Download presentation
Presentation is loading. Please wait.

1
In the name of God In the name of God

2
Spontaneous preterm birth includes birth that follows preterm labor, preterm spontaneous rupture of membranes, and cervical insufficiency, but does not include indicated preterm delivery for maternal or fetal conditions

3
increased more than 20% from 1990 to 2006

4
The strongest clinical risk factors:
Maternal history of preterm birth is commonly reported to confer a 1.5-fold to 2-fold increased risk in a subsequent pregnancy. Importantly, the number of prior preterm births and the gestational age at the prior delivery significantly affect the recurrence risk of preterm birth .A preterm birth followed by delivery at term confers lower risk than the opposite.

5
Short cervical length measured by transvaginal ultrasonography also has been associated with an increased risk of preterm birth

7
Short cervical length is most commonly defined as less than 25 mm, usually before 24 weeks of gestation, but up to 28 weeks of gestation in some series. It is a cutoff that has been associated with an increased risk of preterm birth in screened populations. Clinically, the shorter the cervical length, the greater the risk of preterm birth.

8
Treatment of other risk factors such as asymptomatic UTI or vaginosis or periodontal disease has not been shown to decrease the rate of preterm delivery.

9
An epidemiologic review of three U. S
An epidemiologic review of three U.S. studies showed that the risk of adverse birth outcomes, including preterm birth, was lowest when the interpregnancy interval was 18–23 months and increased when the inter-val fell outside of this range

10
Other specific tests and monitoring modalities, such as fetal fibronectin screening, bacterial vaginosis testing, and home uterine activity monitoring have been proposed but available interventional studies based on the use of these tests for screening asymptomatic women have not demonstrated improved perinatal outcomes . Thus, these methods are not recommended as screening strategies.

11
Progesterone and the risk of preterm birth among women with a short cervix.
2007 Fonseca EB1, Celik E, Parra M, Singh M, Nicolaides KH; Fetal Medicine Foundation Second Trimester Screening Group. CONCLUSIONS: In women with a short cervix, treatment with progesterone reduces the rate of spontaneous early preterm delivery. (ClinicalTrials.gov number, NCT [ClinicalTrials.gov].).
.")
13
Results: In the 9,974 pregnancies included in the study,
The median cervical length multiple of the median (MoM), corrected for maternal characteristics, was significantly lower in the preterm (0.892 MoM, 95% CI 0.829– 0.945) than in the term delivery group (0.994 MoM, 95% CI 0.919–1.082; p ! ). In screening by a combination of maternal characteristics and cervical length, the estimated detection rate of preterm delivery was 54.8%
, corrected for maternal characteristics, was significantly. lower in the preterm (0.892 MoM, 95% CI 0.829– 0.945) than in the term delivery group (0.994 MoM, 95% CI –1.082; p ! ). In screening by a combination of. maternal characteristics and cervical length, the estimated. detection rate of preterm delivery was 54.8%")
14
Vaginal progesterone reduces the rate of preterm birth in women with a sonographic short cervix: a multicenter, randomized, double-blind, placebo-controlled trial. Hassan SS1, Romero R, Vidyadhari D, Fusey S, Baxter JK, Khandelwal M, Vijayaraghavan J, Trivedi Y, Soma-Pillay P, Sambarey P, Dayal A, Potapov V,O'Brien J, Astakhov V, Yuzko O, Kinzler W, Dattel B, Sehdev H, Mazheika L, Manchulenko D, Gervasi MT, Sullivan L, Conde-Agudelo A, Phillips JA, Creasy GW;PREGNANT Trial. 2011 CONCLUSIONS: The administration of vaginal progesterone gel to women with a sonographic short cervix in the mid-trimester is associated with a 45% reduction in the rate of preterm birth before 33 weeks of gestation and with improved neonatal outcome.

