Download presentation
Presentation is loading. Please wait.

1
ASCO Recap Palak Desai, MD

2
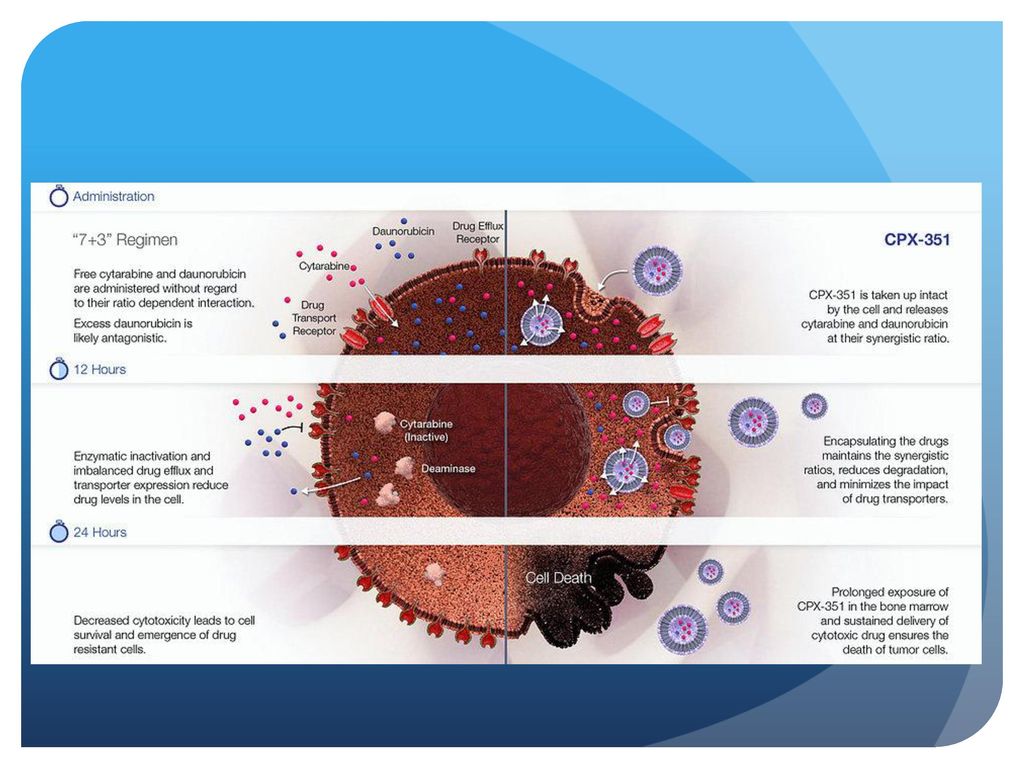
Secondary AML Older patients with secondary AML have poor outcomes following first-line cytarabine and anthracycline-based treatment. 7+3 is often the regimen of choice in patients with secondary AML

3
CPX-351 CPX-351 is a formulation of cytarabine and daunorubicin encapsulated at a 5:1 molar ratio within 100-nm diameter bilamellar liposomes. The specific ratio for inclusion was determined in laboratory testing that showed a molar ratio of 5:1 maximized synergy and minimized antagonism. Selective uptake of the encapsulated formulation by leukemic cells was confirmed in animal leukemia models

5
CPX-351- Study Design Patients years of age with untreated AML with a history of prior cytotoxic treatment, prior MDS or CMML (+/- prior hypomethylator treatment), or AML with WHO-defined MDS-related cytogenetic abnormalities were eligible. Patients were to be randomized 1:1 to CPX-351 (100 units/m2, days 1, 3, 5) or 7+3 (cytarabine 100 mg/m2/day x 7 days, daunorubicin 60 mg/m2 days 1, 2, 3) induction therapy. Primary endpoints overall (OS, 1o) and event free survival (EFS) assessed by stratified log rank analysis, independent blinded assessment of CR+CRi, and 60-day mortality
, or AML with WHO-defined MDS-related cytogenetic abnormalities were eligible. Patients were to be randomized 1:1 to CPX-351 (100 units/m2, days 1, 3, 5) or 7+3 (cytarabine 100 mg/m2/day x 7 days, daunorubicin 60 mg/m2 days 1, 2, 3) induction therapy. Primary endpoints overall (OS, 1o) and event free survival (EFS) assessed by stratified log rank analysis, independent blinded assessment of CR+CRi, and 60-day mortality.")
6
CPX-351- Results A total of 309 patients were randomized (153 to CPX to 7+3) and were well balanced for sex, race, age, performance status, AML-subtype, MDS-related cytogenetics and prior HMA therapy. After minimum follow-up of 13.7 months.
 and were well balanced for sex, race, age, performance status, AML-subtype, MDS-related cytogenetics and prior HMA therapy. After minimum follow-up of 13.7 months.")
7
CPX-351 Results OS was significantly improved with CPX-351, with a median OS of : 9.56 months in the CPX-351 arm 5.95 months in the 7+3 arm (hazard ratio [HR] 0.69; p = 0.005). There were also favorable benefits for the study drug compared to 7+3 for other efficacy endpoints, including event-free survival and response rate. The 60-day mortality rate was more favorable in the group receiving CPX-351 compared with the group treated with the 7+3 regimen (13.7% vs. 21.2%). Of the deaths that occurred within 60 days, 10.5% in the CPX-351 group were due to adverse events, with 3.3% attributable to progressive AML 9.9% of deaths in the 7+3 group were due to adverse events and 11.3% were attributable to progressive AML.
. There were also favorable benefits for the study drug compared to 7+3 for other efficacy endpoints, including event-free survival and response rate. The 60-day mortality rate was more favorable in the group receiving CPX-351 compared with the group treated with the 7+3 regimen (13.7% vs. 21.2%). Of the deaths that occurred within 60 days, 10.5% in the CPX-351 group were due to adverse events, with 3.3% attributable to progressive AML. 9.9% of deaths in the 7+3 group were due to adverse events and 11.3% were attributable to progressive AML.")
8
Transplant Patients Hematopoietic transplant was performed in 34% and 25% of patients in the CPX-351 and 7+3 arms, respectively. However, those patients in the CPX-351 arm who underwent transplant appeared to have more favorable outcomes. At the time of transplant, median OS in the CPX-351 arm had not yet been reached and was months in the 7+3 arm (HR 0.46; p = ). Grade 3 to 5 adverse events were similar in frequency and severity in both arms
. Grade 3 to 5 adverse events were similar in frequency and severity in both arms.")
9
CPX-351 The findings from the trial demonstrated a benefit for the liposomal, encapsulated drug delivery platform, even if the exact mechanism explaining superior outcomes are not well understood After 24 months of follow-up, 31.1% of patients in the CPX-351 treatment group were still alive compared with 12.3% in the 7+3 group. Could this data using liposomal delivery mechanisms be extrapolated to other combinations of chemotherapy drugs? CPX-351 could become the new standard of care for older patients with secondary AML.

