Download presentation
Presentation is loading. Please wait.

1
Chapter 16 Documenting, Reporting, Conferring, and Using Informatics

2
Documentation Written evidence of:
The interactions between and among health care professionals, clients, their families, and health care organizations. The administration of tests, procedures, treatments, and client education. The results of, or client’s response to, diagnostic tests and interventions

3
DOCUMENTING is written or computer-based.
All personnel involved in a patient’s health care contribute to the medical record by documenting on the health agency’s forms. Each institution has specific documentation requirements Medical record, also called a chart or client record, is a formal, legal document that provides information about a person’s health problems, the care provided by health practitioners, and the progress of the patient. Although health care organizations use different systems and forms for documentation, all client records have similar information.

4
Principles of Effective Documentation
Nursing notes must be logical, focused, and relevant to care, and must represent each phase of the nursing process. Nursing documentation based on the nursing process facilitates effective care.

5
Guidelines for Documentation: Written Format
Use forms as per agency policy (i.e. flow sheets, graphic sheet, NCP, progress notes) Follow agency guidelines regarding color ink, approved abbreviations, format of time (i.e. military/standard) Write LEGIBLY-questionable info implies doubt, suggests you lack reasonable knowledge NEVER skip lines!! Never chart PRIOR to doing something. Chart as you go—stay current.
 Follow agency guidelines regarding color ink, approved abbreviations, format of time (i.e. military/standard) Write LEGIBLY-questionable info implies doubt, suggests you lack reasonable knowledge. NEVER skip lines!! Never chart PRIOR to doing something. Chart as you go—stay current.")
6
Using the 24-hr Cycle Military Clock for Documenting Times

7
Documenting General Guidelines for Recording
Because the client’s record is a legal document and may be used to provide evidence in court, many factors are considered in recording. Data & Time: Documenting the date and time of each recording. This is essential not only for legal reasons but also for client safety. Record the time in the conventional manner (e.g. 9:00 am or 3:20 pm) or according to the 24-hours clock (military clock). Timing: follow the agency’s policy about the frequency of documenting, and adjust the frequency as a client’s condition indicates; for example, a client whose blood pressure is changing requires more frequent documentation than a client whose blood pressure is constant. You don’t need an order to apply nursing judgment! Legibility: all entries must be legible and easy to read to prevent interpretation errors.
 or according to the 24-hours clock (military clock). Timing: follow the agency’s policy about the frequency of documenting, and adjust the frequency as a client’s condition indicates; for example, a client whose blood pressure is changing requires more frequent documentation than a client whose blood pressure is constant. You don’t need an order to apply nursing judgment! Legibility: all entries must be legible and easy to read to prevent interpretation errors.")
8
Documenting General Guidelines for Recording
Performance: all entries on the client’s record are made in dark ink so that the record is permanent and changes can be identified. Accepted Terminology: use only commonly accepted abbreviations, symbols, and terms that are specified by the agency. Box 17-3 has a list that you will learn. We’ll add others. Correct Spelling: correct spelling is essential for accuracy in recording. If unsure how to spell a word, look it up in a dictionary. Credibility! Signature: each recording on the nursing notes is signed by the nurse making it. The signature includes the name and title; for example, “Susan J. Green, RN” or “SJ Green, RN” You will write “S. Green, HUSN,” and your instructor will cosign.

9
Documenting General Guidelines for Recording
Sequence: documenting events in the order in which they occur; for example, record assessments, then the nursing interventions, and then the client’s responses. Out-of-sequence entries must be acknowledged. See next slide. Accuracy: the client’s name and identifying information should be written on each page of the clinical record. Accurate notations consist of facts or observations rather than opinions or interpretations. It is more accurate, for example, to write that the client “refused medication” (fact) than to write that the client “was uncooperative” (opinion). A legal nightmare!
 than to write that the client was uncooperative (opinion). A legal nightmare!")
10
Date and time your entry on the next available line.
Charting a late entry Date and time your entry on the next available line. Refer to the time the documented event happened in the narrative. Example: 3/12/ Late entry: The patient was noted to have bilateral 2+ pretibial 0900.

