Download presentation
Presentation is loading. Please wait.

1
Psychiatric Diagnoses and Their Relationship to Affirmative Defenses Bruce Wright, MD

2
Mental Illness and Mental Health Defenses: Perceptions of the Criminal Bar Frierson, et al Journal of the American Academy of Psychiatry & the Law 43: 483-91, 2015

3
Which of the following is the correct definition of PSYCHOSIS? 1.Loss of contact with reality 2.Rapidly shifting mood states 3.Repetitive behavior such as counting or hand- washing 4.Loss of contact with reality; persistent and extreme elevation in mood

4
Which of the following is the correct definition of a DELUSION? 1.A false belief firmly held by the patient despite evidence to the contrary. 2.A false sensory perception, such as seeing or hearing things that are not present. 3.Impairment of thinking where a patient becomes disoriented to time, place, or events 4.A rapid succession of fragmentary thoughts or speech in which content changes abruptly

5
Which of the following is the most severe and chronic mental illness? 1.Major depression 2.Bipolar disorder 3.Schizophrenia 4.Obsessive-compulsive disorder

6
What is the definition of? 1.Not Guilty by Reason of Insanity 2.Guilty But Mentally Ill

7
Psychiatric Diagnoses Guide Treatment Prognosis Research Forensic issues - ?????

8
Diagnoses are assigned if the symptoms are consistent with the DSM criteria Psychiatric Diagnoses do not identify a specific etiology

9
DSM I1952 106 Diagnoses 130 pages DSM II1968 ↓↓ DSM III1980 DSM IV1994 DSM 52013 757 Disorders 947 pages

10
What is Different about DSM 5? 1.Digit not Roman numeral 2.Multi-axial diagnostic system 3.Some diagnoses have changed names

11
Dementia Major Neurocognitive Disorder Minor Neurocognitive Disorder Mental Retardation Intellectual Disability

12
Judge Scalia – US Supreme Court: They changed their mind, counsel. This APA is the same organization that once said that homosexuality was a mental disability and now says it’s perfectly normal. They change their minds. Hall v Florida, 2014

13
Criticism of the DSM - 5 1.Just a money maker for the APA

14
Criticism of the DSM - 5 1.Just a money maker for the APA 2.Blurs the line between normal and pathological

15
Normal vs Pathological Examples include: 1.Normal grief may be diagnosed as Major Depression 2.Behavioral addiction ( ex: internet gaming disorder) 3.Gluttony (binge eating 12x’s in 3 months) is diagnosable 4.Mild neurocognitive disorder = benign forgetfulness 5.Childhood temper tantrums = disruptive mood dysregulation disorder 6.Female vs. Male sexual disorder

