Download presentation
Presentation is loading. Please wait.

1
Basic Needs and Comfort Measures

2
Objectives Define basic human needs
Define: self-actualization, self-esteem, love, security, belonging and physiologic needs according to Maslow’s Hierarchy of Needs Explain and list physiologic needs Define the terms associated with pain: agonist, analgesic, biofeedback, antagonist, relaxation, mediation, PCA endorphins Understand pain measurement techniques Describe techniques used to relieve pain Evaluate effectiveness of pain control measures

3
Objectives List causes of discomfort for patients
List nursing measures to promote comfort and ease discomfort for patients

4
Comfort and Discomfort
List some attributes associated with comfort: Examples: Warmth, softness, rest, quiet, coolness, cleanliness, space, safety Name some more that you associate with comfort

6
Comfort and Discomfort
List some attributes that you might associate with discomfort Examples: pain, nausea, fear, hunger, thirst, dark, worry List some other examples

7
Human Needs Basic human needs: those which are common to all people and essential for survival Some can be met independently; some are dependent on relationships with others Food, water, shelter, warmth Connection, love, security, spirituality

8
Abraham Maslow ( )
")
9
Maslow Professor of psychology at Brandeis University who founded humanistic psychology Created the Theory of Basic Human Needs Useful for understanding the relationships of basic human needs and for establishing priorities of care Theory of Basic Human Needs is a foundation for nursing care and interventions

10
Basic Human Needs have the following characteristics
The absence of a basic human need results in illness. The presence of basic human needs helps prevent illness or signals health. Meeting basic human needs restores health. It is preferred over other satisfactions when unmet One feels something missing when needs are unmet. One feels satisfaction when needs are met.

11
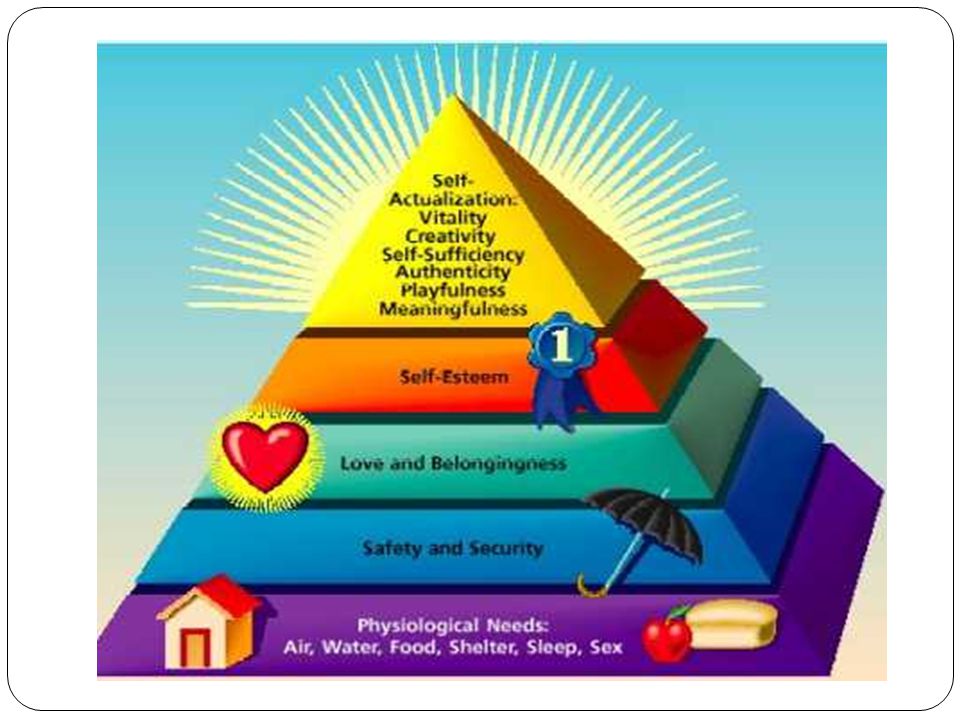
Maslow’s Hierarchy of Needs
Certain needs are more basic than others All people have the same needs all of the time, people generally strive to meet certain of their needs before attending to others Level 1: Physiologic needs Level 2: Safety and security needs Level 3: Love and belonging needs Level 4: self-esteem needs Level 5: Self-actualization needs