11
Documentation Chart facts, not your opinion
Use quotations if the patient said it. Be specific! Using nonspecific terms implies doubt about your knowledge. i.e. appears/seems/tolerated well etc. ABC’s: Accuracy/Brevity/Completeness

12
Guidelines for Documentation: Timing
Chart as soon as possible after care/observations Important to document changes in the patient’s condition, but also what you did about it. NEVER chart what you plan to do Date & time each entry in the margin

13
Guidelines for Documentation: Accountability
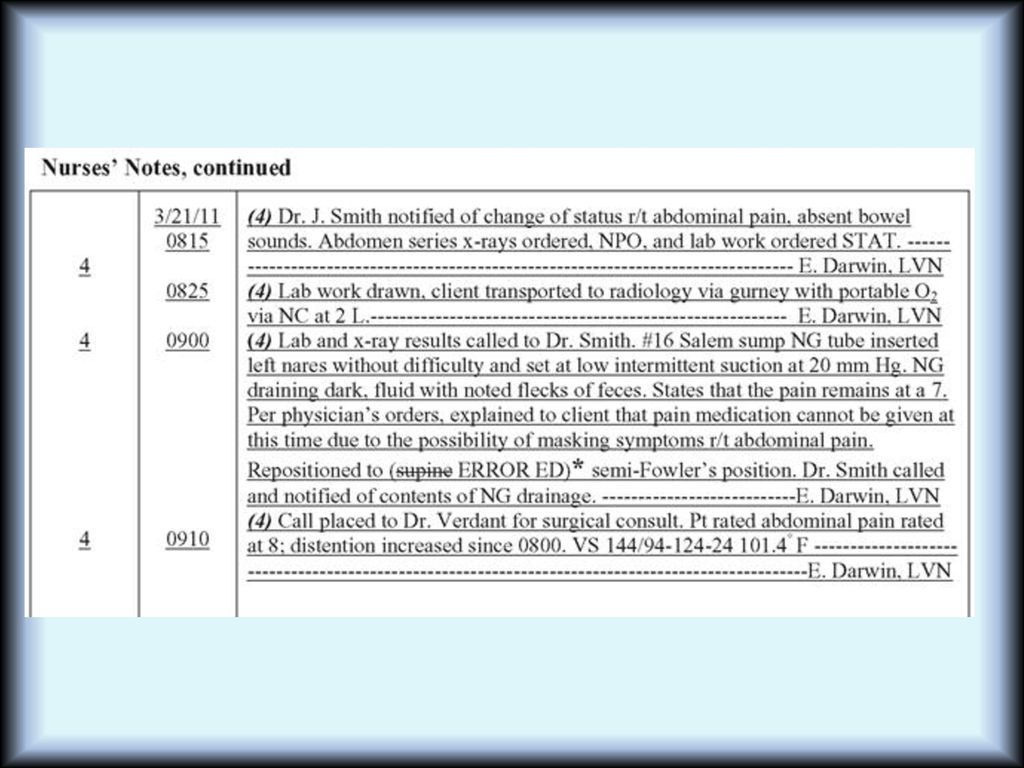
Record is permanent Sign full name and title No erasures Do Not write ERROR for a mistake Single line thru mistake, print “Mistaken Entry” or ME (if acceptable) above or next to mistake, enter correction, initial & date per policy. Other methods—Single strike through, put in parentheses, initials.
 above or next to mistake, enter correction, initial & date per policy. Other methods—Single strike through, put in parentheses, initials.")
14
Correcting errors

15
Guidelines for Documentation: Accountability
IF IT ISN’T DOCUMENTED, IT WASN’T DONE Document all physician visits and phone calls, and what was discussed. If you call the physician to report something, document it. “Dr. Smith notified of 8 cm. area of sanguinous drainage on dressing.” Unusual incidents must be recorded on incident reports or similar forms.

16
Incident Reports Used to document any unusual occurrence or accident in the delivery of client care. Falls, medication errors The incident report is not part of the medical record, but it may be used later in litigation.

17
Guidelines for Documentation: Confidentiality
Students are permitted access to charts for educational purposes Students use only patient initials on all assignments, in every class. Only caregivers need to know info in chart Follow facility policy for pt. review of chart.

18
PRACTICE AND LEGAL STANDARDS
In 80% to 85% of malpractice lawsuits involving client care, the medical record is the determining factor in providing proof of significant events. The legal aspects of documentation require: Writing legible and neat Spelling and grammar properly used Authorized abbreviations used Time-sequenced factual and descriptive entries

19
Legal and Practice Standards
Informed Consent Advance Directives American Nurses Association (ANA) Standards of Care State Nurse Practice Acts Joint Commission on Accreditation of Health Care Organizations (JCAHO)
 Standards of Care. State Nurse Practice Acts. Joint Commission on Accreditation of Health Care Organizations (JCAHO)")
20
Legal & Practice Standards
Nurses are responsible for assessing and documenting that the client has an understanding of treatment prior to intervention. Two indicators of this are Informed Consent and Advance Directives.

