Download presentation
Presentation is loading. Please wait.

1
بسم الله الرحمن الرحيم

2
Imaging modalities in diagnosis breast cancer Dr. Mostafa M. Azouz

3
* IMAGING * The standard techniques used for breast imaging are: 1. Mammography. 2. Real-Time ultrasound. 3. Other techniques include:

4
MRI Color Doppler Ultrasound elastography Scintimammography

5
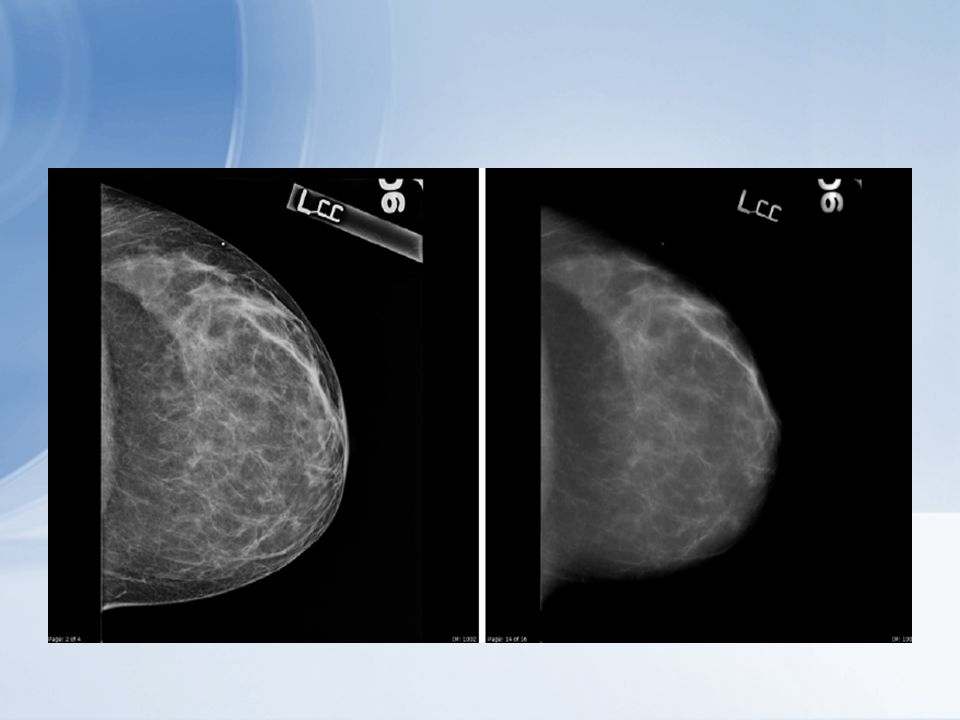
Mammography can find abnormalities between one and three years before they can be felt. Because the inherent attenuation differences between normal & diseased breast tissues is so small, high quality mammography required.

6
Although mammography is the most sensitive exam available for detecting small breast ca. False Negative Rate is 5-10% Mammography