13
Basic Human Needs Level 1: Physiologic - oxygen, water, food, temperature, elimination, sexuality, physical activity and rest Most basic needs and have the highest priority Usually can be met through self-care, but many people who are ill require assistance Level 2: Safety and security - safe environment, protection from violence, safe emotional environment Level 3: Love and belonging needs - understanding and acceptance of others; belonging to a community

14
Basic Human Needs Level 4: Self-Esteem needs - need to feel pride and a sense of accomplishment, respect, appreciation Can be affected by body image, role changes Level 5: Self-Actualization needs - need to reach one’s own full potential

15
Level 1: Physiologic Needs
A need which must be met at least minimally to maintain life; the most basic in the hierarchy and therefore with the highest priority Most healthy children and adults can meet these needs through self-care Very young, old, disabled and ill people requires assistance in meeting them The lack of any of the following cause discomfort Oxygen: respiratory diseases, cardiac disease Water: dehydration, hypovolemia, Food: starvation, NPO Warmth

17
Level 2: Safety and security needs
Involves both physical and emotional components Physical security: Using hand hygiene and sterile techniques to prevent infection Using electrical equipment properly Administering medications knowledgeabley Using skill when moving and ambulating patients Assessing patients for potential risks, such as falling, bleeding, infection

19
Level 2: Safety and security needs
Emotional safety and security: being free from fear, anxiety and apprehension Patients entering health care system face fear of the unknown, their prognosis, unfamiliar surroundings, unfamiliar personnel All patients have anxiety Comfort measures: explain procedures, friendly, unhurried approach, continuity of caregivers, relationship building.

20
Level 3: Love and Belonging Needs
All humans have this need Called a higher-level need Includes understanding, acceptance and a feeling of belonging to families, peers, friends, community Nursing interventions to help meet this need: Including family and friends in the care of the patient Establishing a nurse-patient relationship based on mutual understanding and trust (by demonstrating caring, encouraging communication and respecting privacy)
")
22
Level 4: Self-Esteem Needs
Need for the person to feel good about him or her self, pride and a sense of accomplishment Factors which impact self-esteem: role changes, body-image changes as a result of illness, surgery Nursing interventions: respecting patients values and beliefs, encouraging patients to meet attainable goals

24
Level 5: Self-Actualization Needs
The need for individuals to reach their full potential through development of their unique capabilities In general, the lower level needs must be met before this need can be satisfied.

25
Self-Actualization Characterized by:
acceptance of self and others as they are focus of interest on problems outside oneself ability to be objective feelings of happiness and affection for others Respect for all people Ability to discriminate between good and evil Creativity in solving problems and pursuing interests

26
Nursing Process Assessment Diagnosis Planning Intervention Evaluation

27
Nursing Process Assessment: gathering information, data
Diagnosis: Name the problem Planning: State an achievable goal Interventions: Actions that work toward the stated goal Evaluation: Did the plan/interventions meet the stated goal

28
Nursing Interventions to Meet Patient Needs
Physiologic needs usually take priority Basic human needs are interrelated Examples: ER patient with an MI: Level 1 needs? Level 2 needs? Level 3,4,and 5 needs? Post-surgical patient in pain Pt. NPO for surgery

29
Question A nurse who focuses attention on the strengths and abilities of his patients rather than their problems is helping them to achieve which of Maslow’s basic human needs? A. Self-actualization B. Self-esteem C. Love and belonging D. Safety and security E. Physiologic

30
Answer Answer: A. Self-actualization Rationale:
To meet patient self-actualization needs, nurses provide a sense of direction and hope and maximize patient potential. Self-esteem needs are met by respecting patient values and beliefs and setting attainable goals for them. Love and belonging needs are met by including family and friends and establishing caring relationships with patients. Safety and security needs are met by encouraging spiritual practices and independent decision making. Physiologic needs are needs that must be met to maintain life.