21
Legal and Practice Standards
Informed consent means that the client understands the reasons and risks of the proposed intervention. Witnessing confirms that the person who signs the consent is competent.

22
Legal and Practice Standards
An advance directive allows the client to participate in end-of-life decisions. The Patient Self-Determination Act of 1990 requires health care facilities to document whether the client has such a directive.

23
Legal and Practice Standards
American Nurses Association Standards of Care make explicit the role of data collection and documentation in nursing practice.

24
ANA documentation standards
Elements of nursing process needed to be made evident in documentation include: Assessment. Nursing Diagnosis. Planning and outcome identification. Implementation. Evaluation. Revisions of planned care.

25
Meeting Core Standards
A nurse meets the standards by: ■ documenting an assessment of the client’s health status and situation/circumstances ■ ensuring that client preferences for care and outcomes guide the development of any written plan of care ■ documenting consent when the nurse proposes a treatment or intervention ■ documenting the implementation of the care plan and/or the action(s) taken ■ documenting an evaluation of nursing strategies and client outcomes ■ documenting independent and collaborative actions (e.g., those actions ordered by a physician);
 taken. ■ documenting an evaluation of nursing strategies and client. outcomes. ■ documenting independent and collaborative actions. (e.g., those actions ordered by a physician);")
26
Legal and Practice Standards
State Nurse Practice Acts have established guidelines to ensure safe practice. Require evidence of compliance through documentation. To access the Nurse Practice Act, go the OBN website and select “rule and law”

27
Legal and Practice Standards
The Joint Commission on Accreditation of Health Care Organizations (JCAHO) requires documentation of compliance with its standards of care requirements.
 requires documentation of compliance with its standards of care requirements.")
28
Purposes of Health Care Documentation
Reimbursement Peer review organizations (PROs) are required by the federal government to monitor and evaluate care. Medical record documentation is the mechanism for the PRO review.
 are required by the federal government to monitor and evaluate care. Medical record documentation is the mechanism for the PRO review.")
29
REIMBURSEMENT The federal government requires monitoring and evaluation of quality, appropriateness of care provided. Documentation of intensity of services and severity of illness reviewed. Failure to document can result in reimbursement denied.

30
Reimbursement Diagnosis-Related Groups (DRG)
Patients are assigned a DRG based on their admitting diagnosis Each DRG has a clinical pathway—like a recipe—that patients move along on their way to wellness Federally mandated since the 1980’s, determines how much money hospitals get for each “product,” since patients in each “product” category are similar and are expected to use the same level of resources. Case Managers (nurses) review charts to assure care is appropriate and ongoing. The medical record must provide documentation that supports the DRG and appropriateness of care. If nurses fail to document the equipment or procedures used daily, reimbursement to the facility can be denied.
 review charts to assure care is appropriate and ongoing. The medical record must provide documentation that supports the DRG and appropriateness of care. If nurses fail to document the equipment or procedures used daily, reimbursement to the facility can be denied.")
31
HIPAA Laws Finalized regulations established 2000, modified by the Bush administration 2002. All health agencies have HIPAA training for workers Violations may result in jail/ $25,000 fines. PATIENT RECORDS ARE CONFIDENTIAL

32
What Is Confidential? All information about patients written on paper, spoken aloud, saved on computer Name, address, phone, fax, social security Reason the person is sick Treatments patient receives Information about past health conditions HIV status may even be absent from the chart deliberately. Worried? Then be sure to use standard precautions on EVERY patient.

33
Some real-life examples…
Don’t talk about patients in the elevator, on the shuttle bus, or on Facebook. Hospitals monitor Facebook Don’t let anyone use your computer password—ever! Don’t tell patients’ visitors ANYTHING Never give phone information Don’t copy/take pictures of your patient’s chart for your care plan. Don’t look up anyone else’s test results—even your own! Don’t try to get into someone’s chart/EHR unless you are assigned to that patient. This is monitored by IT!

34
Question Tell whether the following statement is true or false.
A nurse who fails to log off a computer after documenting patient care has breached patient confidentiality. A. True B. False

35
Answer Answer: A. True A nurse who fails to log off a computer after documenting patient care has breached patient confidentiality.

