Download presentation
Presentation is loading. Please wait.

1
Dermatology Update Katie Fiala, MD Department of Dermatology
Scott and White Memorial Hospital

2
TOPICS Varicella Zoster Psoriasis Acne Lipodermatosclerosis
Hemangiomas Melanoma Miscellaneous Updates

3
Varicella Zoster (Shingles)
Reactivation of chickenpox virus along sensory nerve causing a painful blistering skin eruption.

4
Clinical History 70 year old man Recent Hodgkins Disease dx Painful eruption on face Pain is excruciating Blisters erosions

5
Zoster

6
Varicella zoster 20% of healthy adults 50% adults > 85
Induced by stress, fever, XRT, trauma, immunosuppression Blacks 75% less likely Transmission via vesicular fluid 4% recurrence rate

8
Zoster: clinical features
Prodrome intense pain Itch, tingling, or hyperesthesia Grouped vesicles on erythematous base Umbilicated, pustular Sensory dermatome

9
Childhood Zoster Zoster in 5 year old

11
Diagnosis Confirmation
Viral Culture swab Viral PCR swab Aggressively swab base of lesion

12
Management / Treatment
Early treatment, within first 72 hours Oral anti-virals Acyclovir 800mg po 5x/day x 7-10 days Valacyclovir 1gm po TID x 7 days Famciclovir 500 mg po TID x 7 days $$ IV acyclovir - immunocompromised and disseminated form Acyclovir 10mg/kg IV q 8hrs x 7-10 days Oral prednisone (controversial)
")
13
DISSEMINATED ZOSTER >20 lesions outside of affected dermatome
Can cross midline 2 or more non-contiguous dermatomes May have internal involvement: hepatitis, encephalitis, pneumonitis

14
Post-herpetic Neuralgia
Post Zoster inflammation/injury to affected nerves More common >55 years of age Pain may last for months/year Rx: Narcotics, Neurotin (gabapentin), Nerve Block, topical lidocaine, topical gabapentin 6% Prevention?
, Nerve Block, topical lidocaine, topical gabapentin 6% Prevention")
15
Zostavax Reduced in incidence by 70% 50-59 Live attenuated vaccine
Reduced incidence by 55% in >60yo in a real-world practice (JAMA 2011;305;160-6) Effective in pts w/ underlying chronic conditions Reduced in incidence by 70% 50-59 Reduced incidence of PHN by 67% in >60yo Okay to receive if previous shingles Does prevent ophthalmic zoster
 Effective in pts w/ underlying chronic conditions. Reduced in incidence by 70% Reduced incidence of PHN by 67% in >60yo. Okay to receive if previous shingles. Does prevent ophthalmic zoster.")
16
Contraindications Anaphylaxis to gelatin or neomycin
Immunocompromised: HIV, chemo, chronic steroids, pregnancy, h/o leukemia or lymphoma

17
Psoriasis

22
Treatment Topical steroids Vitamin D analogs – calcipotriene
Phototherapy (Narrowband UVB) Methotrexate Cyclosporine Soriatane Biologics **NOT PREDNISONE**
 Methotrexate. Cyclosporine. Soriatane. Biologics. **NOT PREDNISONE**")
23
Psoriasis & Biologic Agents
Enbrel, Humira, Remicade (TNF-alpha inhibitors) Stelara (blocks IL-12 and IL-23) Screening: TB/HIV/Hepatitis prior TB yearly CBC/CMP prior and q6mo Contraindications: MS, Solid tumor, severe CHF Paradoxical Psoriasis (palmo-plantar)
 Stelara (blocks IL-12 and IL-23) Screening: TB/HIV/Hepatitis prior. TB yearly. CBC/CMP prior and q6mo. Contraindications: MS, Solid tumor, severe CHF. Paradoxical Psoriasis (palmo-plantar)")
24
Biologics and Infections
1 in 10 on biologics will have serious infection/year 10-18 fold increase on biologics Ways to help Be aware Tight control of DM Education Vaccines (live given b/f starting tx)
")
25
Psoriasis Associations
Obesity Hypercholesterolemia Hypertension Diabetes Mellitus II Depression Alcohol/Smoking Psoriatic Arthritis