16
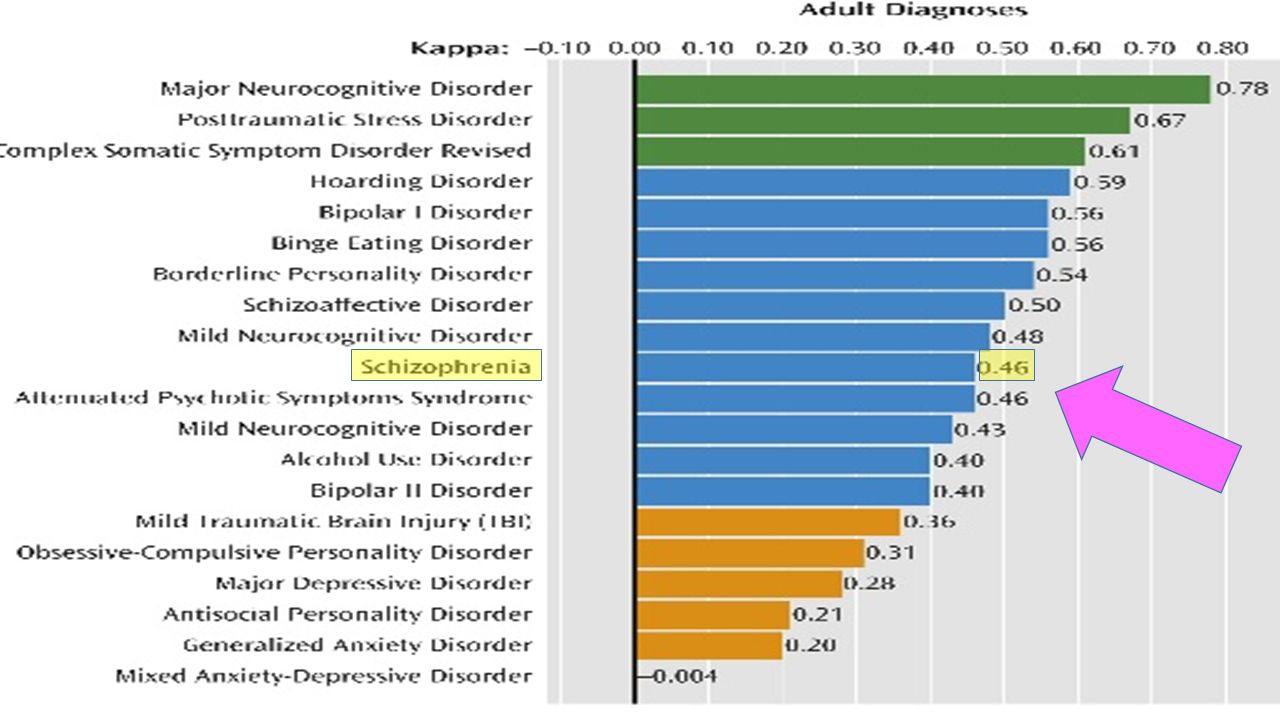
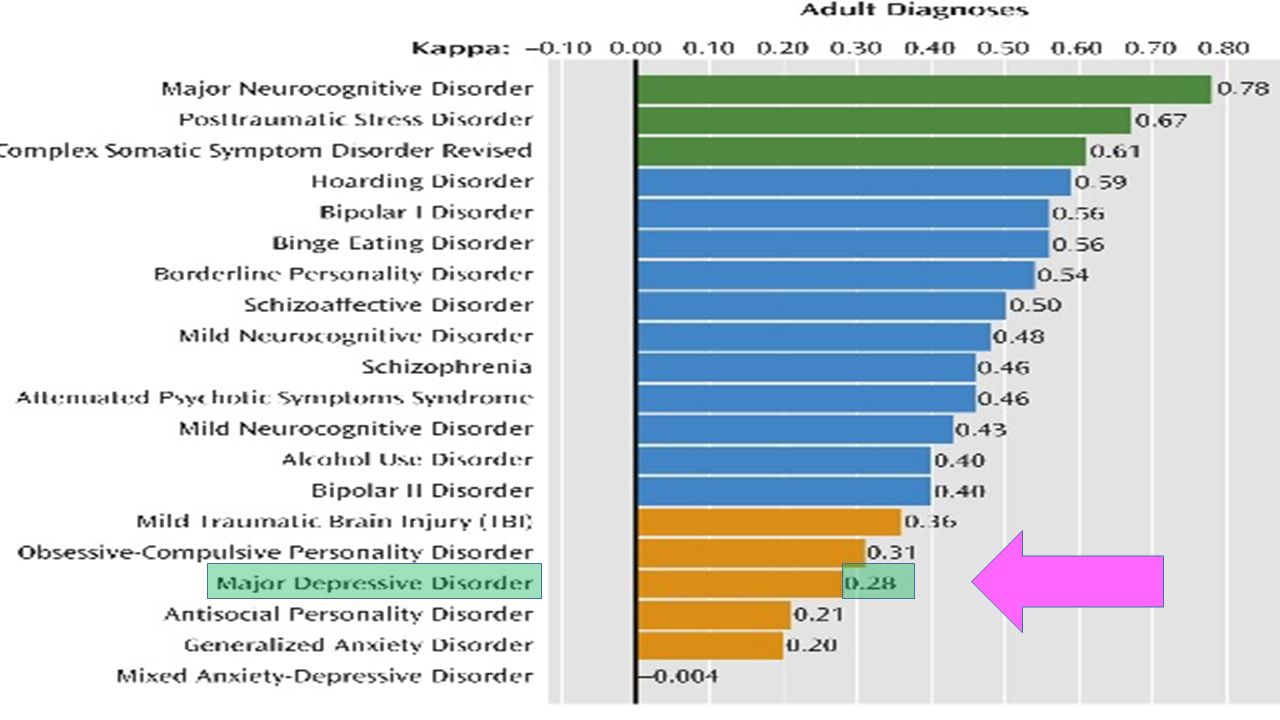
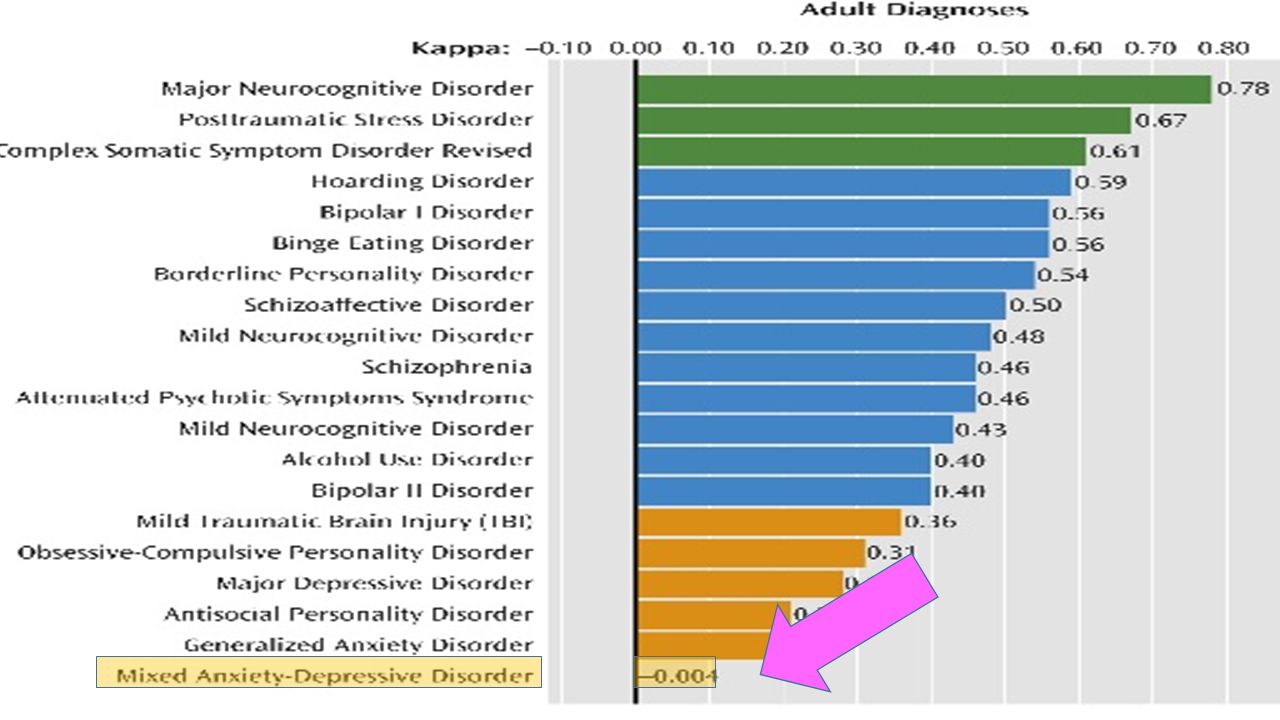
Criticism of the DSM - 5 1.Just a money maker for the APA 2.Blurs the line between normal and pathological 3.Significant problems with inter-rater reliability