31
Comfort and Discomfort
Physiologic Discomfort can come from: Pain Nausea and Vomiting Shortness of breath Hunger Thirst Inactivity Constipation

32
Comfort Measures - Pain

33
Pain Def: an unpleasant, subjective sensory and emotional experience associated with actual or potential tissue damage or described in terms of such damage It is a red flag indicating that something is wrong: “Protective in nature” Such an indicator of health that it is called the “5th Vital Sign”

34
Pain American Bar Association: Pain relief is a legal right
Therefore: Nurses are legally and ethically responsible for managing pain and suffering McCaffrey: “Pain is whatever the experiencing person says it is, existing whenever he says it is.”

35
Common Responses to Pain
Physiologic: increased BP, RR and pulse; pupil dilation, muscle tension, pallor; increased adrenalin, increased blood sugar Behavioral: moving away from painful stimuli, crying, moaning, restlessness Affective: withdrawal, stoicism, anxiety, depression, fear, anger, anorexia, fatigue, hopelessness, powerlessness

36
Categories of Pain Duration Location or source Mode of transmission
Etiology

37
Pain: Duration Acute pain: rapid in onset, varies in intensity from
mild to severe; warning signal that something is wrong (cut finger, sore throat, headache) Chronic pain: may be limited, intermittent or persistent, but lasts belong the normal healing period. Can be periods of remission or exacerbation. (cancer pain, back pain). Interferes with normal functioning
 Chronic pain: may be limited, intermittent or persistent, but lasts belong the normal healing. period. Can be periods of remission or exacerbation. (cancer pain, back pain). Interferes with normal functioning.")
38
Pain: Location or Source
Cutaneous Pain (superficial) usually involves the skin of subcutaneous tissue: paper cut Somatic Pain originates in tendons, ligaments, bones, blood vessels and nerves: sprains, broken bones Visceral pain is poorly localized and originates in body organs in the thorax, cranium, and abdomen: stomach pain
 usually involves the skin of subcutaneous tissue: paper cut. Somatic Pain originates in tendons, ligaments, bones, blood vessels and nerves: sprains, broken bones. Visceral pain is poorly localized and originates in body organs in the thorax, cranium, and abdomen: stomach pain.")
39
Question A patient who has bone cancer is most likely experiencing which of the following types of pain? A. Cutaneous B. Somatic C. Visceral D. Referred

40
Answer Answer: B. Somatic Rationale:
Deep somatic pain is diffuse or scattered and originates in tendons, ligaments, bones, blood vessels, and nerves. Cutaneous pain usually involves the skin or subcutaneous tissue. Visceral pain is poorly localized and originates in body organs. Referred pain is pain that originates in one part of the body and is perceived in an area distant to that part.

41
Origin of Pain Physical—cause of pain can be identified
Psychogenic—cause of pain cannot be identified Referred—pain is perceived in an area distant from its point of origin

42
Pain: Mode of transmission
Referred Pain: pain which is perceived in an area of the body distant from its point of origin Heart Attack or Myocardial Infarction: pain is felt in shoulder, jaw, or arms

43
Referred Pain

44
Pain: Etiology Neuropathic pain: pain resulting from an injury of or abnormal functioning of peripheral or central nervous system (fibromyalgia, peripheral neuropathy) Intractable: pain that is very resistant to treatment Phantom Pain: pain in an amputated limb
 Intractable: pain that is very resistant to treatment. Phantom Pain: pain in an amputated limb.")
45
Peripheral Neuropathy

46
Terms to know Agonist: a drug that binds with a receptor to produce a therapeutic response Analgesic: drug that relieves pain Antagonist: a drug that binds to a receptor to prevent the action of an agonist Placebo: “an inactive substance that gives satisfaction to the person using it” Nociceptors: Peripheral nerve fibers that transmit pain

47
The Pain Process Transduction—activation of pain receptors
Transmission—conduction along pathways (A-delta and C- delta fibers) Perception of pain—awareness of the characteristics of pain Modulation—inhibition or modification of pain
 Perception of pain—awareness of the characteristics of pain. Modulation—inhibition or modification of pain.")
48
Pain Process: Transduction, Transmission, Perception, Modulation

49
Stimulator of Nociceptors or Pain Receptors
Bradykinin: powerful vasodilator, trigger release of histamine (redness, swelling, inflammation) Prostaglandins: hormone-like substances that send additional pain stimuli to the CNS Substance P: sensitized receptors on nerves to feel pain These are Neurotransmitters: substances that excite or inhibit target nerve cells
 Prostaglandins: hormone-like substances that send additional pain stimuli to the CNS. Substance P: sensitized receptors on nerves to feel pain. These are Neurotransmitters: substances that excite or inhibit target nerve cells.")
50
Pain Reception

