Download presentation
Presentation is loading. Please wait.

1
VENERDI’ 08 SETTEMBRE Immuno News Servizio a cura di Filippo de Marinis

2
Blood-based biomarkers for cancer immunotherapy: Tumor mutational burden in blood (bTMB) is associated with improved atezolizumab (atezo) efficacy in 2L + NSCLC (POPLAR and OAK) D. R. Gandara

3
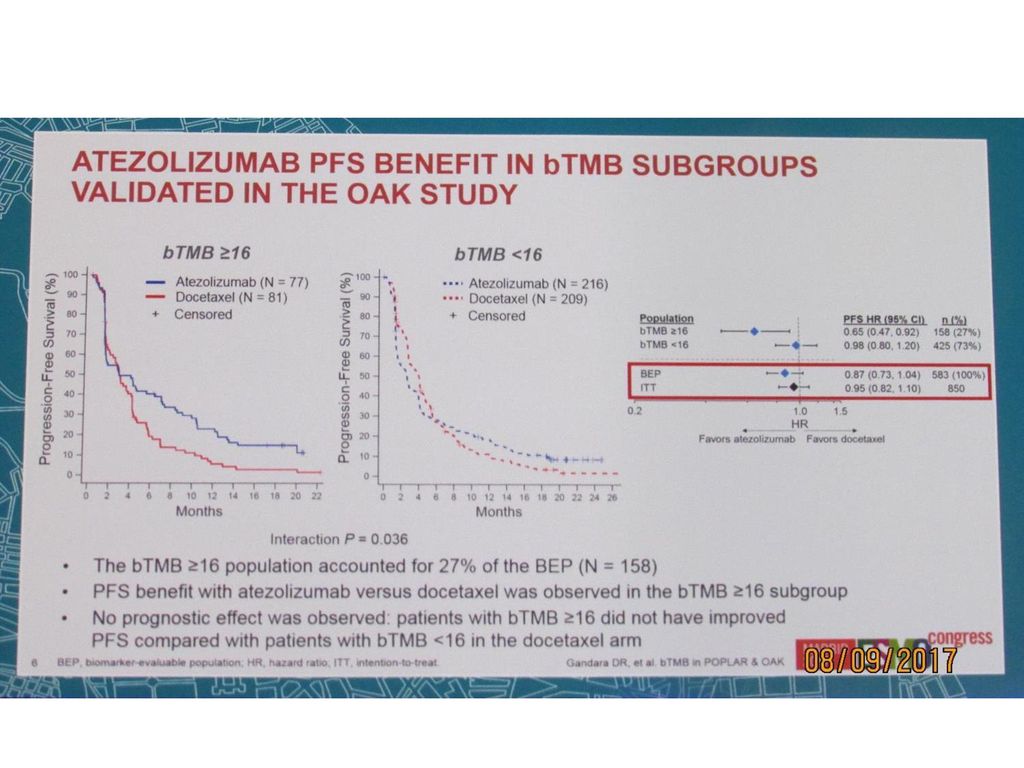
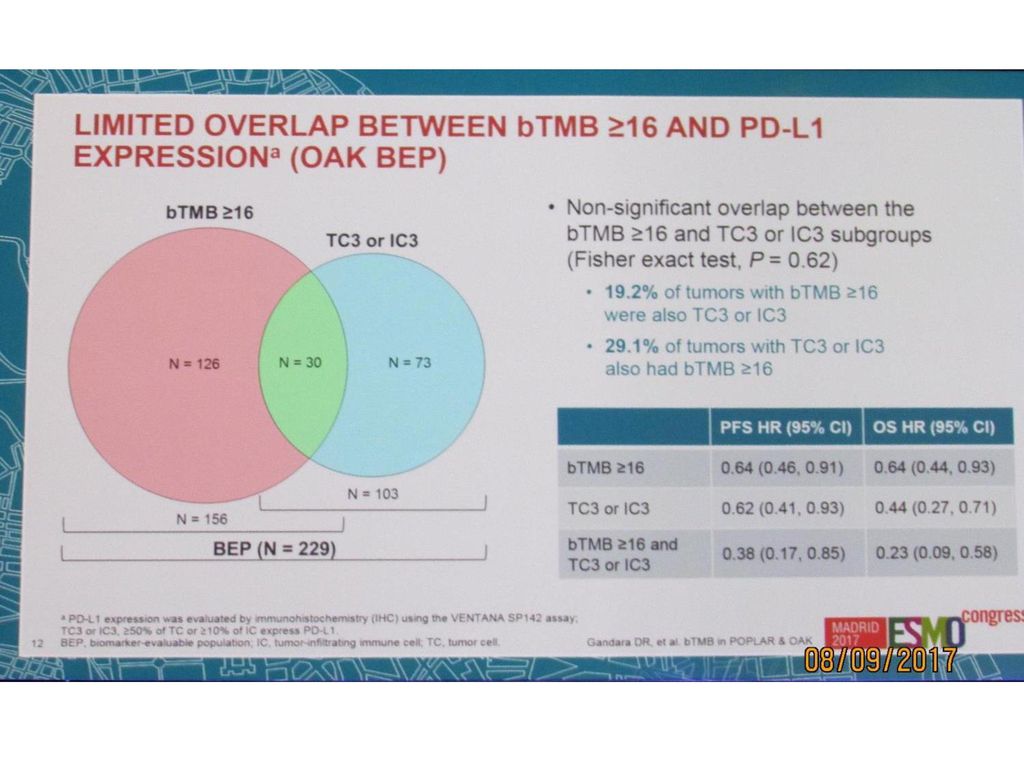
Background Atezo (anti–PD-L1) was FDA approved for 2L+ NSCLC based on results from the randomized OAK and POPLAR trials, with atezo showing superior efficacy vs docetaxel (doc). We previously showed that TMB in tissue correlates with atezo efficacy in 1L+ NSCLC. To address the significant challenge of consistently obtaining sufficient tumor tissue for molecular testing, we developed a novel blood-based assay to measure bTMB. Here we analyzed plasma samples from OAK and POPLAR with the bTMB assay to correlate bTMB with atezo clinical activity Methods The biomarker evaluable population (BEP) included 211 pts in POPLAR (ITT=287) and 583 pts in OAK (excludes pts with known EGFR/ALK mutations; ITT=850), with blood samples available for targeted genomic sequencing. The bTMB assay interrogates single nucleotide variants (SNVs) in 394 genes from cell-free DNA in plasma and reports a score based on the number of high-confidence SNVs identified. The BEP was grouped by bTMB cut points based on the minimum number of SNVs present Results In POPLAR, improved PFS and OS HRs with atezo vs doc were observed at a range of bTMB cut points compared with the ITT and BEP. In OAK, PFS benefit with atezo vs doc was observed at bTMB cut points ≥ 10 compared with BEP. (Table) Importantly, bTMB did not correlate with PD-L1 expression (SP142 or 22C3). Conclusions