17
The Initial Field Trials of DSM-5: New Blooms and Old Thorns Freedman, et al The American Journal of Psychiatry, 2013

18
The Initial Field Trials of DSM-5: New Blooms and Old Thorns Kappa Coefficient (K)
")
22
Causes of inter-rater reliability problems: Examiner’s questions Individual’s answers Available history and collateral information We don’t have diagnostic tests or imaging to confirm diagnoses

23
Delusions Hallucinations Formal Thought Disorder

24
PSYCHOSIS delusions formal thought disorder hallucinations

25
Psychosis seen with: Schizophrenia Schizoaffective disorder Delusional Disorder Mood Disorder with psychosis (Major Depression, Bipolar) Delirium Intoxication/Withdrawal others
 Delirium Intoxication/Withdrawal others")
26
Definition of Personality Disorder Enduring pattern of inner experience and behavior that deviates from cultural expectations Inflexible and Pervasive Cognitive, Affective, Behavioral, or Interpersonal manifestations

27
Cluster A: (ODD) Paranoid Schizoid Schizotypal Cluster B: (DRAMATIC) Antisocial Borderline Histrionic Narcissistic Cluster C: (ANXIOUS) Avoidant Dependent Obsessive Compulsive
 Paranoid Schizoid Schizotypal Cluster B: (DRAMATIC) Antisocial Borderline Histrionic Narcissistic Cluster C: (ANXIOUS) Avoidant Dependent Obsessive Compulsive")
28
DSM-5 CAUTIONARY STATEMENT When DSM-V categories, criteria, and textual descriptions are employed for forensic purposes, there is a risk that diagnostic information will be misused or misunderstood. These dangers arise because of the imperfect fit between the questions of ultimate concern to the law and the information contained in a clinical diagnosis. In most situations, the clinical diagnosis of a DSM-V mental disorder such as intellectual disability (intellectual development disorder), schizophrenia, major neurocognitive disorder, gambling disorder, or pedophilic disorder does not imply that an individual with such a condition meets legal criteria for the presence of a mental disorder or a specified legal standard (e.g. for competence, criminal responsibility, or disability).
, schizophrenia, major neurocognitive disorder, gambling disorder, or pedophilic disorder does not imply that an individual with such a condition meets legal criteria for the presence of a mental disorder or a specified legal standard (e.g. for competence, criminal responsibility, or disability)..")
29
DSM-5: Challenging Diagnostic Testimony Hagan, et al International Journal of Law and Psychiatry, 2015

30
Expert testimony re: the diagnosis (although it might be interesting) is irrelevant in most legal cases
 is irrelevant in most legal cases")
31
The expert opinion must address how that psychiatric illness (or disease of the mind) affects the individual’s thoughts processes, cognitive capacity, and behavior.
 affects the individual’s thoughts processes, cognitive capacity, and behavior.")
32
What is the one exception? 2002 US Supreme Court Atkins v. Virginia The execution of mentally retarded criminals violated the Eight Amendment prohibition of cruel and unusual punishment.

33
The definition of MR/ID has changed with time DSM INO IQ PARAMETERS DSM IIIQ = 52-67 DSM IIIIQ BETWEEN 50 - 70 DSM IVHIGH OF APPROXIMATELY 70 DSM 5IQ NOT INCLUDED IN DIAGNOSTIC CRITERIA

34
Insanity Diminished Capacity GBMI

35
Judge David Bazelon, 1954 United State Court of Appeals “Our collective conscience does not allow punishment where it cannot impose blame.”

36
1.Did the defendant suffer from a mental disorder at the time of the alleged crime? 2.Was there a relationship between the mental disorder and the criminal behavior? 3.If so, were the criteria met for the jurisdiction’s legal test for being found not criminally responsible?

37
Insanity Diminished Capacity GBMI

38
Pre-M’Naghten 1723 -- WILD BEAST TEST A man must be…totally deprived of his understanding and memory, and doth not know what he is doing, no more than an infant,…a brute, or a wild beast… before being found insane.

39
Pre-M’Naghten 1840 - IRRESISTIBLE IMPULSE TEST For a person to be acquitted, as a result of a mental disorder, he could not resist the impulse to commit the crime.

40
1843 - M’Naghten Every man is presumed to be sane….To establish a defense on the grounds of insanity, it must be proved that, at the time of the committing of the act, the party was laboring under such a defect of reasoning from a disease of the mind as to not know the nature or quality of the act he was doing, or, if he did know, he did not know it was wrong

41
M’Naghten DEFECT OF REASONING FROM A DISEASE OF THE MIND DID NOT KNOW THE NATURE AND QUALITY OF THE ACT or DID NOT KNOW THE ACT WAS WRONG

42
Post M’Naghten 1870 – PRODUCT TEST aka DURHAM TEST: No man shall be held accountable, criminally, for an act which was the offspring and product of a mental disease.

43
Post M’Naghten 1955 - MODEL PENAL CODE A person is not responsible for criminal conduct if at the time of such conduct as a result of mental disease or defect he lacks substantial capacity either to appreciate the criminality of his conduct or to conform his conduct to the requirements of law.

44
Post Hinckley 1984 - Insanity Defense Reform Act A defendant will be found not guilty by reason of insanity if, as a result of severe mental disease or defect, he was unable to appreciate the nature and quality or the criminality or wrongfulness of his acts.