7
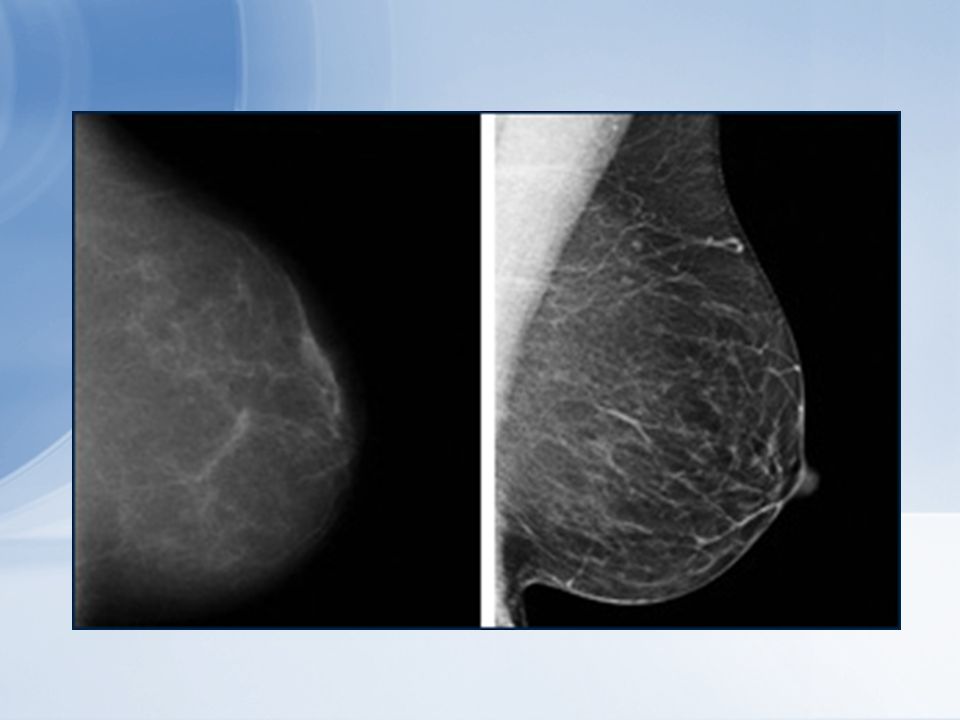
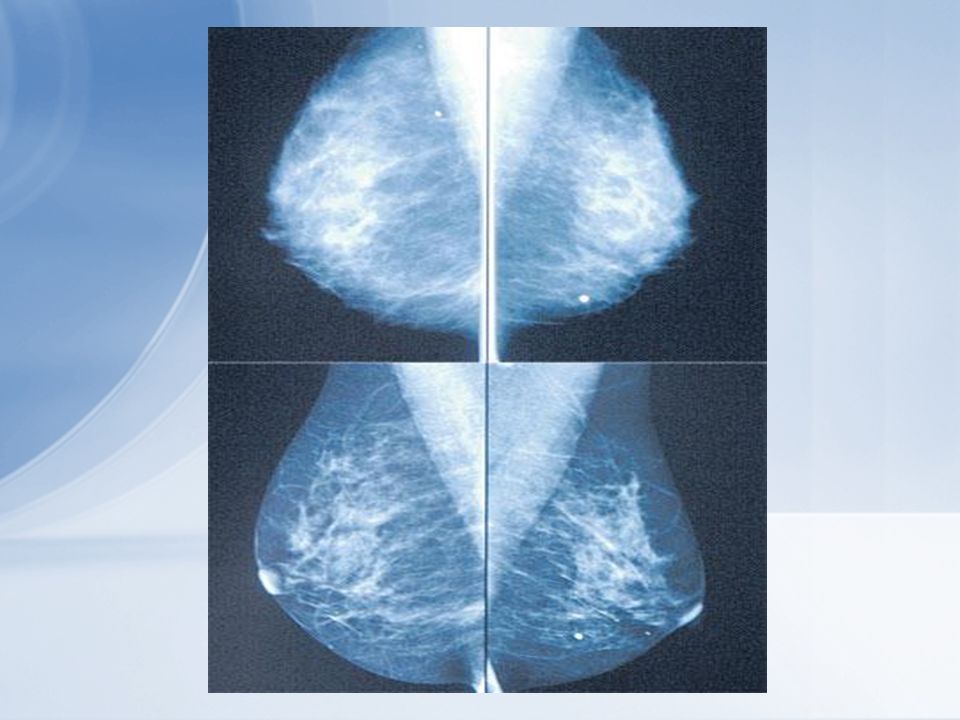
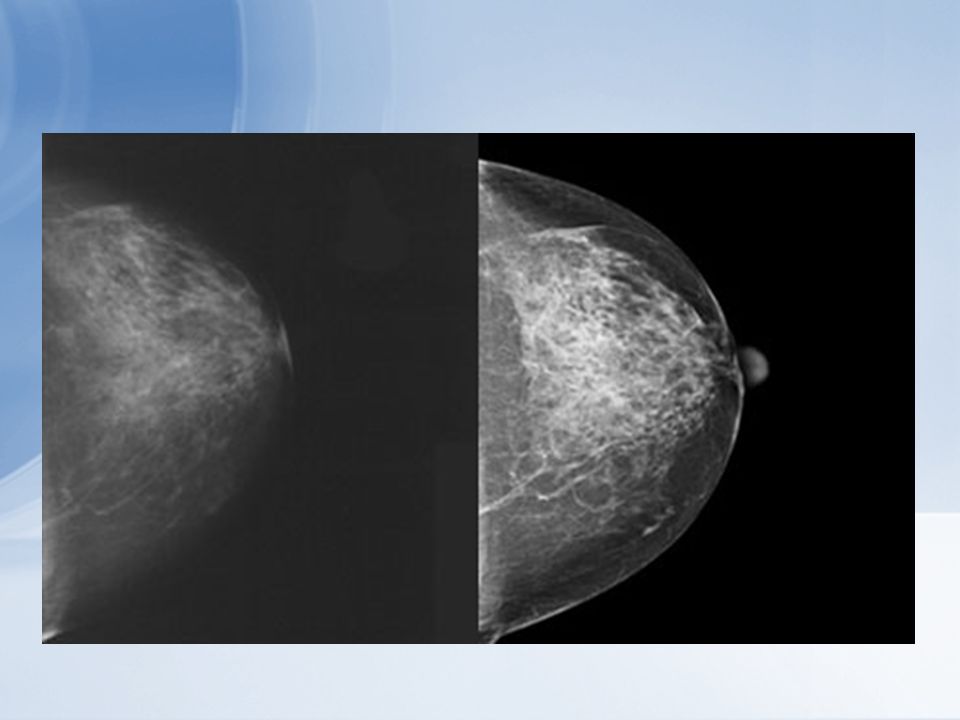
Breast cancers are most likely to develop in dense tissue, where they are most difficult to detect. Mammograms can result in false negative readings (particularly in younger women, who have dense breast tissue) or false positive readings
 or false positive readings.")
9
* Clinical history and examination * Combination imaging Mammography standard views supplementary mammographic views Local compression views magnification views ultrasound * Needle biopsy * F.N.A.C * Or core biopsy False negative rate ↓

10
Review of old films : If old films are available, comparison is important to search for any changes. It is a good idea to compare studies that are of least 2 years apart.

11
Mammography tests are not perfect. Only the part of the breast that extends from the body can be imaged. This makes it easier to get an accurate picture of a larger breast than a smaller breast ! It also may be difficult to detect abnormalities that exist in the breast tissue adjacent to the chest wall.