These exploratory analyses represent the first demonstration of a novel blood-based assay measuring bTMB that may predict atezo clinical efficacy in 2L+ NSCLC. Thus, the bTMB assay may provide a non-invasive biomarker to identify pts who may derive clinical benefit from single agent checkpoint inhibition. Prospective studies using bTMB are currently ongoing in pts with 1L NSCLC (B-F1RST/BFAST).Table: 1295O Clinical efficacy of atezo vs doc in bTMB subgroups POPLAR study ITT (N = 287) BEP (N = 211) OS HR (95% CI) 0.73 (0.53, 0.99) (0.50, 0.93) PFS HR (95% CI) 0.94 (0.72, 1.23) (0.68, 1.20) bTMB subgroup ≥ ≥ 16 ≥ 20 No. of patients OS HR PFS HR OAK study ITT (N = 850) BEP (N = 583) OS HR (95% CI) 0.73 (0.62, 0.87) (0.53, 0.77) PFS HR (95% CI) 0.95 (0.82, 1.10) (0.73, 1.04) bTMB subgroup ≥ ≥ 16 ≥ 20 No. of patients OS HR PFS HR BEP, biomarker-evaluable population; bTMB, tumor mutational burden in blood; ITT, intention to treat
 included 211 pts in POPLAR (ITT=287) and 583 pts in OAK (excludes pts with known EGFR/ALK mutations; ITT=850), with blood samples available for targeted genomic sequencing. The bTMB assay interrogates single. nucleotide variants (SNVs) in 394 genes from cell-free DNA in plasma and reports a score based on the number of high-confidence SNVs identified. The BEP was grouped by bTMB cut points based on the minimum number of SNVs present. Results. In POPLAR, improved PFS and OS HRs with atezo vs doc were observed at a range of bTMB cut points compared with the ITT and BEP. In OAK, PFS benefit with atezo vs doc was observed at bTMB cut points ≥ 10 compared with BEP. (Table) Importantly, bTMB did not correlate with PD-L1 expression (SP142 or 22C3). Conclusions. These exploratory analyses represent the first demonstration of a