Download presentation
Presentation is loading. Please wait.

1
Doubly bad

2
Prehospital Monday 4 th April 2011 14:23 high speed head-on MVA at Birkdale 2 patients Flail chest, severe abdo pain & pelvic # ?compound HR 120, BP 98/46 22.5mg morphine, 500mL N/S Head injury GCS 5 Failed prehospital RSI, LMA insitu Negative FAST

5
Arrival Mr MP 15:23 AIRWAY & BREATHING –Airway patent & protected –Obvious large L sided anterior flail, RR26 –Sats 96% on NRB CIRCULATION –Poor central cap refill –HR 135 BP 99/65 –Oozing compound wound over R ASIS DISABILITY –GCS 15, T35.6 TRAUMA ATTEND

6
CXR Mr MP Multiple rib # Old lung nodule

7
Pelvis Xray Mr MP

8
First venous gas Mr MP

9
Initial ED management Mr MP –FAST negative –RSI 80mg ketamine, 50mcg fentanyl & 150mg sux Gr 2 view –CT scan post (16:00)
")
10
Arrival Mr RC 15:51 AIRWAY & BREATHING –Size 5 LMA insitu –Decreased AE L side –Bilateral chest wall bruising CIRCULATION –HR 120, SBP 110 DISABILITY –Pupils 3mm, reactive –Temp 37.8

11
CXR Mr RC Increased opacification ?contusion ?aspiration Unusual mediastinum

12
Pelvis Xray Mr RC

13
First venous gas Mr RC

14
Initial ED management Mr RC FAST negative Anaesthetic team placed ETT after visualisation with bronchoscope then Pentax IDC Femoral arterial line

15
CT Mr MP

16
SPINE C7 transverse process # Wedge # T 11 (subsequently found to be old) CHEST R # ribs 1-11, L # ribs 1- 8 L sided manubrium # with retrosternal haematoma R scapular # ABDOMEN Thickening of distal ileum with stranding & small locules of adjacent free gas PELVIS Extensively comminuted # pelvis - Bilateral shattered iliac wings No pelvic extravasation contrast
 CHEST R # ribs 1-11, L # ribs 1- 8 L sided manubrium # with retrosternal haematoma R scapular # ABDOMEN Thickening of distal ileum with stranding & small locules of adjacent free gas PELVIS Extensively comminuted # pelvis - Bilateral shattered iliac wings No pelvic extravasation contrast")
17
2ndary Survey Mr MP

18
CT Mr RC

20
HEAD –DAI : Diffuse small haemorrhages –Intraventricular blood Normal C-SPINE CHEST –Multiple bilateral rib # –Pulmonary contusion/aspiration –T2 anterior column vertebral body # ABDOMEN –Hepatic contusion –?duodenal haematoma –L4 & 5 transverse process # PELVIS –Comminuted # involving L acetabulum

21
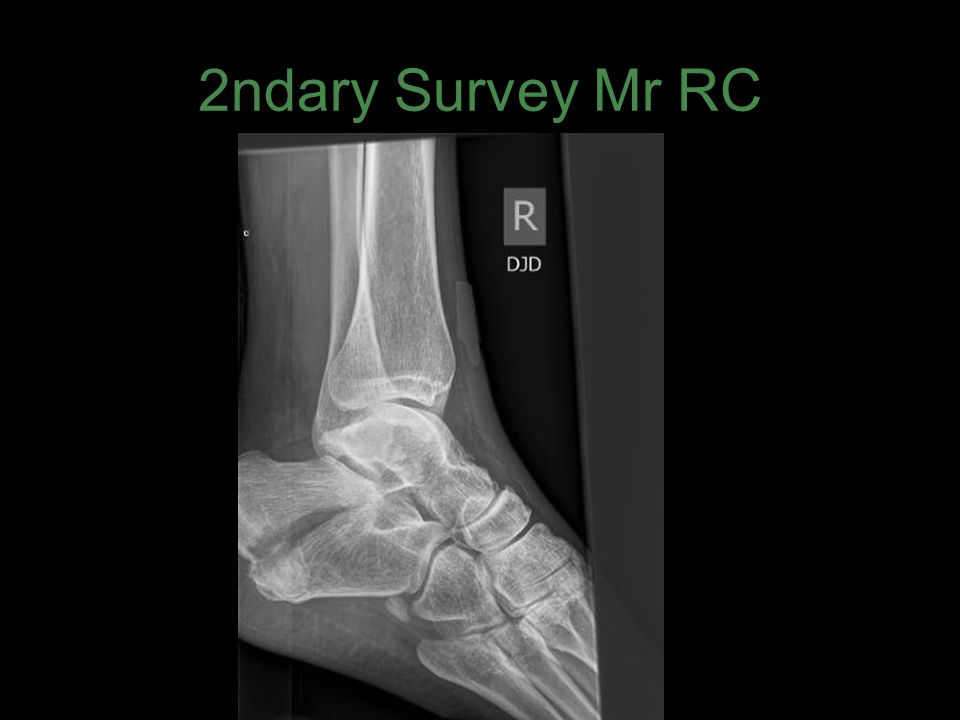
2ndary Survey Mr RC

25
Problem List Mr MP Multitrauma –Flail chest –Compound pelvis –Likely bowel injury –Stable C spine injury –Limb injuries

26
Problem List Mr MP Haemodynamic instability –?bleeding –?cardiac contusion –?SIRS

27
Disposition Mr MP OT 18:43 ED stay 3h and 20 min Specialties consulted –Trauma –Ortho –ICU –Cardiology –anaesthetics

28
Problem List Mr RC Multitrauma –Severe head injury –Chest injury –Stable spinal # –Liver and ?duodenal haematoma –Pelvis # –Multiple limb #

29
Further ED management ICP monitor placed –Initial readings 23 hypertonic saline Fluid resuscitation –3L crystalloid –4 U PRBC –2 U FFP

30
Disposition Mr RC Went to OT at 20:15, ED LOS 4h 24min Specialties consulted –Trauma –Neurosurgery –Ortho & Spinal fellow –ICU –Anaesthetics

31
Outcome Mr MP D1 – ongoing ooze: CT no active bleeding D7 – soleal vein thrombosis D9 – anterior abdominal collection OT D10 – trache D16 – line sepsis D18 – discharged to THDU D45 – discharged to GPH rehab

32
Outcome Mr RC Still inpatient Required Trache for wean Now mobilising with rollator Agitated, aggressive behaviour at times confabulating

Similar presentations






 advance ET tube B) needle thoracostomy.>")

