12
Up to 20 percent of breast cancers are missed by mammograms, according to the National Cancer Institute

13
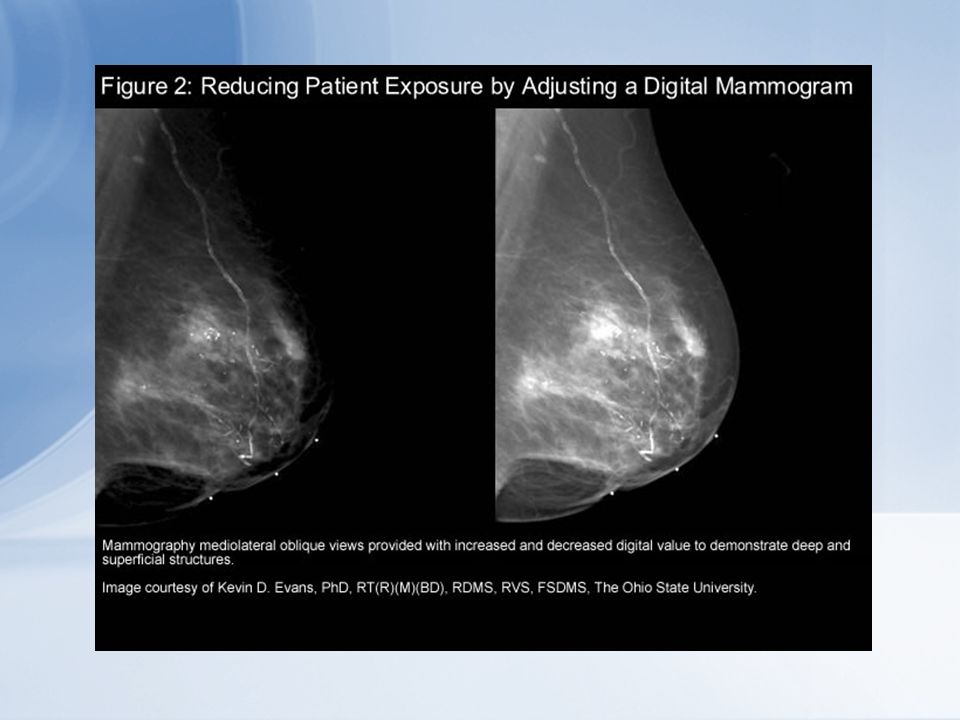
Full-field digital mammography (FFDM). This technique involves taking digital images of the breast. Digital images are captured electronically and can be viewed on a computer. Their magnification, brightness and contrast can be adjusted and enhanced to better reveal abnormalities.

14
Advantages to having digital mammography Elimination of process or artifacts Contrast enhancement Ability to perform invasive procedures faster Potentially better resolution of breast tissue for women younger than 50 years Reduce examination time for patients Increased production of examinations Images are immediately available

15
Digital Mammography Detected up to 28% More Cancers in Certain Groups: Women under the age of 50 Women with heterogeneously dense or extremely dense breast Women that are premenopausal or perimenopausal

16
Greater Access The mammogram can be read where ever the radiologist is located This also allows for physicians to consult with their peers

21
Review of Prior Images Before Procedure

24
Incomplete assessment Category 0: Additional imaging evaluation and/or comparison to prior mammograms needed. Possible abnormality may not be completely seen or defined and will need more tests, such as use of spot compression, magnification views, special mammogram views or ultrasound.

25
Complete assessment Category 1: Negative No significant abnormality to report. Breasts appear the same (symmetrical) with no masses, architectural distortion or suspicious calcifications. Category 2: Benign (Noncancerous).Also a negative mammogram, but with description of a finding known to be benign, such as benign calcifications, intramammary lymph nodes or calcified fibroadenomas. This ensures others viewing the mammogram will not misinterpret benign finding as suspicious.
 with no masses, architectural distortion or suspicious calcifications. Category 2: Benign (Noncancerous).Also a negative mammogram, but with description of a finding known to be benign, such as benign calcifications, intramammary lymph nodes or calcified fibroadenomas. This ensures others viewing the mammogram will not misinterpret benign finding as suspicious..")
26
Category 3: Probably benign - follow-up suggested, Findings have a very high probability (greater than 98%) of being benign. Findings are not expected to change. Follow- up with repeat imaging usually done in six months and regularly thereafter until finding is known to be stable (usually at least two years). Procedure helps avoid unnecessary biopsies while allowing for early diagnosis of a cancer should suspicious area change.
. Procedure helps avoid unnecessary biopsies while allowing for early diagnosis of a cancer should suspicious area change..")
27
Category 4 : Suspicious abnormality - biopsy suggested Findings could be cancer, with sufficient concern to recommend biopsy. Findings in this category have a wide range of suspicion levels. Some – though not all – physicians may divide category further: 4A: finding with low suspicion of being cancerous 4B: finding with intermediate suspicion of being cancerous 4C: finding of moderate concern of being cancerous, but not as high as Category 5

28
Category 5: Highly suggestive of malignancy – appropriate action necessary.Findings look like and have high probability (at least 95%) of being cancer. Biopsy is strongly recommended. Category 6: Confirmed Malignancy – Appropriate Action Should Be Taken.Used for findings on mammogram already determined to be cancerous by a previous biopsy.