novel blood-based assay measuring bTMB that may predict atezo clinical efficacy in 2L+ NSCLC. Thus, the bTMB assay may provide a non-invasive biomarker to identify pts who may derive clinical. benefit from single agent checkpoint inhibition. Prospective studies using bTMB are currently ongoing in pts with 1L NSCLC (B-F1RST/BFAST).Table: 1295O Clinical efficacy of atezo vs doc in bTMB subgroups. POPLAR study. ITT (N = 287) BEP (N = 211) OS HR (95% CI) 0.73 (0.53, 0.99) 0.68 (0.50, 0.93) PFS HR (95% CI) 0.94 (0.72, 1.23) 0.90 (0.68, 1.20) bTMB subgroup ≥ 10 ≥ 16 ≥ 20. No. of patients OS HR PFS HR OAK study. ITT (N = 850) BEP (N = 583) OS HR (95% CI) 0.73 (0.62, 0.87) 0.64 (0.53, 0.77) PFS HR (95% CI) 0.95 (0.82, 1.10) 0.87 (0.73, 1.04) bTMB subgroup ≥ 10 ≥ 16 ≥ 20. No. of patients OS HR PFS HR BEP, biomarker-evaluable population; bTMB, tumor mutational burden in blood; ITT, intention to treat.")
16
Clinical efficacy of atezolizumab (Atezo) in PD-L1 subgroups defined by SP142 and 22C3 IHC assays in 2L+ NSCLC: Results from the randomized OAK study S. Gadgeel

17
Clinical efficacy in OAK ITT850 and BEP populations
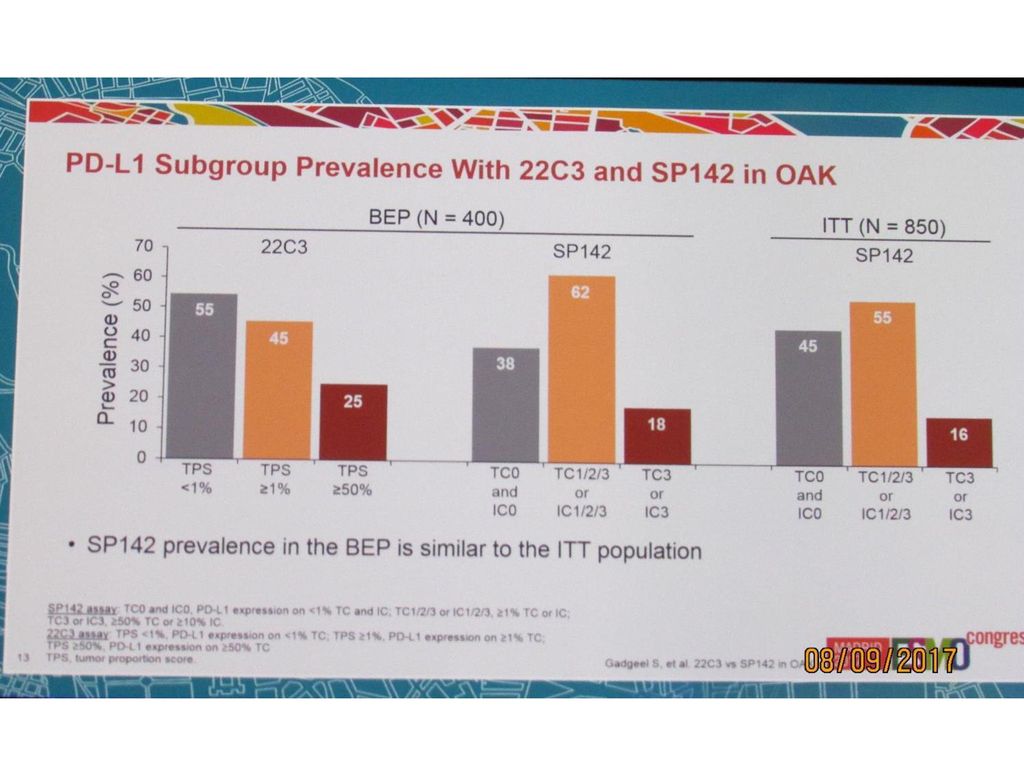
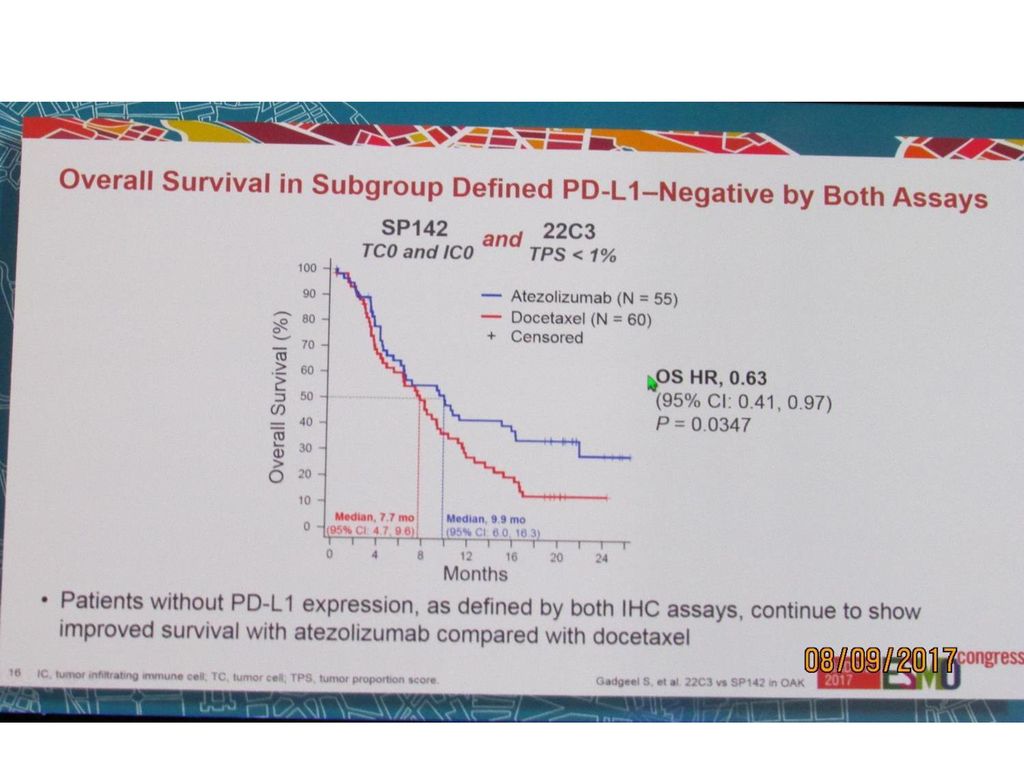
Background In the Phase III OAK trial, patients (pts) with previously treated advanced NSCLC had improved median overall survival (OS) with atezo vs docetaxel (doc), regardless of PD-L1 expression (per VENTANA PD-L1 SP142 IHC assay). Although efficacy correlated with PD-L1 expression on tumor cells (TC) and tumor-infiltrating immune cells (IC), an OS benefit was also observed in pts with PD-L1–negative tumors (i.e., TC0 and IC0; HR, 0.75 [95% CI: 0.59, 0.96]). To determine whether these results were consistent across PD-L1 IHC assays, we assessed atezo