in prison Ever injected it in prison Cocaine (n=387) 72% (n=280) 54% (n=209) 11% (n=41) 35% (n=135) 3% (n=10) Amphetamines (n=417) 52% (n=216) 30% (n=125) 5% (n=19) 26% (n=108) 4% (n=15) a All percentages are calculated based on the numbers who have ever used
 72% (n=280) 54% (n=209) 11% (n=41) 35% (n=135) 3% (n=10) Amphetamines (n=417) 52% (n=216) 30% (n=125) 5% (n=19) 26% (n=108) 4% (n=15) a All percentages are calculated based on the numbers who have ever used.")
90
Table 1. Persistence of drug use on imprisonment Ever usedYear before prison Month before prison First month in prison Ever used it in prison Ever injected it in prison Heroin (n=324)63% a (n=204) 52% (n=169) 36% (n=118) 71% (n=230) 16% (n=51) Cocaine (n=387) 72% (n=280) 54% (n=209) 11% (n=41) 35% (n=135) 3% (n=10) Amphetamines (n=417) 52% (n=216) 30% (n=125) 5% (n=19) 26% (n=108) 4% (n=15) a All percentages are calculated based on the numbers who have ever used
63% a (n=204) 52% (n=169) 36% (n=118) 71% (n=230) 16% (n=51) Cocaine (n=387) 72% (n=280) 54% (n=209) 11% (n=41) 35% (n=135) 3% (n=10) Amphetamines (n=417) 52% (n=216) 30% (n=125) 5% (n=19) 26% (n=108) 4% (n=15) a All percentages are calculated based on the numbers who have ever used.")
91
Post-release carnage F Seaman Brettle Gore, BMJ, 1998 F Bird & Hutchinson, Addiction, 2002 F Farrell & Marsden, Addiction, 2008

93
Prevalence of drug dependence Drug dependence prior to prison Substance Misuse in Prisoners 2002 Singleton N, Farrell M, Meltzer H ONS.

95
N-ALIVE trial – pilot & main phase F N-ALIVE research trial proposal to test/prove reduced deaths post-release F Pilot – n=5600 F Main study – n=56000 (28k + 28k)
")
96
Structure of todays talk F Some initial thoughts F Old wine in old bottles F Old wine in new bottles F New wine, well worth drinking F Wine still in development

97
Treatment Research Institute Mc Lellan et al Levels of Treatment in Methadone Maintenance Programs Random Assignment6 Months Bare-bones Standarddeluxe (n=29)(n=34)(n=36) Methadone: > 65mg>65mg>65mg Counseling:RegularRegular Other ServicesEmployment Family Therapy Psychiatric Care
(n=34)(n=36) Methadone: > 65mg>65mg>65mg Counseling:RegularRegular Other ServicesEmployment Family Therapy Psychiatric Care")
98
Levels of care Study Target behaviors at 6 months

99
Levels of care Study Target behaviors at 6 months

100
Levels of care Study Target behaviors at 6 months

102
F Move to NICE Forest plots of meta-analyses

103
Structure of todays talk F Some initial thoughts F Old wine in old bottles F Old wine in new bottles F New wine, well worth drinking F Wine still in development

104
Wines in development F (migrant medications) F Tele-prompting/monitoring F Vaccines F Ultra-long duration meds (nx; bup; …) F HR moderation medications (?nalmef; ?)
 F Tele-prompting/monitoring F Vaccines F Ultra-long duration meds (nx; bup; …) F HR moderation medications ( nalmef; )")
106
F … add cocaine vaccine slide …

113
conclusion F … exciting times

114
Thank you

115
Bup-nalox effects – by different routes (version 1)
")
118
BupNalox Sub-lingual BupNalox

119
BupNalox Inject BupNalox

Similar presentations
















































 Introduction to Harm Reduction Benefits of MMT One Patient’s Perspective Misconceptions.>")