Download presentation
Presentation is loading. Please wait.

1
Clival Chordoma Case in Pediatric Patient
Radiation Oncology Case with Pre-RT Images Clival Chordoma Case in Pediatric Patient •RT and IMRT slides courtesy of Paul Read, MD

2
Clival Chordoma – Overview
•Congenital tumors believed to originate from notochordal cell rests •Rare in childhood, more common in 3rd and 4th decades •Chordomas generally occur in 3 locations: the sacrum, the clivus, and along the spinal axis •For clival tumors, diplopia, headache, widening sutures, and enlarging head size are most common sx •About ½ patients have cranial nerve palsies (VI, V, III)
")
3
Clival Chordoma – Overview
•Male predominance in pediatric population for unclear reasons •10 month average time from the onset of sx to dx •Tumors usually large in size at dx with innocuous presenting sx •CT exam often reveals a midline soft tissue mass around the clivus associated with osteolytic bone destruction and intralesional calcifications. • MRI delineates the exact site and extension, but also defines neural and vascular relationship for planning surg • Location of these tumours proximal to vital neural and vascular structures makes surgical removal difficult and the ultimate clinical course malignant

4
Clival Chordoma – Overview
•Combination of a ‘radical debulking’ operation followed by high dose radiation therapy appears to be an effective mode of treatment in older children. •Chemotherapy appears to be of no value • Survival for 4‑11 years without recurrence is recorded in children under 10 years of age who received such a combination of treatment • The 5-year survival 51%, 10-year survival 35% • Good prognostic factors are young age, complete resection, and the addition of radiation therapy

5
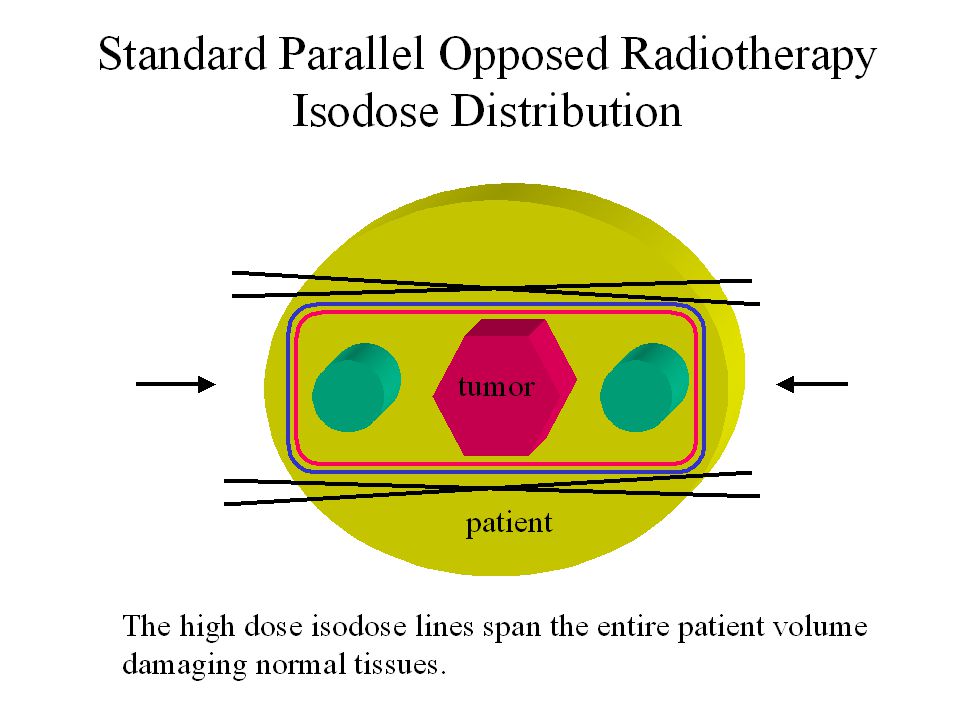
Clival Chordoma Case Pediatric patient with an extremely aggressive atypical chordoma that locally destroyed the clivus Tumor extension to brainstem, upper spinal cord, nasopharynx, cavernous sinus, retropharyngeal space, left parapharyngeal space Plan high dose RT to tumor (65-70 Gy) while respecting CNS tolerance
 while respecting CNS tolerance.")
20
ACR CODE: Presented by Tim Showalter, Class of 2004 Many of the RT and IMRT slides courtesy of Paul Read, MD of UVA Department of Radiation Oncology

Similar presentations













 Ass. Professor of Clinical Oncology Kasr El-Aini School of Medicine.>")
Primary Tumours: Benign Glomus tumour Malignant Carcinoma,sarcoma 2)Secondary Tumours: a) From adjacent areas like.>")








 H. Louis Harkey Department of Neurosurgery University of Mississippi Jackson, MS.>")