efficacy in PD-L1 subgroups as defined by SP142 and Dako 22C3 pharmDx PD-L1 IHC assays. Methods PD-L1 expression was assessed prospectively with SP142 and retrospectively with 22C3. The SP142 assay measured PD-L1 expression on TC and IC, while the 22C3 assay gave a tumor proportion score (TPS) based on TC membrane Results Among the primary population of 850 pts (ITT850), 400 had results from the 22C3 assay (biomarker-evaluable population [BEP]). Clinical outcomes in the BEP vs ITT850, and prevalence in PD-L1 subgroups are summarized (Table). Among pts with tumors negative by SP142 (TC0 and IC0), most (77%) were also negative by 22C3 (TPS < 1%). Comparable OS benefit with atezo was seen in PD-L1–negative subgroups defined by both assays. Improved clinical benefit was observed in pts with the highest PD-L1 expression by either assay (TC3 or IC3 by SP142, or TPS ≥ 50% by 22C3; Table). Conclusions Prevalence of PD-L1 subgroups in the BEP was consistent with previous reports for both assays. Most tumors considered negative by SP142 were also negative by 22C3. An OS benefit (atezo vs doc) was observed in PD-L1–negative subgroups defined by either assay and was consistent with the overall population results from OAK. These data provide evidence of atezo OS benefit in pts with PD-L1–negative tumors irrespective of the PD-L1 IHC assay used.Table: Clinical efficacy in OAK ITT850 and BEP populations ITT850 (N = 850) BEP (N = 400) OS HR (atezo vs doc) (95% CI) (0.62, 0.87) 0.56 (0.44, 0.71) PFS HR (atezo vs doc) (95% CI) (0.82, 1.10) 0.75 (0.61, 0.93) Prevalence of PD-L1 subgroups in OAK BEP (n = 400) SP C3 PD-L1 negative TC0 and IC0, or TPS < 1% % % PD-L1 positive TC1/2/3 or IC1/2/3, or TPS ≥ 1% % % PD-L1 high TC3 or IC3, or TPS ≥ 50% % % OS HR (atezo vs doc) in PD-L1 subgroups in OAK BEP (n = 400) (95% CI) SP C3 PD-L1 negative TC0 and IC0, or TPS < 1% (0.37, 0.80) (0.45, 0.84) PD-L1 positive TC1/2/3 or IC1/2/3, or TPS ≥ 1% (0.42, 0.78) (0.36, 0.73) PD-L1 high TC3 or IC3, or TPS ≥ 50% (0.20, 0.66) (0.29, 0.80