36
Potential Breaches in Patient Confidentiality
Displaying information on a public screen Sending confidential messages via public networks Sharing printers among units with differing functions Discarding copies of patient information in trash cans Holding conversations that can be overheard Faxing confidential information to unauthorized persons Sending confidential messages overheard on pagers

37
Patient Rights See and copy their health record—hospitals have policies on this that you must follow. Update their health record Get a list of disclosures Request a restriction on certain uses or disclosures Choose how to receive health information Choose who can know about their condition

38
Question Tell whether the following statement is true or false.
A patient has the right to obtain, review, and revise the patient information in his or her health record. A. True B. False

39
Answer Answer: B. False A patient has the right to obtain and review, but not revise the patient information in his or her health record.

40
Documenting Purposes of client records
Communication: patient’s record serves as the vehicle by which different members of the health team communicate and share information with each other. Assessment: nurses and other health team members gather assessment data from the patient’s record. Planning patient care: the entire health team uses data from the patient’s record to plan care for the patient. Education & research: nursing students, medical students and other health team members often use patient record as an educational tools. It provides a comprehensive view of the patient’s health status. The information contained in a record can be a valuable source of data for research.

41
Documenting Purposes of client records
Legal documentation: the client’s record is a legal document and is usually admissible in court as evidence. Health care analysis: records can be used to establish the costs of various services and to identify those services that cost the agency money and those that generate revenue. Auditing health agencies: patient’s record is used to monitor the care received by the patient and the competence of people giving that care.

42
Other forms of Communication--Orders
The chart is a method of communicating between disciplines Diagnostic and therapeutic orders Who can write these orders? Physicians, dentists, podiatrists, psychologists, PA’s, APN’s who are licensed, have privileges. (residents and interns count—they are doctors, but medical students’ orders must be cosigned by a physician.) Written orders Preferred! Must be signed/dated by the provider. Verbal orders v.o. Dr. Smith/M. Jones RN Only in emergencies, then Dr. (or provider) must co-sign Telephone orders t.o .Dr. Smith/M. Jones RN Read it back
 Written orders. Preferred! Must be signed/dated by the provider. Verbal orders. v.o. Dr. Smith/M. Jones RN. Only in emergencies, then Dr. (or provider) must co-sign. Telephone orders. t.o .Dr. Smith/M. Jones RN. Read it back.")
43
Documenting a Telephone Order

44
Other forms of communication--Reporting
Change of shift report Summary of patient condition and current status of care, from off-going nurse to oncoming-nurse Types of shift report Face-to Face Audiotaped Walking rounds Students will receive report and be expected to give report when leaving Learn to use a report sheet! Examples….

45
INFORMATION FOR SHIFT REPORT
Name, room and bed, age, gender Physician, admission date, and diagnosis Diagnostic tests or treatments performed in past 24 hours (results if ready) Handout—try it, or make your own. General status, any significant change New or changed physician’s orders IV fluid amounts, last PRN medication Concerns about client
 Handout—try it, or make your own. General status, any significant change. New or changed physician’s orders. IV fluid amounts, last PRN medication. Concerns about client.")
46
Other reports Talking to physicians Transfers/Discharge Reports
SBAR Transfers/Discharge Reports Nurse to nurse Family condition reports HIPAA rules apply Do not inform about bad test results—some things are to be done by physicians

47
Here is an example of a call to a physician using SBAR: Introduction:
Dr. Jones, this is Deb McDonald RN, I am calling from ABC Hospital about your patient Jane Smith. Situation: Here's the situation: Mrs. Smith is having increasing dyspnea and is complaining of chest pain. Background: She is 2nd day post op from a total knee replacement. About two hours ago she began complaining of chest pain. Her pulse is 120 and her blood pressure is 128/54. She is restless and short of breath. Assessment: I think she may be having a cardiac event or a pulmonary embolism. Recommendation: I need someone to evaluate her STAT, so I called the 3rd year resident, because I know you’re in the office. I also started O2 via nasal canula at 8 liters/min. I can have a STAT EKG done, if you’d like. She has an IV of NS running at 100 ml/hr and I cancelled her lunch for now and made her NPO. Is there anything else you want me to do?

48
Methods of Documentation
Narrative Charting Source-Oriented Charting Problem-Oriented Charting PIE Charting Focus Charting Charting by Exception (CBE) Computerized Documentation Case Management with Critical Paths
 Computerized Documentation. Case Management with Critical Paths.")
49
Methods of Documentation
Source-Oriented Charting Narrative recording by each member (source) of the health care team on separate records.
 of the health care team on separate records.")
50
Methods of Documentation
Narrative Charting Describes the client’s status, interventions and treatments; response to treatments is in story format. Narrative charting is now being replaced by other formats. We’ll look at some examples, but first, let’s look at some rules of charting…..