26
Psoriasis & Metabolic Syndrome
Chronic inflammatory skin condition Pro-inflammatory cytokines Diabetes mellitus type II (OR=2.48), arterial hypertension (OR = 3.27), hyperlipidemia (OR = 2.09), and coronary heart disease (OR = 1.95). Increased prevalence of the metabolic syndrome in patients with moderate to severe psoriasis , Archives of Dermatological Research , Volume 298, Number 7, , 2006
, arterial hypertension (OR = 3.27), hyperlipidemia (OR = 2.09), and coronary heart disease (OR = 1.95). Increased prevalence of the metabolic syndrome in patients with moderate to severe psoriasis , Archives of Dermatological Research , Volume 298, Number 7, ,")
27
Psoriasis & Metabolic Syndrome
Metabolic syndrome more common in psoriatic patients than controls OR 1.65, >40 yo. Psoriatic patients - higher prevalence of hypertriglyceridemia and abdominal obesity Association independent from smoking. Conclusion: Psoriatic patients have a higher prevalence of metabolic syndrome, which can favor cardiovascular events. We suggest psoriatic patients should be encouraged to correct aggressively their modifiable cardiovascular risk factors Prevalence of metabolic syndrome in patients with psoriasis: a hospital-based case–control study, British Journal of Dermatology, Volume 157, Issue 1, pages 68–73, July 2007

28
Psoriasis and Cardiovascular Risk
Risk for MI 3.6 for controls, 4.0 for mild psoriasis, 5.1 for severe psoriasis Younger pts with severe psoriasis have the greatest risk of MI JAMA 2006;296:1735,41

29
Psoriatic Arthritis

30
Inverse Psoriasis

32
Inverse psoriasis +/- psoriasis elsewhere Treatment
Low-potency topical steroids Protopic (tacrolimus) 0.1% ointment or Elidel cream Minimize moisture, careful drying, drying powders (Zeosorb AF)
 0.1% ointment or Elidel cream. Minimize moisture, careful drying, drying powders (Zeosorb AF)")
33
LIPODERMATOSCLEROSIS
Sclerosing panniculitis Affects lower legs Secondary to chronic venous insufficiency 2/3 of patients are obese

34
Presentation ACUTE CHRONIC
Erythematous, painful, indurated plaques, swelling Can be unilateral or bilateral CHRONIC Less erythema, significant induration, hyperpigmentation, may ulcerate “inverted champagne bottle”

38
THERAPY Leg elevation Compression stockings
Potent topical steroids, under occlusion Aspirin NSAIDS Trental 400mg po TID Weight loss ? Vascular surgery

39
Hemangiomas Natural course Complications Proliferate by 9mo
Involute by 10yo 10% rule Complications Beard area Eye Diaper area

40
Know when to refer

41
(

42
Diffuse Cutaneous Hemangiomatosis
Liver Thyroid High Output Cardiac Failure

43
Treatment Especially if danger zones Prednisone 2-3mg /kg/ day
Propanolol 2-3 mg/ kg/day Very successful Risks: Hypotension, hypoglycemia Pediatric Cardiologist (Engl J Med 2008;358; )
")
44
ACNE

45
Topical therapy Non-comedogenic/ non-acnegenic
Topical retinoid – Differin, Retina, Retina Microgel, Tazorac Topical antibacterial – benzoyl peroxide, topical clindamycin, Benzaclin or Duac (BPO+ clinda) Azaelic Acid Topical Dapsone (Aczone)
 Azaelic Acid. Topical Dapsone (Aczone)")
46
Oral Therapy Minocycline 100mg bid Doxycycine 100mg bid
Clindamycin mg bid Bactrim DS bid **Azithromycin mg TIW Amoxicillin 500mg bid (pregnancy) **Spironolactone mg daily Oral contraceptives (Yasmin) Isotretinoin 1mg/kg bid x 5 -6 mo
 **Spironolactone mg daily. Oral contraceptives (Yasmin) Isotretinoin 1mg/kg bid x 5 -6 mo.")
47
Isotretinoin Other issues
Depression Labs: LFTs, lipids Pseudotumor cerebri: more likely with tetracyclines Xerosis and cheilitis Flare ? Inflammatory Bowel Disease

48
Inflammatory Bowel Crockett SD et al. Isotretinoin use and the risk of inflammatory bowel disease: A case–control study. Am J Gastroenterol 2010 Mar 30 8,189 pts with IBD and 21,832 controls 3664 Crohns & 4428 UC Isotretinoin use strongly associated with UC (OR 4.36) but not with Crohns Higher dosage and longer duration increased risk
 but not with Crohns. Higher dosage and longer duration increased risk.")
49
What does this mean? Pts must be made aware of risk
Stop if bowel symptoms develop until cleared by GI More studies needed ? Association with Tetracyclines