 with previously treated advanced NSCLC had improved median overall survival (OS) with atezo vs docetaxel (doc), regardless of PD-L1 expression (per VENTANA PD-L1 SP142 IHC assay). Although efficacy correlated with. PD-L1 expression on tumor cells (TC) and tumor-infiltrating immune cells (IC), an OS benefit was also observed in pts with PD-L1–negative tumors (i.e., TC0 and IC0; HR, 0.75 [95% CI: 0.59, 0.96]). To determine whether these results were consistent across PD-L1. IHC assays, we assessed atezo efficacy in PD-L1 subgroups as defined by SP142 and Dako 22C3 pharmDx PD-L1 IHC assays. Methods. PD-L1 expression was assessed prospectively with SP142 and retrospectively with 22C3. The SP142 assay measured PD-L1 expression on TC and IC, while the 22C3 assay gave a tumor proportion score (TPS) based on TC membrane. Results. Among the primary population of 850 pts (ITT850), 400 had results from the 22C3 assay (biomarker-evaluable population [BEP]). Clinical outcomes in the BEP vs ITT850, and prevalence in PD-L1 subgroups are summarized (Table). Among pts with tumors negative by SP142 (TC0 and IC0), most (77%) were also negative by 22C3 (TPS < 1%). Comparable OS benefit with atezo was seen in PD-L1–negative subgroups defined by both assays. Improved clinical benefit was observed in pts with the highest PD-L1. expression by either assay (TC3 or IC3 by SP142, or TPS ≥ 50% by 22C3; Table). Conclusions. Prevalence of PD-L1 subgroups in the BEP was consistent with previous reports for both