51
Documenting Nurses Remarks Methods of Charting Date/time 13.30 pm
Narrative charting: Narrative charting (style of documentation generally used in source-oriented records) involves writing information about the patient and patient care in chronologic order. Nursing Notes Date/time Nurses Remarks 13.30 pm States “I am having chest pain. It’s like an elephant is sitting on me” B. Zook, RN 13.40 pm Skin is pale & moist. O2 started at 5L/min Nitroglycerin tablet administered sublingual Figure 1 Sample of narrative charting
 involves writing information about the patient and patient care in chronologic order. Nursing Notes. Date/time. Nurses Remarks pm. States I am having chest pain. It’s like an elephant is sitting on me B. Zook, RN pm. Skin is pale & moist. O2 started at 5L/min. Nitroglycerin tablet administered sublingual. Figure 1 Sample of narrative charting.")
53
Procedural narrative notes
5/15/ #16 fr. Foley catheter inserted to closed drainage. Draining moderate amounts clear straw-colored urine. Pt. remained stable throughout the procedure (or pt. tolerated procedure well, if your institution allows that) S. Smith RN 5/15/ Right chest tube dressing changed for small amount of serosanguinous drainage. Site benign. No crepitus noted. Replaced dressing w/ vasoline gauze and drain sponges per policy. All tubing checked for air leaks, no leaks noted. Tubes taped and secured to body. Pt. remained stable throughout the procedure (or tolerated well, depending on policy).-----S. Smith RN
 S. Smith RN. 5/15/ Right chest tube dressing changed for small amount of serosanguinous drainage. Site benign. No crepitus noted. Replaced dressing w/ vasoline gauze and drain sponges per policy. All tubing checked for air leaks, no leaks noted. Tubes taped and secured to body. Pt. remained stable throughout the procedure (or tolerated well, depending on policy).-----S. Smith RN.")
54
How do I know what to say? Writing a narrative can be hard for beginners. You must write the sentences in the chronological order in which things were done. Don’t use complete sentences or say “I noted…” Say “thus-and-such noted.” You’ve got to know the words! To that end---here are some handouts you need to memorize!

55
Methods of Documentation
Problem-Oriented Charting (POMR) Has 4 elements: database, problem list, POC, and progress note, written in SOAP format Uses a structured, logical format called S.O.A.P. S: subjective data O: objective data A: assessment (conclusion stated in form of nursing diagnoses or client problems) P: plan
 Has 4 elements: database, problem list, POC, and progress note, written in SOAP format. Uses a structured, logical format called S.O.A.P. S: subjective data. O: objective data. A: assessment (conclusion stated in form of nursing diagnoses or client problems) P: plan.")
56
Problem-Oriented Charting (POMR)
SOAPIE and SOAPIER refer to formats that add: I: Intervention E: Evaluation R: Revision

57
Problem-Oriented Charting (POMR)
Uses flow sheets to record routine care. A discharge summary addresses each problem. SOAP entries are usually made at least every 24 hours on any unresolved problem. SOAP was developed on a medical model.

58
Documenting Types of Patient Records
SOAP charting: SOAP charting (documentation style more likely to be used in a problem-oriented record) acquired its name from the four essential components included in a progress note: * S : subjective data * O : objective data * A : analysis of the data * P : plan for care SOAP charting helps to demonstrate interdisciplinary cooperation, because everyone involved in the care of a patient makes entries in the same location in the chart.
 acquired its name from the four essential components included in a progress note: * S : subjective data. * O : objective data. * A : analysis of the data. * P : plan for care. SOAP charting helps to demonstrate interdisciplinary cooperation, because everyone involved in the care of a patient makes entries in the same location in the chart.")
59
Documenting Types of Patient Records Letter Explanation Nurses Remarks
Subjective Information reported by the patient S – “I don’t feel well” Objective Information reported by the nurse O - Temperature 38C Analysis Problem identification A – Fever Plan Proposed treatment P – Increased fluid intake & Monitor body temperature. Call Dr. for acetaminophen order SOAP charting format

60
Methods of Documentation
PIE Charting P: Problem I: Intervention E: Evaluation Key components are assessment flow sheets and the nurses’ progress notes with an integrated plan of care. PIE charting is a nursing model.

