Download presentation
Presentation is loading. Please wait.

1
Endovascular repair of mycotic aortic aneurysms
Wee Ming TAY, Zhiwen Joseph LO, Glenn Wei Leong TAN, Sriram NARAYANAN, Sadhana CHANDRASEKAR

2
Disclosure Speaker name: ......Tay Wee Ming I do not have any potential conflict of interest

3
Debridement followed by reconstruction
Open Surgery Debridement followed by reconstruction Complications with bypass – 20% aortic stump disruption, 30% amputation rate, 20% risk of re-infection Complications with in-situ aortic replacement – 8% mortality, 100% 5 year-limb-salvage , 22% graft re-infection rates Oderich et al; Infected aortic aneurysms: aggressive presentation, complicated early outcome, but durable results. J Vasc Surg 2001; 34:900-8) EVAR Avoidance of large incision, blood loss, revascularization, aortic clamping. Overall mortality 19% 60% in patients with primary mycotic aorto-enteric fistula 6% in patients without aorto-enteric fistula Kritpracha et al; Endovascular therapy for infected aortic aneurysms. J Vasc Surg 2011 ; 54:
 EVAR. Avoidance of large incision, blood loss, revascularization, aortic clamping. Overall mortality 19% 60% in patients with primary mycotic aorto-enteric fistula. 6% in patients without aorto-enteric fistula. Kritpracha et al; Endovascular therapy for infected aortic aneurysms. J Vasc Surg 2011 ; 54:")
4
Can they be managed by endovascular repair?
September 4, 2018 Endovascular repair of mycotic aneurysms : Can they be managed by endovascular repair? AIM: Evaluate characteristics and outcomes of patients with mycotic aortic aneurysms who underwent EVAR/TEVAR The EVRF system yields satisfactory clinical and anatomical midterm outcomes with very low complication rates However, contemporary studies of the radiofrequency-induced thermal therapy device (RFiTT®), show that in experienced hands, clinical equivalence to the Venefit™ procedure can be achieved. The evidence base for EVRF® and VeinCLEAR™ devices is currently weak and absent, respectively. Copyright UPM-Kymmene Group
, show that in experienced hands, clinical equivalence to the Venefit™ procedure can be achieved. The evidence base for EVRF® and VeinCLEAR™ devices is currently weak and absent, respectively. Copyright UPM-Kymmene Group.")
5
September 4, 2018 Methodology: Records of patients who underwent EVAR/TEVAR in the hospital were extracted from Aortic Aneurysm Database: Total of 271 EVAR/TEVAR performed from May 2008 to December 2015 14 Patients identified Diagnosis of mycotic aneurysm : Fever, abdominal pain CT aortogram findings Positive blood cultures VNUS Closurefast now Venefit? Copyright UPM-Kymmene Group

6
September 4, 2018 Formulated based on literature review Copyright UPM-Kymmene Group

7
Results Immunocompromised states :
September 4, 2018 Results Immunocompromised states : 64% had a comorbidity – Steroids, DM, HIV Similar to other studies (70%) Formulated based on literature review Oderich et al; Infected aortic aneurysms: aggressive presentation, complicated early outcome, but durable results. J Vasc Surg 2001; 34:900-8) Copyright UPM-Kymmene Group
 Formulated based on literature review. Oderich et al; Infected aortic aneurysms: aggressive presentation, complicated early outcome, but durable results. J Vasc Surg 2001; 34:900-8) Copyright UPM-Kymmene Group.")
8
Results: Salmonella Enteriditis (67%) was the most prevalent organism
Well known cause worldwide, tends to adhere to vascular endothelium, especially if atherosclerotic Known to have fast disease progression with early rupture Sorelius et al; Endovascular treatment of mycotic aortic aneurysms: A European multicenter study

9
Discussion: Antibiotics :
Once diagnosis suspected, IV antibiotics should be started, reasonable to perform course of antibiotics prior to surgery (2-4 weeks) If patient not impending rupture Extend for 12 weeks after excision and clearance of blood cultures Lopes et al. Infectious Thoracic Aortitis: A Literature Review. Clin.Cardio. 32,9, (2009)
 If patient not impending rupture. Extend for 12 weeks after excision and clearance of blood cultures. Lopes et al. Infectious Thoracic Aortitis: A Literature Review. Clin.Cardio. 32,9, (2009)")
10
Discussion: From our study:
Pre-op, most of our patients are placed on antibiotics with average of 19 days prior to surgery Sufficient for control of infection and sepsis All our patients are placed on life-long antibiotics Patients had smaller/no aneruysm by 3-6 month followup scans