assays. Most tumors considered negative by SP142 were also negative by 22C3. An OS benefit (atezo vs doc) was observed in PD-L1–negative subgroups defined by either. assay and was consistent with the overall population results from OAK. These data provide evidence of atezo OS benefit in pts with PD-L1–negative tumors irrespective of the PD-L1 IHC assay used.Table: Clinical efficacy in OAK ITT850 and BEP populations. ITT850 (N = 850) BEP (N = 400) OS HR (atezo vs doc) (95% CI) 0.73 (0.62, 0.87) 0.56 (0.44, 0.71) PFS HR (atezo vs doc) (95% CI) 0.95 (0.82, 1.10) 0.75 (0.61, 0.93) Prevalence of PD-L1 subgroups in OAK BEP (n = 400) SP142 22C3. PD-L1 negative TC0 and IC0, or TPS < 1% 38% 55% PD-L1 positive TC1/2/3 or IC1/2/3, or TPS ≥ 1% 62% 46% PD-L1 high TC3 or IC3, or TPS ≥ 50% 18% 25% OS HR (atezo vs doc) in PD-L1 subgroups in OAK BEP (n = 400) (95% CI) SP142 22C3. PD-L1 negative TC0 and IC0, or TPS < 1% (0.37, 0.80) (0.45, 0.84) PD-L1 positive TC1/2/3 or IC1/2/3, or TPS ≥ 1% (0.42, 0.78) (0.36, 0.73) PD-L1 high TC3 or IC3, or TPS ≥ 50% (0.20, 0.66) (0.29,")
52
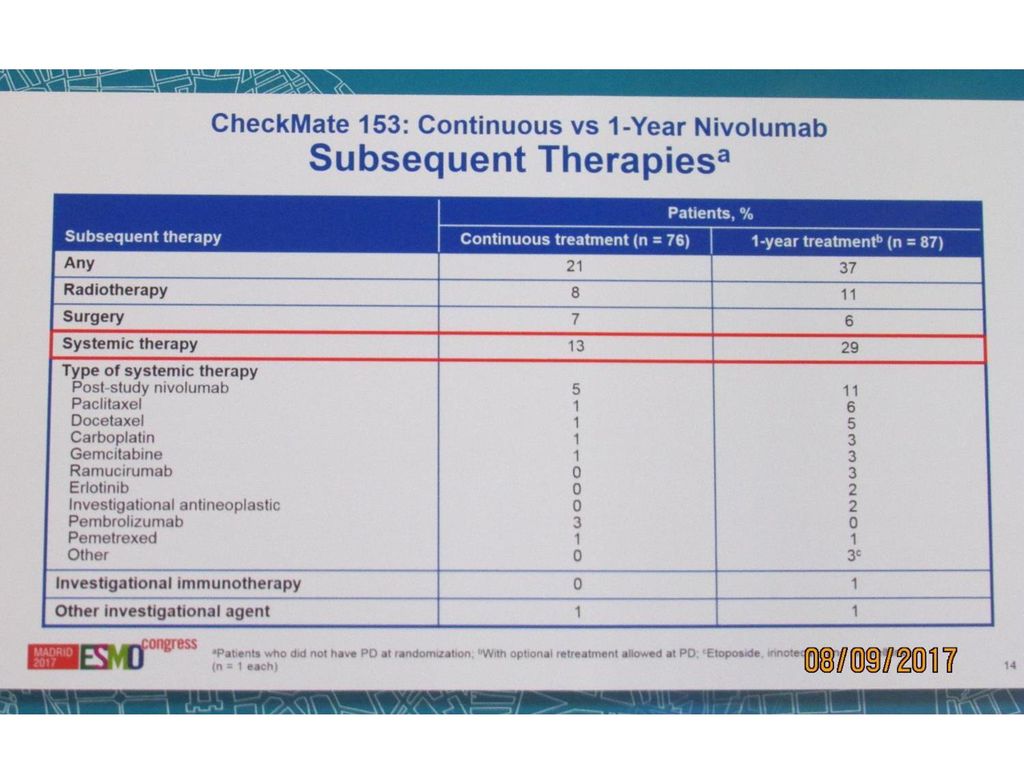
Randomized results of fixed-duration (1-yr) vs continuous nivolumab in patients (pts) with advanced non-small cell lung cancer (NSCLC) D.R. Spigel

53
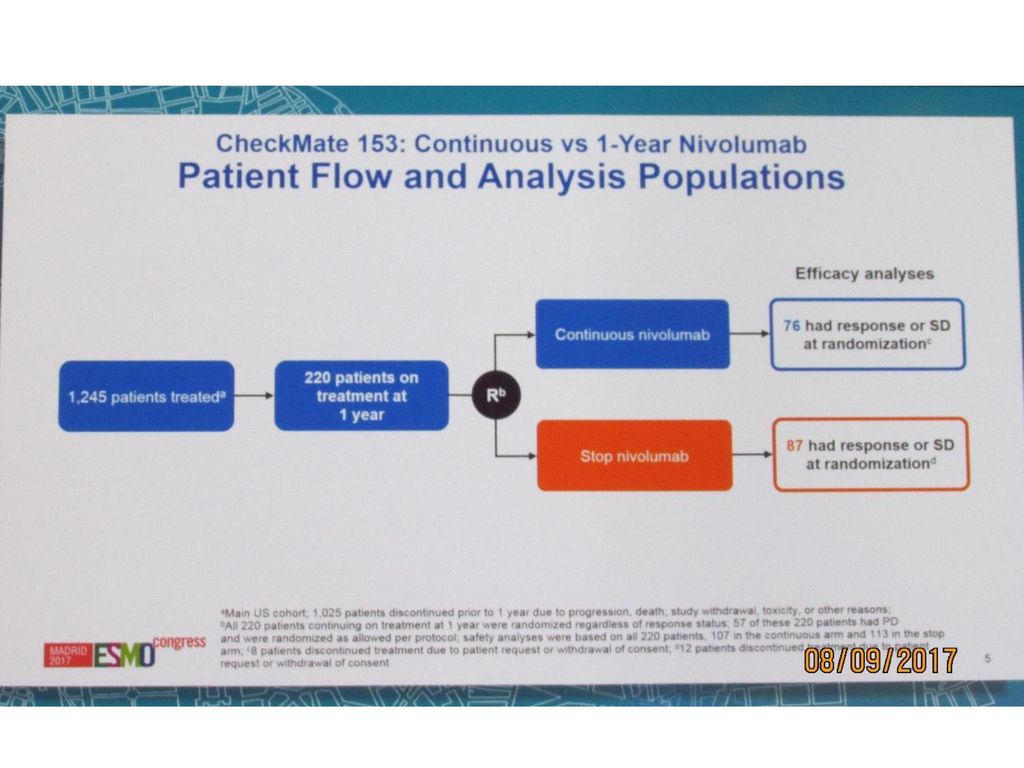
Background Nivolumab, the anti-programmed death (PD)-1 antibody, has demonstrated durable responses and survival benefit in pts with advanced NSCLC, with some pts continuing to derive benefit even after discontinuation of nivolumab (due to adverse events [AEs] or a stopping rule). This raises the question of whether continuous nivolumab treatment is necessary for long-term benefit. CheckMate 153 (NCT ), an ongoing phase IIIB/IV study conducted primarily in the