11
Adjuvant Treatment

12
ESPAC-4 The ESPAC-3 trial compared adjuvant GEM with 5- fluorouracil/folinic acid for resected pancreatic cancer. GEM is the standard of care based on similar survival and less toxicity. ESPAC-4 aimed to determine whether combination chemotherapy with GEM/CAP improved survival compared to GEM monotherapy.

14
ESPAC-4 Patients with pancreatic ductal adenocarcinoma were randomized within 12 weeks of surgery (stratified for R0/R1 resection margin status and country) to have: six 4 week cycles of IV GEM alone GEM with oral CAP for 24 weeks The primary endpoint was overall survival; secondary endpoints were toxicity, relapse free survival, 2 and 5 year survival and quality of life.
 to have: six 4 week cycles of IV GEM alone. GEM with oral CAP for 24 weeks. The primary endpoint was overall survival; secondary endpoints were toxicity, relapse free survival, 2 and 5 year survival and quality of life.")
15
732 patients were randomized with 730 included in the full analysis set (366 GEM, 364 GEM/CAP).
Median age was 65 years, 57% were men. WHO performance status was 0, 1 or 2 in 42% 55% and 3% respectively. Postoperative median CA19-9 was 19 kU/L. Median maximum tumor size was 30 mm 60% were R1 resections 80% were node positive and 40% were poorly differentiated.

17
ESPAC-4 Results Median survival (months) for patients treated with GEM/CAP was: 28.0 (95% CI, 23.5 – 31.5) 25.5 (22.7 – 27.9) for GEM. HR=0.82 [95% CI, 0.68 – 0.98]; P=0.032.
 for GEM. HR=0.82 [95% CI, 0.68 – 0.98]; P=")
23
ESPAC-4 Adjuvant GEM/CAP for pancreatic cancer had a statistically significant improvement in survival compared to GEM monotherapy. The toxicities were manageable New standard of care for adjuvant therapy for pancreatic adenocarcinoma

25
Delta-Like Protein 3 (DLL3)
An atypical inhibitory Notch Ligand Induced by the key neuroendocrine transcription factor, ASCL-1 Aberrant cell surface expression in >80% of small cell lung and large cell neuroendocrine cancers On both cancer stem and tumor cells, but not normal adult tissues Not prognostic, and does not predict response to chemo

27
Patients with progressive SCLC after at least 1 previous systemic therapy were eligible.
Efficacy was assessed by the investigator via RECIST and toxicity when available, archived tumor tissue was assessed retrospectively for DLL3 expression by immunohistochemistry.

28
74 pts were enrolled at dose levels ranging from 0. 05 to 0
74 pts were enrolled at dose levels ranging from 0.05 to 0.8 mg/kg at either q3w or q6w. Among evaluable pts treated at doses of mg/kg, 15/61 (25%; 95% CI 15-37%) achieved a best response of PR or CR, and 44/61 (72%; 95% CI 59-83%) achieved clinical benefit (best response of at least SD).
 achieved a best response of PR or CR, and 44/61 (72%; 95% CI 59-83%) achieved clinical benefit (best response of at least SD).")
36
Conclusions Single-agent activity in recurrent/refractory SCLC
Comparable responses in second and third line Responses and survival improved vs. historical approved treatments First biomarker-directed therapy in SCLC Manageable safety profile Results justify further clinical development

Similar presentations





























>")
![Randomized Phase III Trial Comparing FOLFIRINOX (F: 5FU/Leucovorin [LV], Irinotecan [I], and Oxaliplatin [O]) versus Gemcitabine (G) as First-Line Treatment.](/34/8349925/big_thumb.jpg "Randomized Phase III Trial Comparing FOLFIRINOX (F: 5FU/Leucovorin [LV], Irinotecan [I], and Oxaliplatin [O]) versus Gemcitabine (G) as First-Line Treatment.>")

 Treated with Vosaroxin plus Cytarabine versus Placebo plus.>")

 Summary of Data as of December 16, 2004 Kevin Carroll, MSc Summary of Data.>")