51
Pain Receptor Stimulators
Mechanical - friction Thermal - heat or cold Chemical - acid Electrical- static electricity

53
Perception of Pain Pain threshold: lowest intensity of a stimulus that is recognized as pain Adaptation: “getting used to the stimulus” Modulation of pain: sensation of pain is modified or lessened by naturally produced chemical substances Neuromodulators Endorphins, dynorphins, enkephalins

54
Gate Control Theory of Pain
States that certain small nerve fibers conduct pain impulses toward the brain Certain large nerve fibers appear to block pain impulses toward the brain A “gating mechanism” occurs when too much information is sent to the brain and the pain signal is interrupted The brain can influence its own gating mechanism through past experiences and learned behaviors

55
Gate Control Theory

56
Factors Affecting Pain Experience
Culture Ethnic variables Family, gender, and age variables Religious beliefs Environment and support people Anxiety and other stressors Past pain experience

57
General Assessments of Pain
Patient’s verbalization and description of pain Duration of pain Location of pain Quantity and intensity of pain Quality of pain Chronology of pain

59
Pain Scale

60
Symptom Analysis P, Q, R, S, T
P = Place: where is the pain (or other symptom)? Q= Quality: what does it feel like? R = Radiation: does it go anywhere else? S = Severity:how bad is it? Rate it on a 1-10 scale T = Time: how long have you had this?
 Q= Quality: what does it feel like R = Radiation: does it go anywhere else S = Severity:how bad is it Rate it on a 1-10 scale. T = Time: how long have you had this")
61
Nursing Interventions for Pain
Establishing trusting nurse–patient relationship Manipulating factors affecting pain experience Reviewing additional pain control measures Initiating nonpharmacologic and pharmacologic pain relief measures Considering ethical and legal responsibility to relieve pain Teaching patient about pain

62
Establishing a Relationship

63
Manipulating Factors Affecting Pain
Remove or alter the cause of pain: change body positions, empty distended bladder, loosen tight bindings Alter factors affecting pain tolerance: promote rest, sleep; encourage use of pain medication Initiate non-pharmacologic relief measures: distraction, humor, music, imagery, relaxation techniques, cutaneous stimulation (TENS unit), hypnosis, biofeedback, therapeutic touch
, hypnosis, biofeedback, therapeutic touch.")
64
Transcutaneous electrical nerve stimulation (TENS unit)
")
65
Pharmacologic Pain Relief Measures Selecting analgesics
Pharmacological – Analgesics Non-opiods – act on peripheral nerve ending at the injury site (Tylenol, NSAIDS) Opiods – Act on the CNS (Morphine, Codeine, Demerol; also synthetic opiods like Dilaudid) Adjuvants/Co-analgesics – Used in combination with opiods (benzodiazapines: Valium, Ativian)
 Opiods – Act on the CNS (Morphine, Codeine, Demerol; also synthetic opiods like Dilaudid) Adjuvants/Co-analgesics – Used in combination with opiods (benzodiazapines: Valium, Ativian)")
66
Selecting analgesics - WHO Ladder

67
Additional Methods for Administering Analgesics
Patient-controlled analgesia Epidural analgesia Local anesthesia

68
PCA pump: Patient Controlled Analgesia

69
PCA: Patient Controlled Analgesia

70
Placement of an Epidural Catheter

71
Scheduling Analgesic Doses
Preventive approach to pain management is crucial Nurses should be able to anticipate procedures and activities which will cause pain and pre-medicate the patient Pain should be controlled “ATC” or around the clock with long-acting medications and/or prn with “break-through” medications When pain is out of control, larger doses are required

72
Comfort Measures Provide quiet, clean, uncluttered environment
Provide warmth or coolness as indicated Provide personal hygiene: keep patient clean and dry, linen changes, oral care Provide activity as indicated: TV, radio, reading material Explain all procedures, tests, hospital routines Facilitate family visits and support Check with patient at regular intervals about his comfort/discomfort Keep call light within reach and encourage patient to call you if needed

73
Focus on the Patient

Similar presentations












>")