45
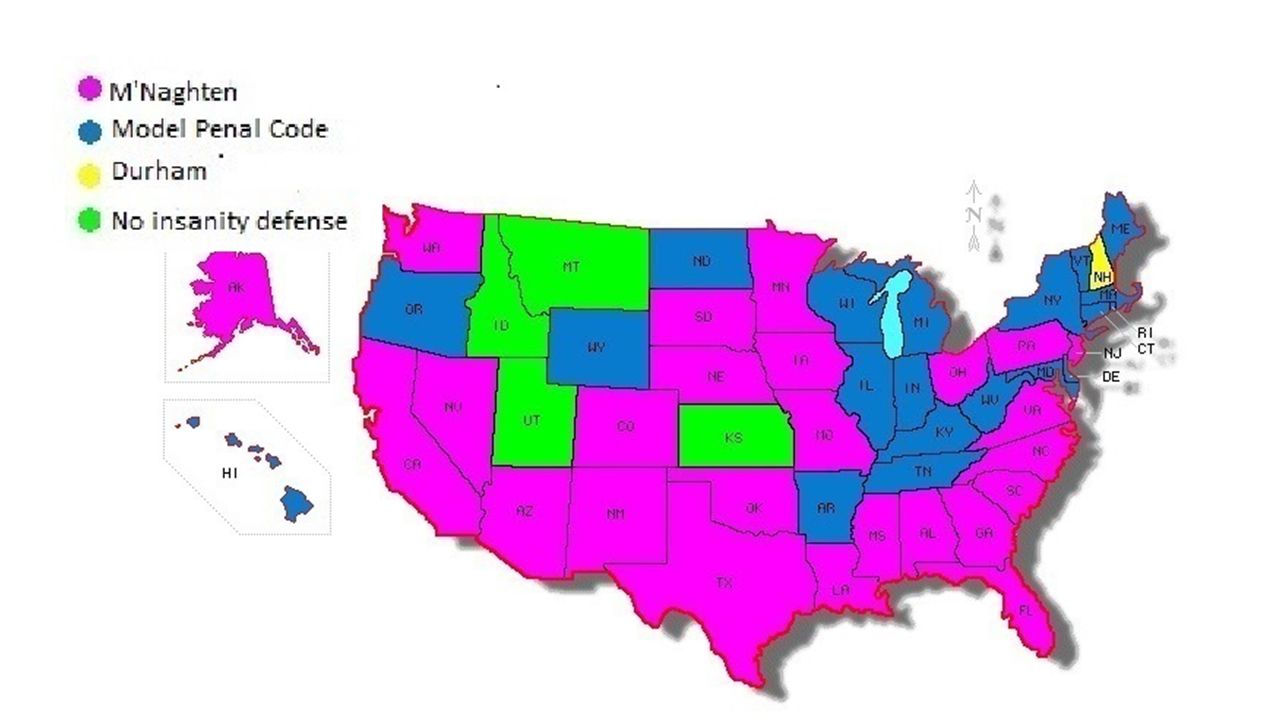
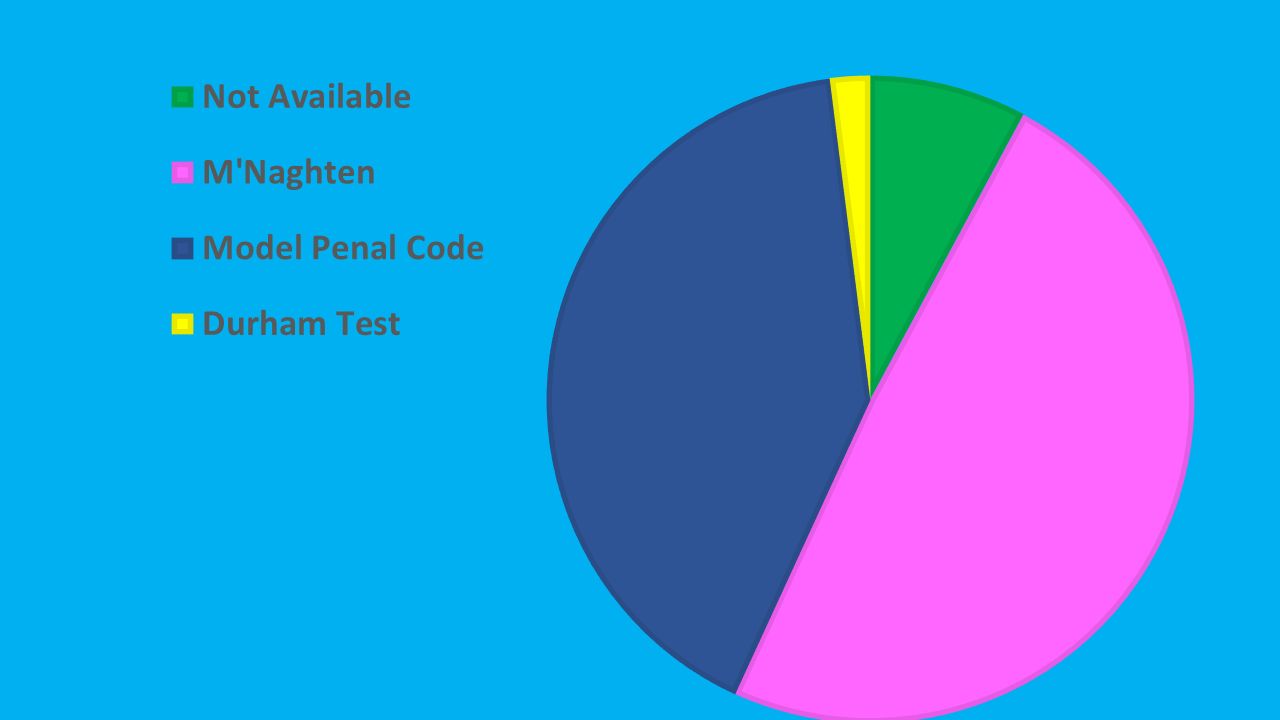
M’Naghten Durham – Product Test Model Penal Code Insanity Defense Reform Act