community setting, is evaluating the clinical benefit of a fixed-duration (1 yr) of nivolumab treatment vs continuous treatment in pts with previously treated advanced NSCLC. Pts who remained on nivolumab treatment for 1 yr were randomized to either continue receiving treatment or to stop treatment. Methods Pts with stage IIIB/IV NSCLC and ≥1 prior systemic therapy were enrolled and treated with nivolumab 3 mg/kg IV Q2W. The primary objective of the study overall was the incidence of high-grade (grade 3–5) select treatment-related AEs. Pts still on treatment at 1 yr were randomized 1:1 either to continue nivolumab until progressive disease, unacceptable toxicity, or withdrawal of consent (continuous-treatment arm), or to discontinue treatment, with the possibility of resuming treatment upon disease progression (fixed-duration arm). Prespecified exploratory objectives included safety and efficacy in the 2 randomized arms. Results As of April 2016, 1375 pts were enrolled and treated; 218 pts were randomized after 1 yr of treatment to the continuous-treatment arm (n = 111) or the fixed-duration arm (n = 107).Of these 218 pts, 133 (61%) had received ≥2 prior therapies and 10 (5%) had baseline ECOG PS 2. Data from an upcoming database lock (at which time, the expected post-randomization follow-up ≥10.7 mo) will be presented for randomized pts and will include overall survival, progression-free survival, and safety. In addition, data from pts who were re-treated in the fixed-duration arm will be presented. Conclusions The results from CheckMate 153 represent the first insights from a randomized trial evaluating the impact of stopping treatment with a PD-1/PD-L1 inhibitor at 1 yr vs continuing treatment in pts with advanced, previously treated NSCLC.