30
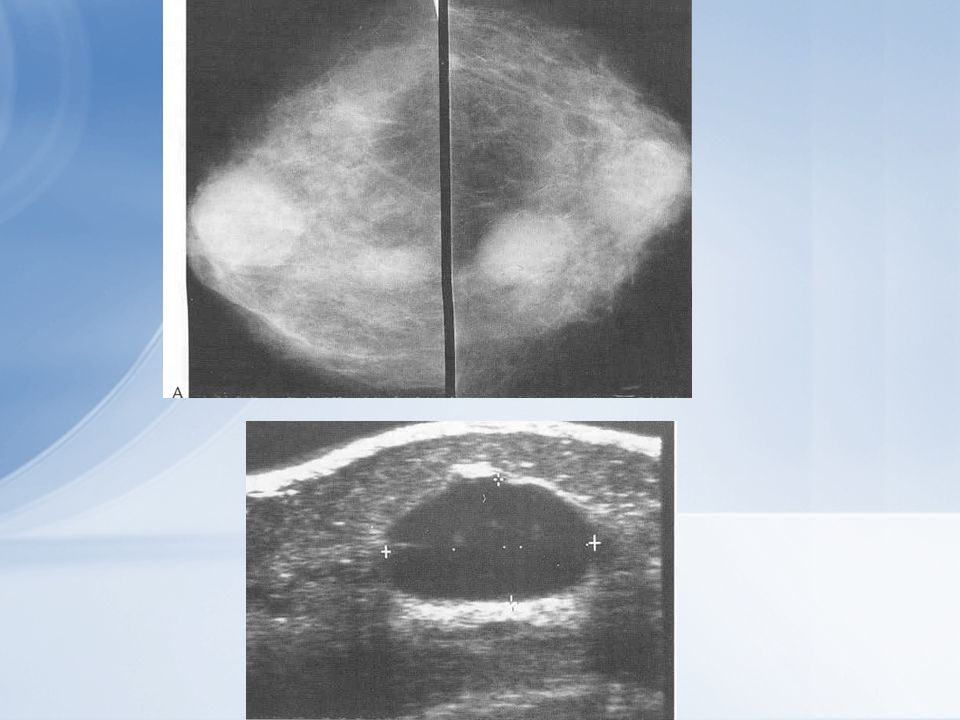
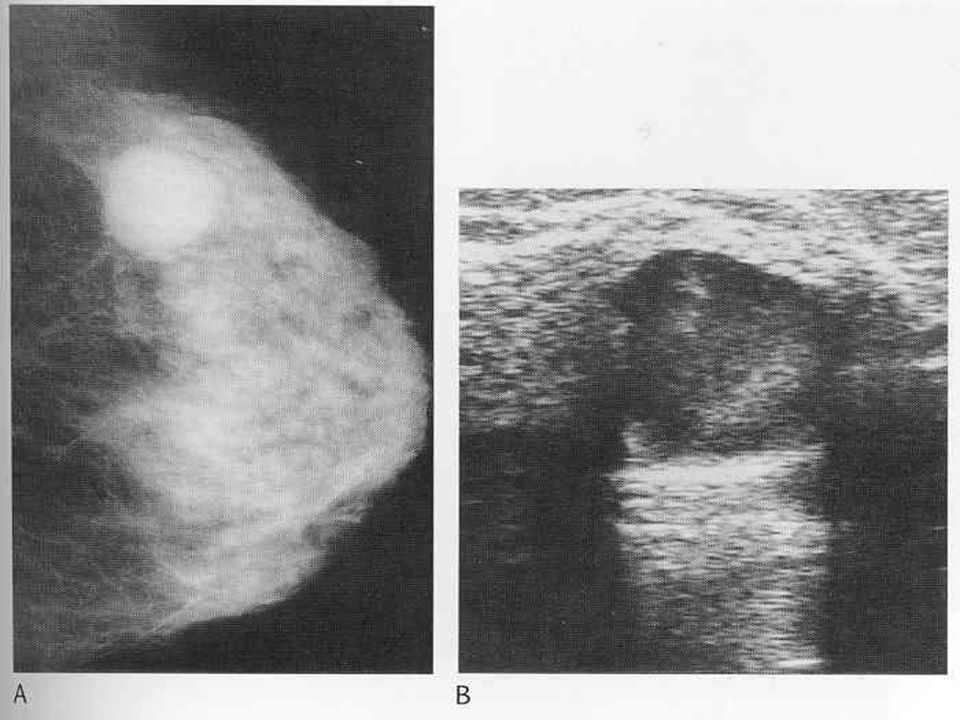
Breast ultrasound At the minimum, a 7.5 MHZ linear array probe should be used The original role of breast sonography is in the differentiation of cystic and solid lesions The role of ultrasound complements both clinical examination and mammography Ultrasound plays an important role in the triple assessment of symptomatic lesions the dense breast