15
Vaginal progesterone prophylaxis for preterm birth
(the OPPTIMUM study): a multicentre, randomised, double-blind trial Feb 2016 Jane Elizabeth Norman, Neil Marlow, Claudia-Martina Messow, Andrew Shennan, Phillip R Bennett, Steven Thornton, Stephen C Robson, Alex McConnachie, Stavros Petrou, Neil J Sebire, Tina Lavender, Sonia Whyte, John Norrie, for the OPPTIMUM study group Vaginal progesterone was not associated with reduced risk of preterm birth or composite neonatal adverse outcomes, and had no long-term benefi t or harm on outcomes in children at 2 years of age.
: a multicentre, randomised, double-blind trial. Feb Jane Elizabeth Norman, Neil Marlow, Claudia-Martina Messow, Andrew Shennan, Phillip R Bennett, Steven Thornton, Stephen C Robson, Alex McConnachie, Stavros Petrou, Neil J Sebire, Tina Lavender, Sonia Whyte, John Norrie, for the OPPTIMUM study group. Vaginal progesterone was not associated with reduced risk of preterm birth or composite neonatal. adverse outcomes, and had no long-term benefi t or harm on outcomes in children at 2 years of age.")
16
ACOG

17
How should women with a previous spontaneous preterm birth be evaluated for risk of subsequent preterm birth?

18
a detailed medical history, reviewing comprehensively aspects of all previous pregnancies, reviewing risk factors, and determining their candidacy for prophylactic interventions, such as progesterone supplementation, cervical cerclage, or both.

19
How should the current pregnancy be managed in a woman with a prior spontaneous preterm delivery?

20
A woman with a singleton gestation and a prior spontaneous preterm singleton birth should be offered progesterone supplementation starting at 16–24 weeks of gestation

21
Based on the pooled results of five clinical trials, in a singleton pregnancy with prior spontaneous preterm birth at less than 34 weeks of gestation and cervical length less than 25 mm before 24 weeks of gestation, cerclage was associated with a 30% reduction in the risk of preterm birth at less than 35 weeks of gestation (28% versus 41%; RR, 0.7; 95% CI, 0.55–0.89) and a 36% reduction in composite perinatal mortality and morbidity
 and a 36% reduction in composite perinatal mortality and morbidity")
22
Insufficient evidence exists to assess whether progesterone and cerclage together have an additive effect in reducing the risk of preterm birth in women at high risk for preterm birth

23
No evidence exists to support the addition of an alternative form of progesterone to the current progesterone treatment (eg, adding a vaginal form to an intramuscular form), if a short cervix is identified in a woman with a prior preterm birth who is already receiving preventive progesterone therapy.
, if a short cervix is identified in a woman with a prior preterm birth who is already receiving preventive progesterone therapy.")
24
Should a woman with a current singleton pregnancy without a history of preterm birth be screened for a risk of preterm birth?

25
The American College of Obstetricians and Gyne-cologists recognizes that both sides of this debate raise valid issues.

26
What interventions have been shown to be beneficial for reducing the risk of preterm birth in women who do not have a history of preterm birth but who are found to have a short cervical length?

27
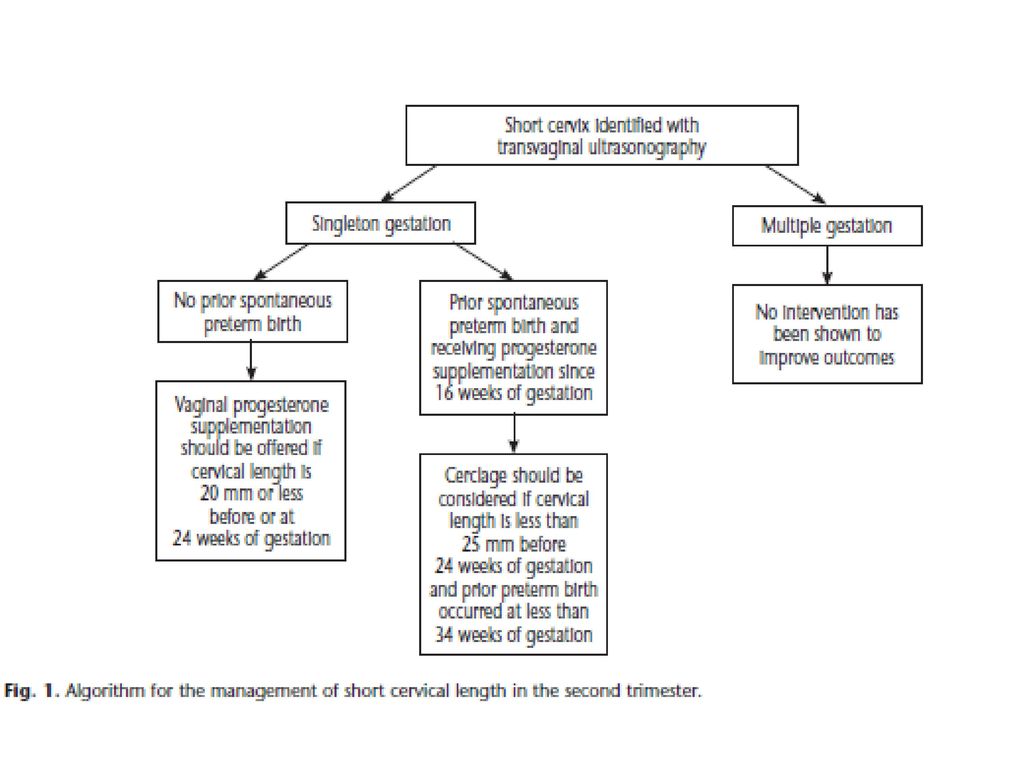
Vaginal progesterone has been studied as a management option to reduce the risk of preterm birth in asymptomatic women with singleton gestations without prior preterm birth with a very short cervical length, defined as less than or equal to 20 mm at up to 24 weeks of gestation.