61
Documenting Nurses Remarks Types of Patient Records Date/time 6/6
PIE charting: PIE charting is method of recording the patient’s progress under the headings of problem, intervention, and evaluation. When the PIE method is used, assessments are documented on separate form and the patient’s problems are given a corresponding number. Date/time Nurses Remarks 6/6 8.30 am P# 1 crackles heard on inspiration in the bases of R and L lungs. I# 1 splinted with pillow. Instructed to breathe deeply, open mouth, and cough at the end of expiration. E# 1 Lungs clear with coughing. L Cass, HN Sample of PIE charting

63
Methods of Documentation
Focus Charting A method of identifying and organizing the narrative documentation of all client concerns. Includes data, action, response. Uses a columnar format within the progress notes to distinguish the entry from other recordings in the narrative notes.

64
Documenting Types of Patient Records
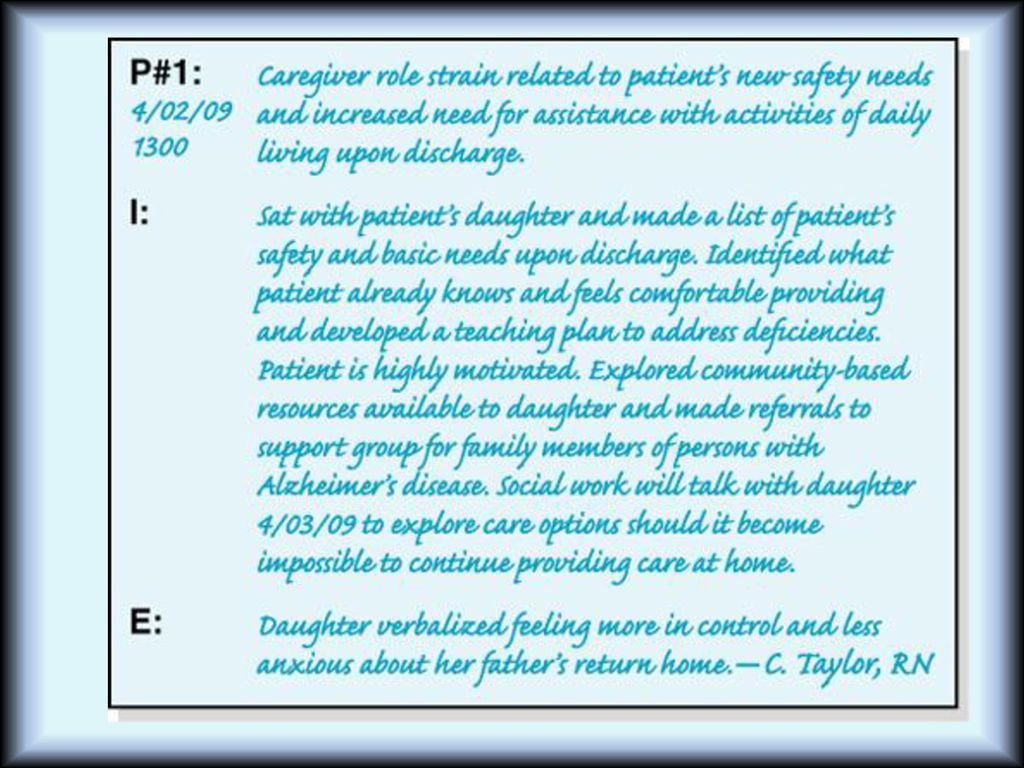
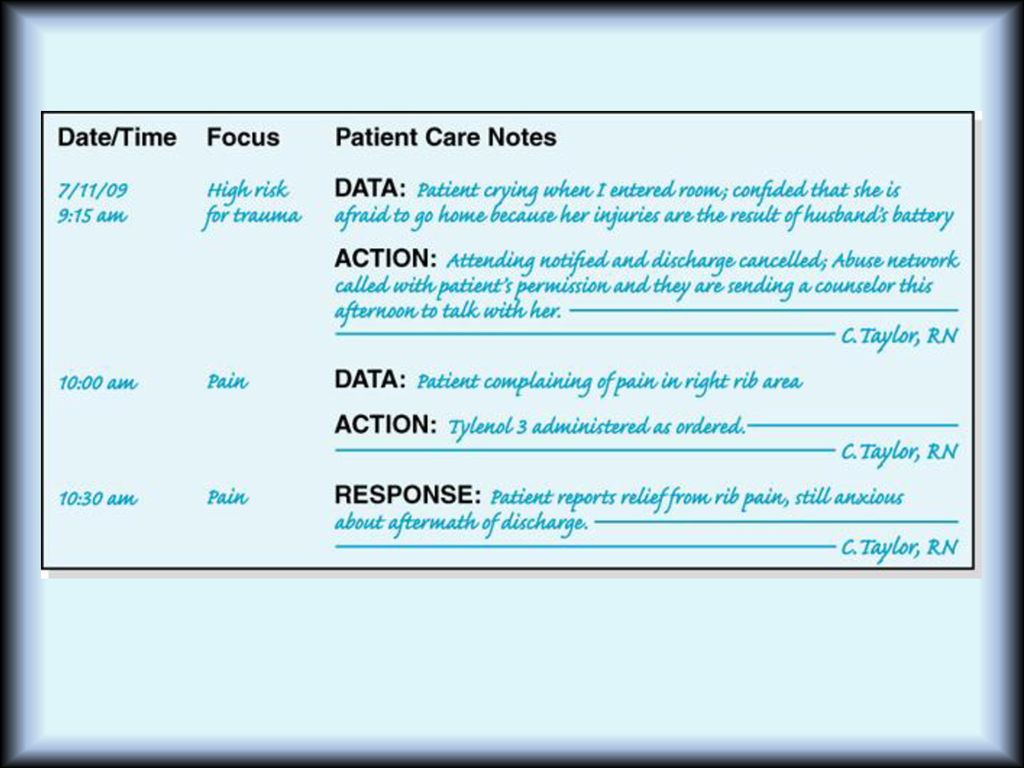
Focus charting: Focus charting (modified form of SOAP Charting) uses the word focus rather than problem, because some believe that the word problem carries negative connotations. Focus charting used DAR model: D = data category reflects the assessment phase of the nursing process A = action category reflects planning & implementation phase of the nursing process. R = response category reflect the evaluation of the nursing process DAR notation tends to reflect the steps in the nursing process.
 uses the word focus rather than problem, because some believe that the word problem carries negative connotations. Focus charting used DAR model: D = data category reflects the assessment phase of the nursing process. A = action category reflects planning & implementation phase of the nursing process. R = response category reflect the evaluation of the nursing process. DAR notation tends to reflect the steps in the nursing process.")