31
It is the examination of choice in young women and is valuable in the assessment of mammography ‘ dense’ breast

36
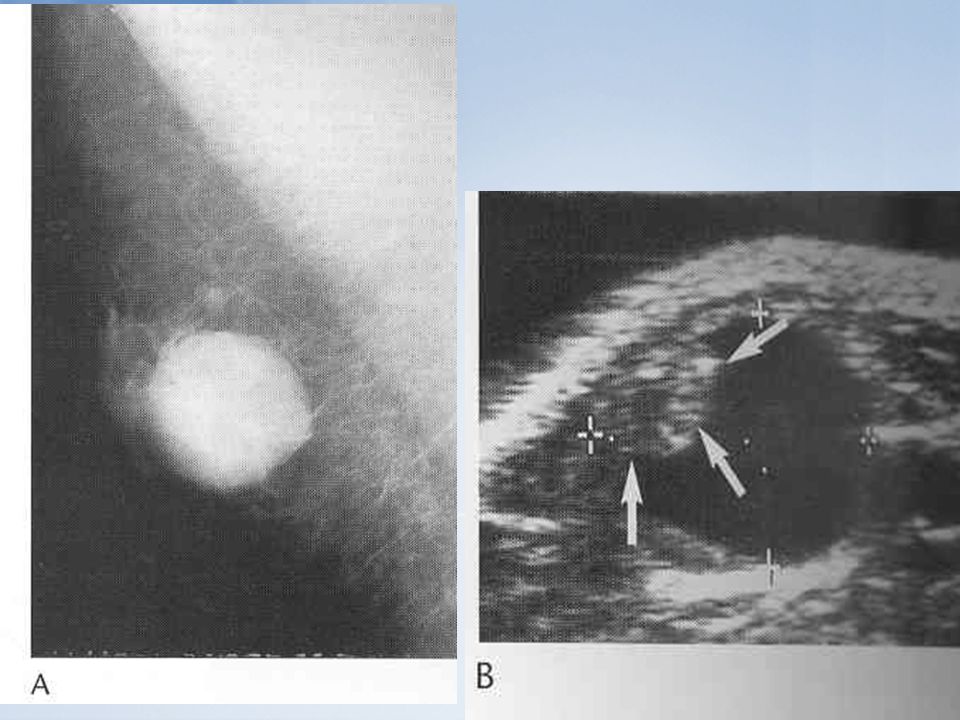
BIRADS 1 Sonographically normal tissue that cause mammographic or clinical abnormality. BIRADS 2 Benign entities (intramammary LN, ectatic duct,simple cyst,definitively benign solid such as lipoma) BIRADS 3 Probably benign( 90% risk )
 BIRADS 3 Probably benign( 90% risk ).")
37
Management Rules BIRADS 1,2 Routine screening BIRADS 3 Three choices short interval sonographic F.U image guided needle biopsy surgical biopsy BIRADS 4a,4b,5 Require biopsy

38
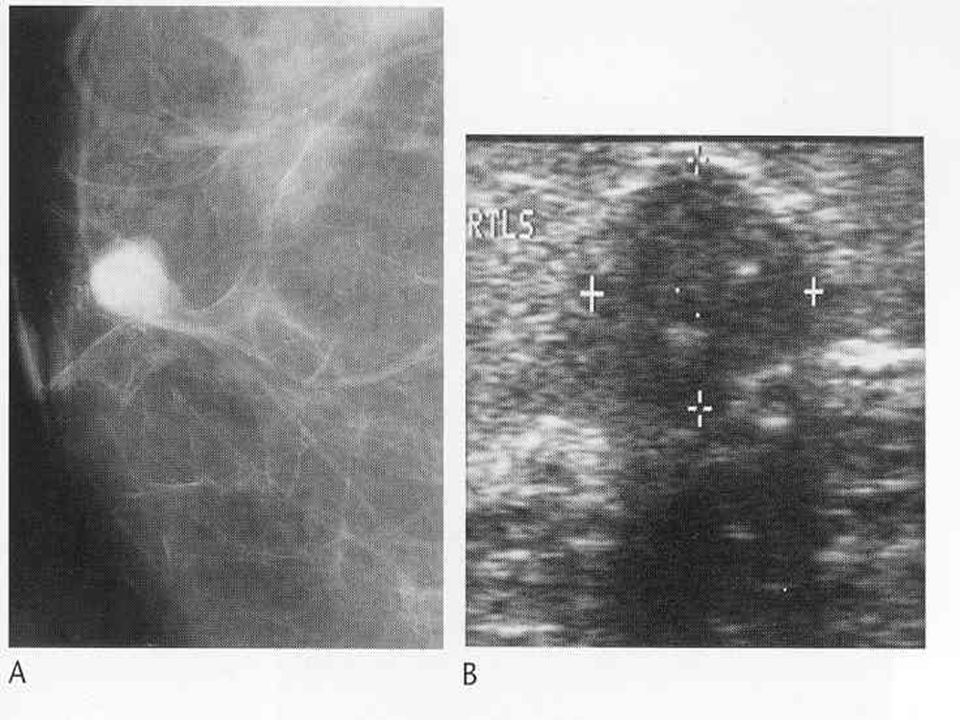
The type of imaging chosen depends principally on which method (ultrasound or mamography) shows the lesion clearly. Ultrasound is used for cysts and most soft – tissue lesions Mammography is used for microcarcification and for soft – tissue lesions that are not seen or are poorly visualized on ultrasound particularly distortions Imaging – guided practical procedures