28
In contrast, for women in this otherwise low-risk population, cerclage placement in women with a cervical length less than 25 mm detected between 16 weeks of gestation and 24 weeks of gestation has not been associated with a significant reduction in preterm birth at less than 35 weeks of gestation

29
Does cerclage placement or progesterone treatment decrease the risk of preterm birth in women with multiple gestations?

30
Available data regarding the efficacy of cerclage placement, progesterone supplementation, or both for the reduction of preterm birth risk in women with multiple gestations with a short cervical length with or without a prior preterm birth do not support their use

40
History-indicated cerclage
Insertion of a cerclage as a result of factors in a woman’s obstetric or gynaecological history which increase the risk of spontaneous second-trimester loss or preterm delivery. A history-indicated suture is performed as a prophylactic measure in asymptomatic women and normally inserted electively at 12–14 weeks of gestation.

41
Ultrasound-indicated cerclage
Insertion of a cerclage as a therapeutic measure in cases of cervical length shortening seen on transvaginal ultrasound. Ultrasound-indicated cerclage is performed on asymptomatic women who do not have exposed fetal membranes in the vagina. Sonographic assessment of the cervix is usually performed between 14 and 24 weeks of gestation

42
Rescue cerclage Insertion of cerclage as a salvage measure in the case of premature cervical dilatation with exposed fetal membranes in the vagina. This may be discovered by ultrasound examination of the cervix or as a result of a speculum/physical examination performed for symptoms such as vaginal discharge, bleeding or ‘sensation of pressure’

43
History-indicated women with three or more previous preterm births
and/or second-trimester losses. Regardless of characteristics of the previous adverse event, such as painless dilatation of the cervix or rupture of the membranes before the onset of contractions.

44
cervical surgery,or prepregnancy diagnostic techniques are not
helpful in the decision to place a history-indicated cerclage.

45
The insertion of an ultrasound-indicated cerclage is not recommended in women without a history of
spontaneous preterm delivery or second-trimester loss who have an incidentally identified short cervix of 25 mm or less.

46
Women with a singleton pregnancy and a history of spontaneous mid-trimester loss or
preterm birth who are undergoing transvaginal sonographic surveillance of cervical length should be offered an ultrasound indicated cerclage if the cervix is 25 mm or less and before 24 weeks of gestation.

47
An ultrasound-indicated cerclage is not recommended for funnelling of the cervix (dilatation of the
internal os on ultrasound) in the absence of cervical shortening to 25 mm or less.
 in the absence of cervical shortening to 25 mm or less.")
48
(see 6.1), while those whose cervix remains long have a low risk.
Who should be offered serial sonographic surveillance ± ultrasound-indicated cerclage? Women with a history of spontaneous second-trimester loss or preterm delivery who have not undergone a history-indicated cerclage may be offered serial sonographic surveillance, as there is evidence to suggest that those who experience cervical shortening are at an increased risk of subsequent second-trimester loss/preterm birth and may benefit from ultrasound-indicated cerclage (see 6.1), while those whose cervix remains long have a low risk.
, while those whose cervix remains long have a low risk.")
49
deliver after 33 weeks of gestation.
Women should be informed that expectant management is a reasonable alternative since there is a lack of direct evidence to support serial sonographic surveillance over expectant management. Furthermore, the majority of women with a history of second-trimester loss/preterm delivery will deliver after 33 weeks of gestation.

50
increase in preterm delivery and pregnancy loss.
The insertion of a history- or ultrasound-indicated cerclage in women with multiple pregnancies is not recommended, as there is some evidence to suggest it may be detrimental and associated with an increase in preterm delivery and pregnancy loss.