11
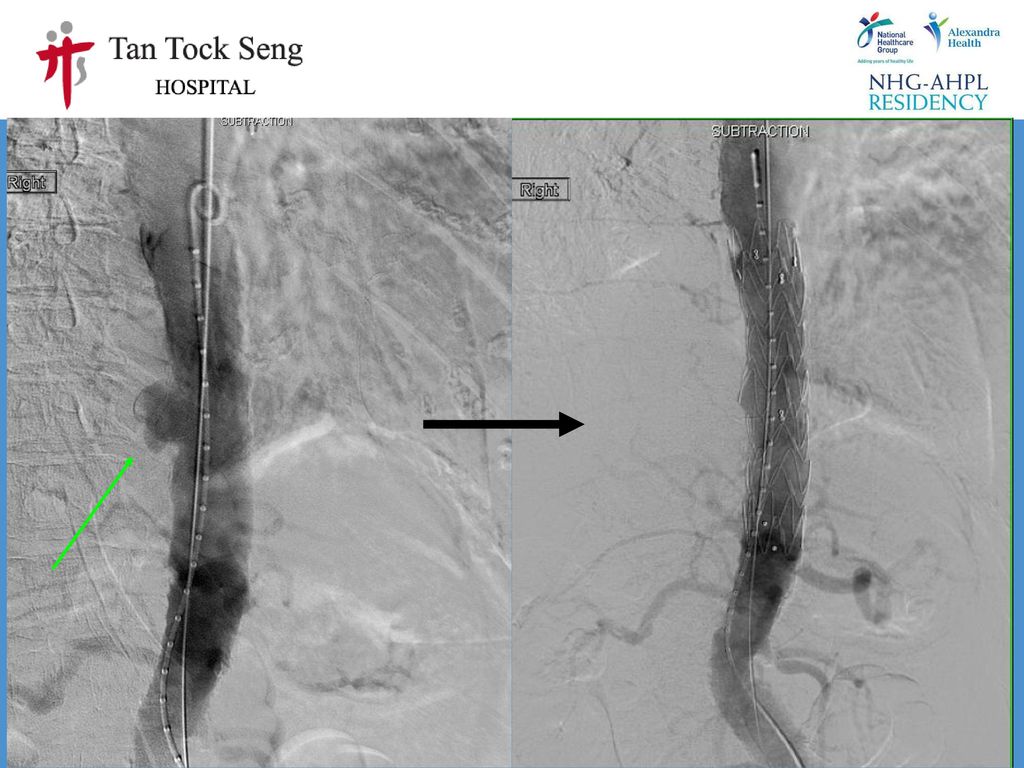
Salmonella bacteraemia
September 4, 2018 69/male Salmonella bacteraemia For asian population? Similar clinical outcomes? (But no CEAP comparison) Efficacy, safety similar; technical aspects advantageous in EVRF Copyright UPM-Kymmene Group 15
 Efficacy, safety similar; technical aspects advantageous in EVRF. Copyright UPM-Kymmene Group. 15.")
12
EVAR performed No endoleak Good renal perfusion

13
Repeat CT Aortogram: 2 months later No leak Resolution of stranding and inflammation

14
Results

15
Discussion: Our EVARs 2 cases of endoleak
First: Type 3B endoleak in abdominal aorta graft – repeat EVAR and subsequent re-lining Second: Type 1B/3 endoleak 1 year after initial EVAR. Complicated by aorto-esophageal fistula. Low Aneurysm-related mortality (1/14)
")
16
Patient #B MG (on prednisolone), old CVA Admitted for abdominal pain & Fever Blood cultures – Salmonella Enteritidis Saccular outpouching 1.8 X 1.2 cm

18
8 months later Re-admitted for dysphagia
CT Aortogram: Type 3 / 1b endoleak compressing on distal oesophagus Repeat CT Aortogram 2/12 post procedure: No leak

19
2 Grafts deployed Distal border (fix Type 1b)
Proximal border (fix Type 3) Good flow to celiacs, SMA, renal arteries Patients subsequently discharged well
 Good flow to celiacs, SMA, renal arteries. Patients subsequently discharged well.")
20
Re-admitted 1/12 later Back pain, fever CT aortogram: Increase in aneurysm Gas locules Type 1b leak

21
Endovascular repair done :
Celiac artery & SMA stented Good seal post angiogram check OGD done Likely aortoenteric fistula
22
September 4, 2018 Progress Initially in discussion with upper GI colleagues regarding stent of the esophagus Complicated by perforated gastric ulcer Underwent laparotomy and omental patch repair of ulcer Sepsis, bacteraemia Passed away a week later For asian population? Similar clinical outcomes? (But no CEAP comparison) Efficacy, safety similar; technical aspects advantageous in EVRF Copyright UPM-Kymmene Group 26
 Efficacy, safety similar; technical aspects advantageous in EVRF. Copyright UPM-Kymmene Group. 26.")
23
September 4, 2018 Conclusion Endovascular stent grafting feasible in management of mycotic aneurysm Fistulous aorto-enteric mycotic aneurysms poor prognosis Sepsis must be controlled by antibiotics post-surgery Satisfactory outcomes in this series For asian population? Similar clinical outcomes? (But no CEAP comparison) Efficacy, safety similar; technical aspects advantageous in EVRF Copyright UPM-Kymmene Group
 Efficacy, safety similar; technical aspects advantageous in EVRF. Copyright UPM-Kymmene Group.")
24
Questions

Similar presentations







 LECT7 ALI B ALHAILIY.>")









 +/- stenting in a subgroup of patients.>")