39
Ultrasound – guided procedures 1. Cyst aspiration (simple cysts with symptoms) 2. Abscess aspiration (simple, unilocular abscess) 3. Ultrasound – guided FNAC (solid lesions) 4. Ultrasound guided core biopsy (small solid lesions)
 3. Ultrasound – guided FNAC (solid lesions) 4. Ultrasound guided core biopsy (small solid lesions).")
40
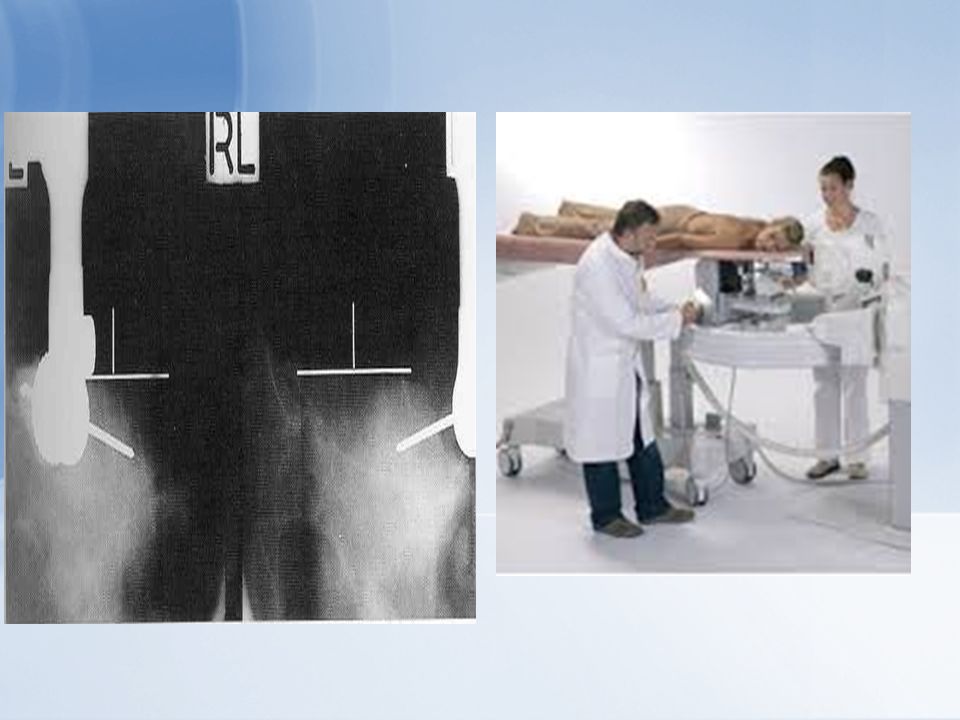
Mammography – guided procedures Stereotactic – guided FNAC or core biopsy Preoperative localization of non – palpable lesions.