51
dilatation and evacuation.
History- or ultrasound-indicated cerclage cannot be recommended in other high-risk groups such as women with müllerian anomalies, previous cervical surgery (cone biopsy, large loop excision of the transformation zone or destructive procedures such as laser ablation or diathermy) or multiple dilatation and evacuation.
 or multiple. dilatation and evacuation.")
52
The decision to place a concomitant cerclage at radical trachelectomy should be individualised

53
When should a rescue cerclage be considered?
Even with rescue cerclage the risks of severe preterm delivery and neonatal mortality and morbidity remain high. Insertion of a rescue cerclage may delay delivery by a further 5 weeks on average It may also be associated with a two-fold reduction in the chance of delivery before 34 weeks of gestation. However, there are only limited data to support an associated improvement in neonatal mortality or morbidity. Advanced dilatation of the cervix (more than 4 cm) or membrane prolapse beyond the external os appears to be associated with a high chance of cerclage failure.
 or membrane prolapse beyond the external os. appears to be associated with a high chance of cerclage failure.")
54
What are the contraindications to cerclage insertion?
● active preterm labour ● clinical evidence of chorioamnionitis ● continuing vaginal bleeding ● PPROM ● evidence of fetal compromise ● lethal fetal defect ● fetal death.

55
scan has been performed recently.
What investigations should be performed before insertion of cervical cerclage? It is good practice to offer a first-trimester ultrasound scan and screening for aneuploidy before the insertion of a history-indicated suture to ensure both viability and the absence of lethal/major fetal abnormality. Before ultrasound-indicated or rescue cerclage, it is good practice to ensure an anomaly scan has been performed recently.

56
Should amniocentesis to detect infection be performed before rescue or ultrasound-indicated cerclage? There is insufficient evidence to recommend routine amniocentesis before rescue or ultrasoundindicated cerclage as there are no clear data demonstrating that it improves outcome.

57
In selected cases where there is suspicion of intra-amniotic infection, amniocentesis may be performed to aid the decision about rescue cerclage, as the presence of infection is associated with a poor prognosis. Amniocentesis before rescue cerclage does not appear to increase the risk of preterm delivery before 28 weeks of gestation.

58
Is amnioreduction before rescue cerclage recommended?
There is an absence of data to either refute or support the use of amnioreduction before insertion of a rescue cerclage.

59
Is there a role for post-cerclage serial sonographic surveillance of cervical length?
While routine serial sonographic measurement of the cervix is not recommended, it may be useful in individual cases following ultrasound-indicated cerclage to offer timely administration of steroids or in utero transfer

60
ultrasound-indicated and rescue cerclage.
Several studies have shown a significant increase in cervical length following the insertion of elective, ultrasound-indicated and rescue cerclage. A postoperative upper cervical length (closed cervix above the cerclage) of less than 10 mm before 28 weeks of gestation appears to provide the best prediction of subsequent preterm delivery before 36 weeks of gestation following the placement of an ultrasound-indicated Cerclage.
 of less than 10 mm before 28 weeks of gestation appears to provide the best prediction of. subsequent preterm delivery before 36 weeks of gestation following the placement of an ultrasound-indicated. Cerclage.")
61
pregnancy loss and delivery before 35 weeks of gestation.
Is there a role for repeat cerclage when cervical shortening is seen post-cerclage? Placement of an ultrasound-indicated cerclage in the presence of cervical length shortening cannot be recommended as, compared with expectant management, it may be associated with an increase in both pregnancy loss and delivery before 35 weeks of gestation. The decision to place a rescue cerclage following an elective or ultrasound-indicated cerclage should be made on an individual basis, taking into account the clinical circumstances.

62
such women makes the finding of a positive result less useful.
Is fetal fibronectin testing useful following insertion of a cervical cerclage? Routine fetal fibronectin testing is not recommended post-cerclage. However, the high negative predictive value of fetal fibronectin testing for subsequent delivery at less than 30 weeks of gestation in asymptomatic high-risk women with a cerclage in place may provide reassurance to women and clinicians in individual cases. However, the increased false-positive rate of fetal fibronectin testing in such women makes the finding of a positive result less useful.

63
Should women receive supplemental progesterone following cerclage?
Routine use of progesterone supplementation following cerclage is not recommended.

65
Thank you very much for your attention

Similar presentations





>")











>")