48
The Insanity Defense Reform Act of 1984: Much Ado About Nothing Finkel Behavioral Sciences and the Law, 1989

49
US v Freeman 1966 The determination whether a man is or is not held responsible for his conduct is not a medical, but a social or moral judgement. Ideally, the psychiatrist, much like experts in other fields, should provide grist for the legal mill, should furnish the raw data upon which the legal judgement is based. It is the psychiatrist who informs as to the mental state of the accused, his characteristics, his potentialities, his capabilities.

50
PENNSYLVANIA -- M’Naghten DEFECT OF REASONING FROM A DISEASE OF THE MIND DID NOT KNOW THE NATURE AND QUALITY OF THE ACT or DID NOT KNOW THE ACT WAS WRONG

51
Which psychiatric diagnoses qualifiy for the M’Naghten defense? Dementia Schizophrenia Major Depression Delirium Alcohol Intoxication

52
INSANITY is not in the DSM-5

53
INSANITY EVALUATION Particular attention to: Mental state at the time of the offense o Cognitive o Psychotic Behavior at the time of the offense Motive Planning and preparation Ability to complete other deliberate acts Ability to control behavior Knowledge of wrongfulness

54
Insanity evaluation Ground for suspicion: 1.Efforts at flight 2.Efforts at concealment of the crime 3.Efforts at concealment of evidence

55
Insanity Diminished Capacity GBMI

56
First Degree murder requires: 1.The victim is dead 2.The defendant killed him 3.The defendant did so with a SPECIFIC INTENT TO KILL and with malice Diminished Capacity

57
Diminished capacity is not available where the defendant denies committing the act

58
Diminished Capacity Specific intent to kill – does not require planning or previous thought or any particular length of time; all that is required is that the defendant formed the intent to kill and is conscious of his intentions

59
Diminished Capacity Commonwealth v Logan: Specific intent to kill means that the killer plans and carries out the act to advance his or her own desire and that he or she knows that act will result in the death of another

60
Diminished Capacity Psychiatric testimony must speak to the MENTAL DISORDER affecting cognitive functions necessary to from a specific intent to kill

61
Diminished Capacity Commonwealth v Zettlemoyer 1982 Testimony is irrelevant unless it speaks to mental disorders affecting the cognitive functions of deliberation and premeditation necessary to formulate a specific intent to kill Testimony that speaks to irresistible impulse or inability to control self would be irrelevant Must ask about whether the defendant had the capacity to kill rather than whether he had the intent to kill

62
Diminished Capacity Commonwealth v Vandivner, 2009 An inability to control actions, or impulsive acts are irrelevant to specific intent to kill and not admissible to support diminished capacity

63
Insanity Diminished Capacity GBMI

64
GBMI: “The defendant LACKS SUBSTANTIAL CAPACITY either to APPRECIATE the wrongfulness of what he is doing or to conform his conduct to the requirements of the law”

65
Other considerations: 1.Voluntary intoxication 2.Involuntary intoxication 3.Heat of passion 4.Battered woman syndrome

66
Other considerations: MALINGERING – the voluntary production of symptoms for an identifiable goal

67
Interview Techniques for Suspected Malingerers: 1.Always suspect malingering -- Especially in forensic settings 2.Do your homework 3.Look for unusual/rare/unique symptoms 4.Start with non-related subjects

68
SUMMARY: Psychiatric diagnoses Mental health issues pertaining to Insanity, Diminished Capacity, GBMI

Similar presentations








 Forensic psychiatry is a branch of medicine which focuses on the interface.>")




 Paranoid Personality Disorder Schizoid Personality Disorder Cluster B (Dramatic-Impulsive Cluster)>")



 –Conform his.>")