42
Indication for breast MRI Clinical Indications Screening of High-Risk Women Pre-Operative Staging Contralateral Breast Cancer in Newly Diagnosed Breast Cancer Lobular Cancer Occult Breast Cancer Close or Positive Surgical Margins Post-operative Scar vs. Tumor Recurrence Neo-Adjuvant Chemotherapy Implants and Known or Suspected Cancer Problematic Mammogram Breast MRI is the technique of choice in the differentiation between postoperative scarring and local recurrence It has an important role in the assessment of the indeterminate mass because of its very high sensitivity for malignancy though at present, core biopsy is a more cost – effective approach. High Risk Screening Annual Breast MRI and Mammography Screening is Recommended for Women Who Have: BRCA1 or BRCA2 gene mutation BRCA1 or BRCA2 gene mutation First degree relative with BRCA1 or BRCA2 gene mutation and have not been tested themselves First degree relative with BRCA1 or BRCA2 gene mutation and have not been tested themselves Lifetime risk of breast cancer has been scored at 20-25% or greater, based on one of several accepted risk assessment tools that look at family history and other factors Lifetime risk of breast cancer has been scored at 20-25% or greater, based on one of several accepted risk assessment tools that look at family history and other factors Chest wall radiation between the ages of 10 and 30 at dosages above 4 Gy Chest wall radiation between the ages of 10 and 30 at dosages above 4 Gy Li-Fraumeni syndrome, Cowden syndrome, or Bannayan-Riley-Ruvalcaba syndrome, or may have one of these syndromes based on a history in a first-degree relative Li-Fraumeni syndrome, Cowden syndrome, or Bannayan-Riley-Ruvalcaba syndrome, or may have one of these syndromes based on a history in a first-degree relative 21 High Risk Screening Currently there is insufficient evidence to recommend for or against annual breast MRI screening in women who: have a lifetime risk of 15-24% as defined by several accepted risk assessment tools, such as BRACAPRO, have a lifetime risk of 15-24% as defined by several accepted risk assessment tools, such as BRACAPRO, that look at family history and other factors that look at family history and other factors have lobular carcinoma in situ (LCIS) have lobular carcinoma in situ (LCIS) have atypical ductal hyperplasia (ADH) have atypical ductal hyperplasia (ADH) have heterogeneously or extremely dense breasts on mammography (refer to first line of report) have heterogeneously or extremely dense breasts on mammography (refer to first line of report) Have a personal history of breast cancer including ductal carcinoma in situ (DCIS) Have a personal history of breast cancer including ductal carcinoma in situ (DCIS) Decisions should be made on a case by case basis. Decisions should be made on a case by case basis. 22 Clinical Indications Pre-Operative Staging Index tumor Size Index tumor Size Multi-focality or multi-centricity Multi-focality or multi- centricity Involvement of skin, pectoral muscle, chest wall Involvement of skin, pectoral muscle, chest wall Contralateral breast Contralateral breast Lymph node status Lymph node status Hematogenous metastases Hematogenous metastases 23 Clinical Indications Detection of Contralateral Breast Cancer in Newly Diagnosed Breast Cancer As many as 10% of women with breast cancer will develop a new tumor in the opposite breast with a negative mammogram and physical exam at the initial time of diagnosis. As many as 10% of women with breast cancer will develop a new tumor in the opposite breast with a negative mammogram and physical exam at the initial time of diagnosis. Finding cancers earlier may help women make treatment decision, potentially sparing additional surgery, radiation therapy and chemotherapy later. Finding cancers earlier may help women make treatment decision, potentially sparing additional surgery, radiation therapy and chemotherapy later. UW Researchers performed breast MRI on 969 patients with newly diagnosed breast cancer and detected 30 early stage tumors not detected on mammogram or physical exam * UW Researchers performed breast MRI on 969 patients with newly diagnosed breast cancer and detected 30 early stage tumors not detected on mammogram or physical exam * Memorial Sloan Kettering found contralateral breast cancer more often identified when index cancer was infiltrating lobular carcinoma **\ Memorial Sloan Kettering found contralateral breast cancer more often identified when index cancer was infiltrating lobular carcinoma **\ * NEJM 2007 vol. 356,No. 13: ** AJR 2003, vol. 180: 24 Clinical Indications Lobular Infiltrating Carcinoma Insidious cancer- Difficult to detect on Insidious cancer- Difficult to detect on mammography and physical exam Multifocal / multi-centric in up to 35% of cases and bilateral in 10% Multifocal / multi-centric in up to 35% of cases and bilateral in 10% Frequent cause of positive lumpectomy margins Frequent cause of positive lumpectomy margins 25 Clinical Indications Occult Breast Cancer About 0.3% of breast cancers present with malignant axillary lymph nodes, but normal breast exams and mammograms About 0.3% of breast cancers present with malignant axillary lymph nodes, but normal breast exams and mammograms Mastectomy standard treatment for occult malignancy Mastectomy standard treatment for occult malignancy Up to 2/3 can be localized with MRI allowing breast conservation surgery Up to 2/3 can be localized with MRI allowing breast conservation surgery 26 Clinical Indications Close or Positive Surgical Margins Up to 50% of lumpectomies have inadequate margins, requiring additional resection Up to 50% of lumpectomies have inadequate margins, requiring additional resection MRI can locate residual or additional tumor foci MRI can locate residual or additional tumor foci Applied pre-operatively, MR significantly decreases re- operations Applied pre-operatively, MR significantly decreases re-operations 27 Clinical Indications Post-operative Scar vs. Tumor Recurrence At 6 months or more after surgery At 6 months or more after surgery Mature scar, which may simulate cancer morphologically, does not enhance Mature scar, which may simulate cancer morphologically, does not enhance Recurrent tumor shows malignant-like enhancement curve Recurrent tumor shows malignant-like enhancement curve 28 Clinical Indications Neo-adjuvant Chemotherapy MRI improves the T classification as well as staging MRI improves the T classification as well as staging Can document tumor response to chemotherapy Can document tumor response to chemotherapy 29 Clinical Indications Implants and Known or Suspected Cancer MRI is not affected by implants or silicone MRI is not affected by implants or silicone Improves diagnostic confidence Improves diagnostic confidence Allows U/S guided needle biopsy prn Allows U/S guided needle biopsy prn Women with history of silicone injections can benefit from MRI screening Women with history of silicone injections can benefit from MRI screening 30 Clinical Indications Inappropriate Indications: Screening for Average Risk Women Screening for Average Risk Women Screening for Women with Less than 15% Lifetime Risk Screening for Women with Less than 15% Lifetime Risk As a Replacement for Mammography or Sonography As a Replacement for Mammography or Sonography To Biopsy or Determine the Need for Biopsy of a Suspicious Lesion Detected by Other Methods: Mammography, Ultrasound, and Physical Exam To Biopsy or Determine the Need for Biopsy of a Suspicious Lesion Detected by Other Methods: Mammography, Ultrasound, and Physical Exam 31 Accuracy Varies Considerably with Different Techniques Sensitivity: > 95-98% * Specificity: 37-97% Negative Predictive Value: > 95% Positive Predictive Value: ~ 65-75% * For DCIS sensitivity is lower, especially for low or intermediate grade lesions 32 Conclusions Bilateral, dynamic and high- spatial resolution breast MRI is widely accepted Bilateral, dynamic and high-spatial resolution breast MRI is widely accepted In the past, primarily employed as a problem-solving tool In the past, primarily employed as a problem-solving tool Now, central role in the diagnosis and staging of breast cancer Now, central role in the diagnosis and staging of breast cancer Increasing use in the treatment of breast cancer Increasing use in the treatment of breast cancer Multi-modality approach makes it work Multi-modality approach makes it work