50
Melanoma Barriers to full skin exam Continues to be on the rise
Primary care: time constraints (54%) Dermatologists: patient embarrassment (44%) Arch Dermatol 2011;147:36-44 Continues to be on the rise One American dies of melanoma every hour
 Dermatologists: patient embarrassment (44%) Arch Dermatol 2011;147: Continues to be on the rise. One American dies of melanoma every hour.")
51
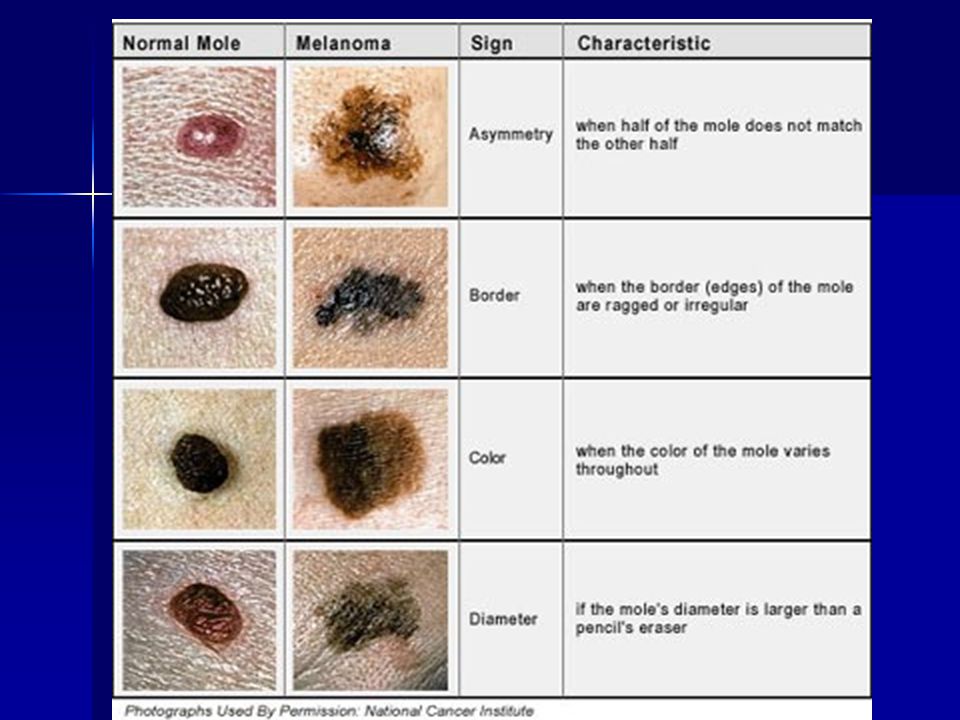
Melanoma Asymmetry Borders Color Diameter >6mm Evolution

54
Lentigo Maligna

55
SEER Age Adjusted Incidence Rates by Race and Sex Melanoma of the Skin, All Ages SEER 9 Registries for

56
Malignant Melanoma 75% of skin cancer deaths 1 American dies/ hour
25-29 yo Areas of intense, rare sun exposure Scalp = aggressive Also: eyes, mouth, genitalia

57
Who’s at Risk Red/blonde hair, blue/green eyes >50 nevi
Dysplastic nevi First degree relative H/o melanoma, 9x more likely Tanning bed Summer vacations >5 sunburns doubles risk Higher SES

58
IPILIMUMAB (Yervoy) FDA approved for metastatic melanoma
Monoclonal antibody (IV) Median overall survival 10.0 months (both), 10.1 (ipilimumab only) and 6.4 (vaccine only) N Engl J Med 2010;363;711-23
 Median overall survival 10.0 months (both), 10.1 (ipilimumab only) and 6.4 (vaccine only) N Engl J Med 2010;363;")
59
Vitamin D Debate Acknowledge benefits Encourage oral supplementation
Educate about sun protection Avoid peak hours 10am – 4pm Broad Spectrum (UVA/UVB) SPF 30, year round SPF 30 block 97-98% UVB Adequate amount Wet white shirt only SPF 4 Special clothing
 SPF 30, year round. SPF 30 block 97-98% UVB. Adequate amount. Wet white shirt only SPF 4. Special clothing.")
60
Miscellaneous New, COMB-FREE head lice treatment approved by FDA
Natroba Topical Suspension (spinosad 0.9%) Approved for children over 4yo Important not to use <6mo b/c contains benzoyl alcohol
 Approved for children over 4yo. Important not to use <6mo b/c contains benzoyl alcohol.")
61
Miscellaneous PDT for Actinic Keratoses Photodynamic Therapy
Metvixia (methyl amiolevulinate cream) applied to affected area approx 2 hours under occlusion Red light for 6-8 minutes Reaction similar to 5-FU in 1-2 days
 applied to affected area approx 2 hours under occlusion. Red light for 6-8 minutes. Reaction similar to 5-FU in 1-2 days.")
62
Miscellaneous BRACYTHERAPY Precise placement of radiation sources
Exposure to radiation of healthy tissues reduced Tumor can be treated w/ very high doses Applicator can conform to contour of face/skin Cure rates comparable to EBRT Can be completed in less time Less visits Less time for cancer cells to divide

63
Thank you!

Similar presentations
























 201-5414 Tuberculosis surveillance data for Minnesota are available on.>")





 in Children>")