-1 antibody, has demonstrated durable responses and survival benefit in pts with advanced NSCLC, with some pts continuing to derive benefit even after discontinuation of nivolumab (due to adverse events [AEs] or a stopping rule). This raises the question of whether continuous nivolumab treatment is necessary for long-term benefit. CheckMate 153 (NCT ), an ongoing phase IIIB/IV study conducted primarily in the community setting, is evaluating the clinical benefit of a fixed-duration (1 yr) of nivolumab treatment vs continuous treatment in pts with previously treated advanced NSCLC. Pts who remained on nivolumab treatment for 1 yr were randomized to either continue receiving treatment or to stop treatment. Methods. Pts with stage IIIB/IV NSCLC and ≥1 prior systemic therapy were enrolled and treated with nivolumab 3 mg/kg IV Q2W. The primary objective of the study overall was the incidence of high-grade (grade 3–5) select treatment-related AEs. Pts still on treatment at 1 yr were randomized 1:1 either to continue nivolumab until progressive disease, unacceptable toxicity, or withdrawal of consent (continuous-treatment arm), or to discontinue treatment, with the possibility of resuming treatment upon disease progression (fixed-duration arm). Prespecified exploratory objectives included safety and efficacy in the 2 randomized arms. Results. As of April 2016, 1375 pts were enrolled and treated; 218 pts were randomized after 1 yr of treatment to the continuous-treatment arm (n = 111) or the fixed-duration arm (n = 107).Of these 218 pts, 133 (61%) had received ≥2 prior therapies and 10 (5%) had baseline ECOG PS 2. Data from an upcoming database lock (at which time, the expected post-randomization follow-up ≥10.7 mo) will be presented for randomized pts and will include overall survival, progression-free survival, and safety. In addition, data from pts who were re-treated in the fixed-duration arm will be presented. Conclusions. The results from CheckMate 153 represent the first insights from a randomized trial evaluating the impact of stopping treatment with a PD-1/PD-L1 inhibitor at 1 yr vs continuing treatment in pts with advanced, previously treated NSCLC.")
69
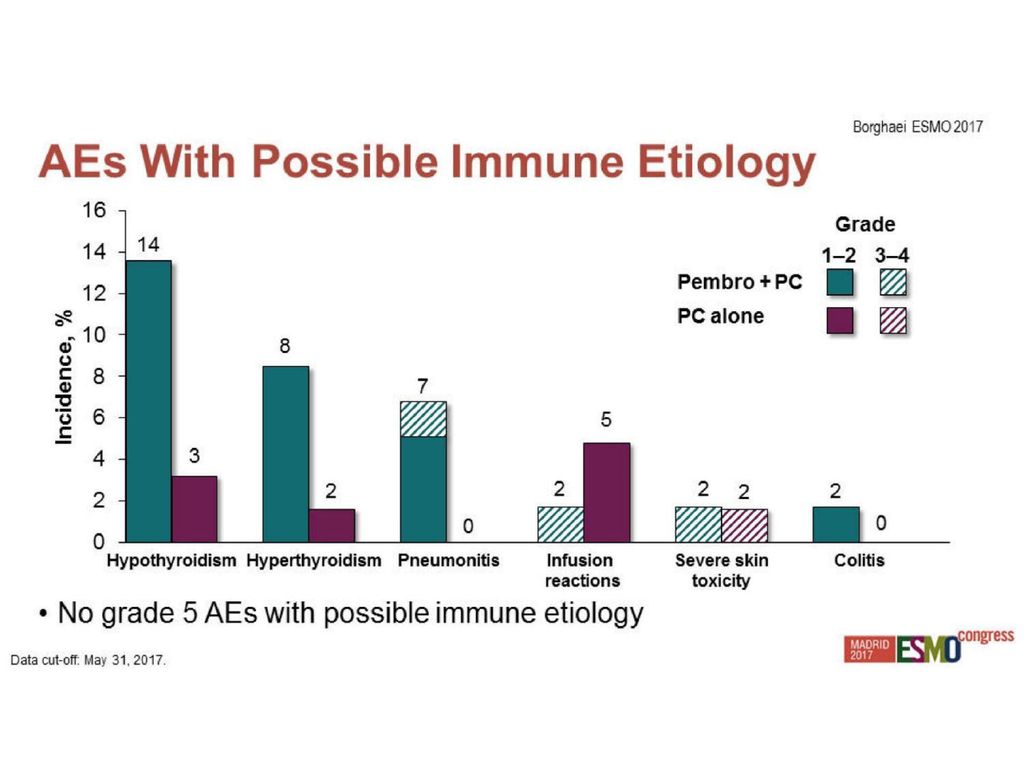
LBA49 - Updated results from KEYNOTE-021 cohort G: a randomized, phase 2 study of pemetrexed and carboplatin (PC) with or without pembrolizumab (pembro) as first-line therapy for advanced nonsquamous NSCLC H. Borghaei

Similar presentations













































































 Shows Favorable Tolerability, Promising Activity in Urothelial Bladder Cancer CCO Independent Conference.>")














>")