 have lobular carcinoma in situ (LCIS) have atypical ductal hyperplasia (ADH) have atypical ductal hyperplasia (ADH) have heterogeneously or extremely dense breasts on mammography (refer to first line of report) have heterogeneously or extremely dense breasts on mammography (refer to first line of report) Have a personal history of breast cancer including ductal carcinoma in situ (DCIS) Have a personal history of breast cancer including ductal carcinoma in situ (DCIS) Decisions should be made on a case by case basis. Decisions should be made on a case by case basis. 22 Clinical Indications Pre-Operative Staging Index tumor Size Index tumor Size Multi-focality or multi-centricity Multi-focality or multi- centricity Involvement of skin, pectoral muscle, chest wall Involvement of skin, pectoral muscle, chest wall Contralateral breast Contralateral breast Lymph node status Lymph node status Hematogenous metastases Hematogenous metastases 23 Clinical Indications Detection of Contralateral Breast Cancer in Newly Diagnosed Breast Cancer As many as 10% of women with breast cancer will develop a new tumor in the opposite breast with a negative mammogram and physical exam at the initial time of diagnosis. As many as 10% of women with breast cancer will develop a new tumor in the opposite breast with a negative mammogram and physical exam at the initial time of diagnosis. Finding cancers earlier may help women make treatment decision, potentially sparing additional surgery, radiation therapy and chemotherapy later. Finding cancers earlier may help women make treatment decision, potentially sparing additional surgery, radiation therapy and chemotherapy later. UW Researchers performed breast MRI on 969 patients with newly diagnosed breast cancer and detected 30 early stage tumors not detected on mammogram or physical exam * UW Researchers performed breast MRI on 969 patients with newly diagnosed breast cancer and detected 30 early stage tumors not detected on mammogram or physical exam * Memorial Sloan Kettering found contralateral breast cancer more often identified when index cancer was infiltrating lobular carcinoma **\ Memorial Sloan Kettering found contralateral breast cancer more often identified when index cancer was infiltrating lobular carcinoma **\ * NEJM 2007 vol. 356,No. 13: ** AJR 2003, vol. 180: 24 Clinical Indications Lobular Infiltrating Carcinoma Insidious cancer- Difficult to detect on Insidious cancer- Difficult to detect on mammography and physical exam Multifocal / multi-centric in up to 35% of cases and bilateral in 10% Multifocal / multi-centric in up to 35% of cases and bilateral in 10% Frequent cause of positive lumpectomy margins Frequent cause of positive lumpectomy margins 25 Clinical Indications Occult Breast Cancer About 0.3% of breast cancers present with malignant axillary lymph nodes, but normal breast exams and mammograms About 0.3% of breast cancers present with malignant axillary lymph nodes, but normal breast exams and mammograms Mastectomy standard treatment for occult malignancy Mastectomy standard treatment for occult malignancy Up to 2/3 can be localized with MRI allowing breast conservation surgery Up to 2/3 can be localized with MRI allowing breast conservation surgery 26 Clinical Indications Close or Positive Surgical Margins Up to 50% of lumpectomies have inadequate margins, requiring additional resection Up to 50% of lumpectomies have inadequate margins, requiring additional resection MRI can locate residual or additional tumor foci MRI can locate residual or additional tumor foci Applied pre-operatively, MR significantly decreases re- operations Applied pre-operatively, MR significantly decreases re-operations 27 Clinical Indications Post-operative Scar vs. Tumor Recurrence At 6 months or more after surgery At 6 months or more after surgery Mature scar, which may simulate cancer morphologically, does not enhance Mature scar, which may simulate cancer morphologically, does not enhance Recurrent tumor shows malignant-like enhancement curve Recurrent tumor shows malignant-like enhancement curve 28 Clinical Indications Neo-adjuvant Chemotherapy MRI improves the T classification as well as staging MRI improves the T classification as well as staging Can document tumor response to chemotherapy Can document tumor response to chemotherapy 29 Clinical Indications Implants and Known or Suspected Cancer MRI is not affected by implants or silicone MRI is not affected by implants or silicone Improves diagnostic confidence Improves diagnostic confidence Allows U/S guided needle biopsy prn Allows U/S guided needle biopsy prn Women with history of silicone injections can benefit from MRI screening Women with history of silicone injections can benefit from MRI screening 30 Clinical Indications Inappropriate Indications: Screening for Average Risk Women Screening for Average Risk Women Screening for Women with Less than 15% Lifetime Risk Screening for Women with Less than 15% Lifetime Risk As a Replacement for Mammography or Sonography As a Replacement for Mammography or Sonography To Biopsy or Determine the Need for Biopsy of a Suspicious Lesion Detected by Other Methods: Mammography, Ultrasound, and Physical Exam To Biopsy or Determine the Need for Biopsy of a Suspicious Lesion Detected by Other Methods: Mammography, Ultrasound, and Physical Exam 31 Accuracy Varies Considerably with Different Techniques Sensitivity: > 95-98% * Specificity: 37-97% Negative Predictive Value: > 95% Positive Predictive Value: ~ 65-75% * For DCIS sensitivity is lower, especially for low or intermediate grade lesions 32 Conclusions Bilateral, dynamic and high- spatial resolution breast MRI is widely accepted Bilateral, dynamic and high-spatial resolution breast MRI is widely accepted In the past, primarily employed as a problem-solving tool In the past, primarily employed as a problem-solving tool Now, central role in the diagnosis and staging of breast cancer Now, central role in the diagnosis and staging of breast cancer Increasing use in the treatment of breast cancer Increasing use in the treatment of breast cancer Multi-modality approach makes it work Multi-modality approach makes it work.")
43
It is very accurate in the local staging of breast cancer in difficult cases (very dense breasts, mammographically occult tumours, suspected multi- focality or multicentricity and suspected chest wall involvement). It is the technique of choice in the evaluation of implant integrity and detection of cancer in the augmented breast. It is also accurate in the differentiation of axillary recurrence and brachial plexopathy post radiotherapy. Indication for breast MRI

44
Breast MRI appears highly accurate in the assessment of response to neoadjuvant and primary chemotherapy, predicting ulti- mate response before changes in tumour volume and differentiating between residual tumour and fibrosis. The place of breast MRI in screening high-risk patients has yet to be established Indication for breast MRI

46
Limitation of MRI Too expensive. Couldn’t find the microcalcification. Ductal Carcinoma in Situ: Intraductal carcinoma: cancer cells are confined to an intact basementmembrane: Appearances: microcalcification ( 85% ) microcalcification and mass ( 10% ) mass or architectural distortion ( 5% )
 microcalcification and mass ( 10% ) mass or architectural distortion ( 5% ).")
Similar presentations