65
Focus charting Types of Patient Records 6/6/2006
D (data) - Bladder distended 2 fingers above pubis. Patient states, “I feel like my bladder is full but I can’t go on this bedpan.” 10.15 am Has not urinated since catheter was removed 6 hours ago A (action) –Assisted to toilet. Faucet turned on, dangled fingers in basin of water, provided privacy R (response)- voided 525ml of clear urine L. Cass, SN Example of DAR charting
 - Bladder distended 2 fingers above pubis. Patient states, I feel like my bladder is full but I can’t go on this bedpan am. Has not urinated since catheter was removed 6 hours ago. A (action) –Assisted to toilet. Faucet turned on, dangled fingers in basin of water, provided privacy. R (response)- voided 525ml of clear urine L. Cass, SN. Example of DAR charting.")
67
Question Which of the following methods of documentation is unique in that it does not develop a separate plan of care but instead incorporates the plan of care into the progress notes? A. Source-oriented records B. Problem-oriented records C. PIE (problem, intervention, evaluation) D. Focus charting
 D. Focus charting.")
68
Answer Answer: C. PIE (problem, intervention, evaluation) Rationale:
PIE charting incorporates the plan of care into progress notes in which problems are identified by number. In source-oriented records, each healthcare group keeps data on its own separate form. Problem-oriented records are organized around patient problems rather than around sources of information. Focus charting brings the focus of care back to the patient and the patient’s concerns.

69
Methods of Documentation
Charting by Exception (CBE) The nurse documents only deviations from preestablished norms. Avoids lengthy, repetitive notes. Enables the identification of trends in client status.
 The nurse documents only deviations from preestablished norms. Avoids lengthy, repetitive notes. Enables the identification of trends in client status.")
70
CBE—old Summa forms (they are now all electronic
CBE—old Summa forms (they are now all electronic.) Checkboxes unless something was out of the ordinary.
 Checkboxes unless something. was out of the ordinary.")
71
Methods of Documentation
Case Management Process A methodology for organizing client care through an illness, using a critical pathway. A critical pathway is a monitoring and documentation tool used to ensure that interventions are performed on time and that client outcomes are achieved on time.

72
Forms for Recording Data
Kardex Nursing Assessment Sheet (covered in previous chapter) Flow Sheets Nurses’ Progress Notes (also called nurses’ notes) Discharge Summary MAR (Medication Administration Record) (Lorantffy handouts)
 Flow Sheets. Nurses’ Progress Notes (also called nurses’ notes) Discharge Summary. MAR (Medication Administration Record) (Lorantffy handouts)")
73
Forms for Recording Data
The Kardex is used as a reference throughout the shift and during change-of-shift reports. Client data Medical diagnoses and nursing diagnoses Medical orders Activities

74
Forms for Recording Data
Flow sheets reduce the redundancy of charting in the nurses’ progress notes. The information on flow sheets can be formatted to meet the specific needs of the client.

75
Flow Sheets Vertical or horizontal columns for recording dates and times and related assessment and intervention information. Also included are notes on: Client teaching. Use of special equipment. IV Therapy.

76
Forms for Recording Data
Nurses’ progress notes are used to document the client’s condition, problems and complaints, interventions, responses, achievement of outcomes. Progress notes can be completely narrative or incorporated into a standardized flow sheet.

77
Forms for Recording Data
Discharge Summary Client’s status at admission and discharge Brief summary of client’s care Interventions and education outcomes Resolved problems and continuing need Referrals Client instructions

78
Forms The MAR is for recording daily and prn medications
Used at the bedside as a patient identifier

79
Charting a prn medication

80
COMPUTERIZED DOCUMENTATION
Reduces time taken, increases accuracy. Increases legibility. Stores, retrieves information quickly. Improves communication among health care departments. Confidentiality and costs can be problems.

81
Electronic Documentation
Bedside data entry Abilities of EMR’s Retrieval by caregivers, administrators, third-party payers Trending and tracking Concerns about EMR’s Security of data No national standards Depersonalization of care

82
Electronics in Health Care
Client monitoring devices have been used for years Telemedicine/telehealth Practice management

83
Nursing Informatics According to the ANA, the role of the informatics nurse is distinguished from other informatics roles by its association with patient care delivery. ANA provided the current definition in 2001 as: A specialty that integrates nursing science, computer science and information science to manage and communicate data, information, and knowledge in nursing/patient practices. Facilitates the integration of data, information, knowledge to support patients, nurses and other providers in their decision-making in all roles and settings.

84
Components of Practice: Transformation of Data to Knowledge
The transformation of data to knowledge is a key concept of the nursing informatics role and has the potential to significantly impact nursing practice. It involves three components: 1. Data are discrete entities that are described objectively without interpretation 2. Information is data that are interpreted, organized, or structured 3. Knowledge is information that is synthesized so that relationships are identified and formalized.

85
Core Functions of EHR’s
Health information and data Results management Order management Decision support Electronic connectivity Patient support Administrative processes and reporting

86
WHY EHR’s are important
Historically, there are drawbacks to paper records. Certainly, EHR’s have fixed many of these. But problems still exist. Read “Where’s my Chart?” and answer the following questions: What are the dangers to the client when the provider has no access to their old charts? How would this situation have been improved if the EHR’s were interconnected?

87
Workflows, old and new Outpatient settings: Workflows in an office using paper charts are compared to an office using EHR. (see handouts) Inpatient settings: Significant differences exist which make EHR more efficient

88
Problems of Paper Record
• Chart is thick • Disorganized and illegible • Problems in finding data • Record fragmentation • Archiving issues (space, environmental control) • Handling files issues (occupational hazards)
 • Handling files issues (occupational hazards)")
89
Benefits of EHR’s More time spent with patient and less time at nurse station Reduce paperwork / paper loss Automated tools of nursing documentation Accurate logging of nurses activities Uniform standards of nursing care are programmed (nursing process) Cost reduction (Fewer loss of charges) Timely transfer of test results Decision support—computer gives you advice
 Cost reduction (Fewer loss of charges) Timely transfer of test results. Decision support—computer gives you advice.")
90
Point of Care documentation
Nurse enters data at the client’s bedside Real-time entry makes data available immediately Can be COWs or fixed computer workstations located throughout the unit Tablets with handwriting or speech recognition

91
Guidelines for safe computer charting
Don’t let anyone use your password Always log off when you are done Never delete anything. Use error protocols. Don’t leave patient info displayed on the monitor where it can be seen Don’t use to send protected patient information

92
Guidelines for aesthetic use of computers
Bedside computers may help us, but don’t forget to talk to the patient. Nurse the patient, not the computer Look the patient in the eye when he talks, not at your computer screen. Don’t fiddle around with it in the patient’s room—if you’re unsure where to find data, leave the room and do it elsewhere.

Similar presentations

 VUMC Privacy Website www.mc.vanderbilt.edu/privacy.>")

















 Other words (Reporting, Documenting, Charting,>")