Download presentation
Presentation is loading. Please wait.

1
Subclinical Thyroid Disease: Where Are We Now Dr Praveen Shankar MD, MRCP(UK)
")
2
Definitions Subclinical Disease The presence of a disease without obvious symptoms Usually indicates early stage in evolution of a disease Subclinical thyroid disease A biochemical diagnosis Subclinical hyperthyroidism ↓ TSH ↔ FT4 & TT3 Subclinical hypothyroidism ↑TSH ↔ FT4 & TT3.

3
How does Subclinical Thyroid Disease develop? TSH secretion is very tightly controlled by T4 & T3 Very small changes in serum T4 & T3 concentrations have large effects on TSH secretion Log/linear relationship between serum TSH & FT4 – alterations in serum FT4 that is within normal range can cause increase/decrease in serum TSH concentrations that can be outside its reference range. JCEM 2002; 87: 1068–72 JCEM2004; 89: 1181–87.

4
Subclinical Hyperthyroidism With mildly suppressed TSH concentrations (TSH 0.1 to 0.4 mU/L) With completely suppressed TSH concentrations (TSH < 0.1 mU/L) With progressive decline in TSH level chances of clinically significant consequences rises In any population mild subclinical hyperthyroidism is more common The population prevalence of subclinical hyperthyroidism higher in o Women o Old age o Geographical region with iodine-deficiency.
 With completely suppressed TSH concentrations (TSH < 0.1 mU/L) With progressive decline in TSH level chances of clinically significant consequences rises In any population mild subclinical hyperthyroidism is more common The population prevalence of subclinical hyperthyroidism higher in o Women o Old age o Geographical region with iodine-deficiency.")
6
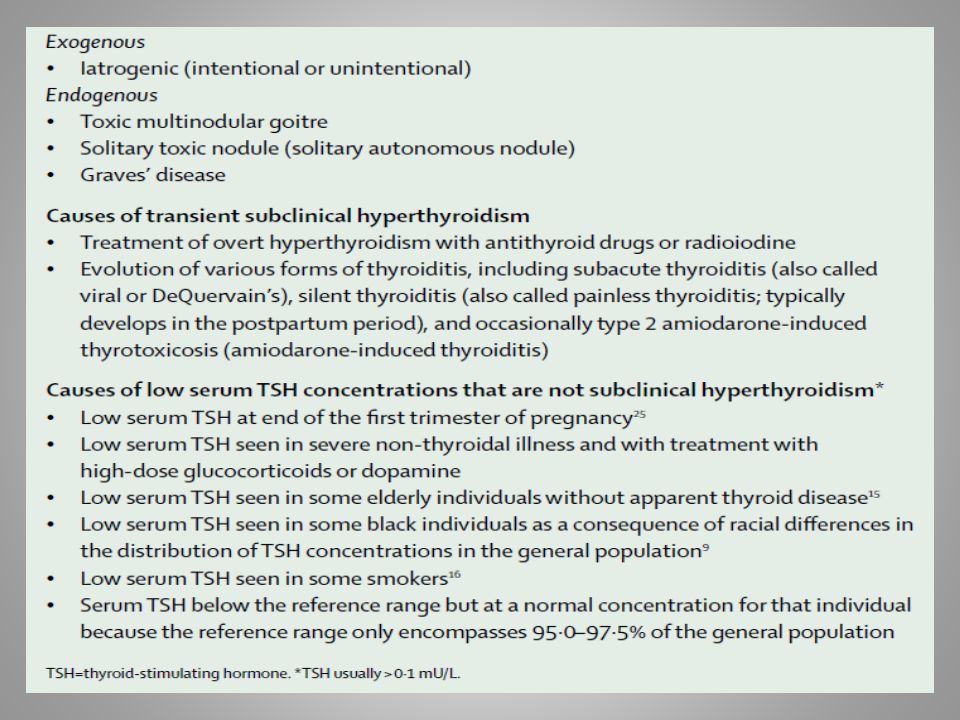
Subclinical Hyperthyroidism Exogenous disease more common than endogenous form o 20-40% of patients on LT4 replacement have low TSH concentration o Reversible on lowering doses Graves’ disease is the most common cause in young patients Toxic adenoma/MNG most common cause in elderly MNG is more typically associated with subclinical hyperthyroidism than Graves’ disease In one study, about 20% of patients with Graves’ disease had a chronically suppressed TSH after a course of ATD or surgery, and were more likely to relapse than a comparable group with normal TSH levels. Acta Endocrinol (Copenh) 1990; 122: 623.
 1990; 122:")
7
Progression to overt hyperthyroidism in people with completely suppressed TSH concentrations is higher Am J Med Sci 2009; 337: 225–32.

8
www.thelancet.com Published online January 23, 2012 DOI:10.1016/S0140- 6736(11)60276-6. Natural History

9
Systemic effects Similar to that of overt hyperthyroidism Bone & mineral metabolism ↑ bone resorption Cortical bone is affected more than trabecular bone ↓BMD in postmenopausal women, but, little effect in men or premenopausal women ?Whether this translates into increased risk of fracture in postmenopausal women. Atrial fibrillation ↑ risk Risk similar whether TSH <0.1 or 0.1-0.4 mU/L Prevalence similar to that in overt hyperthyroidism May remit with ATD therapy.

10
Systemic effects Cardiovascular system ↑ heart rate & atrial premature beats ?↑LV mass Changes in coagulation indicators ↑carotid intima-media thickness ↑atherosclerotic CV events & CV morbidity & mortality especially in elderly patients & those with underlying cardiac disease Cognitive dysfunction & quality of life Associated with dementia in elderly people Palpitations, heat intolerance & anxiety cause reduction in quality-of-life scores.

11
Prevention of Exogenous subclinical hyperthyroidism important Cause substantial morbidity especially in older patients o ↓BMD o ↑risk of AF Important to carefully titrate LT4 doses to maintain normal TSH level in those on replacement therapy TSH suppressive therapy to decrease goitre or thyroid nodule size is no longer recommended Less aggressive TSH suppression has been suggested for patients o With low-risk thyroid cancer o Older patients who have been shown to be disease-free on follow up. Thyroid 2009; 19: 1167. Thyroid 2010; 20: 135.

12
TSH <0.1 mU/LTSH 0.1-0.4 mU/L HIGH-RISK PATIENTS Postmenopausal women who are not on oestrogen or bisphosphonates Patients with osteoporosis Patients with cardiac disease Elderly (age >65 years) Treatment recommended Consider treatment LOW-RISK PATIENTS Postmenopausal women who are on oestrogen or bisphosphonates Patients <65 years with no comorbidities Consider treatment Treatment unnecessary SYMPTOMATIC PATIENTSTreatment recommended Consider treatment Werner & Ingbar’s The Thyroid- A Fundamental and Clinical Text 10 th Edition: p520. Who deserve treatment?

13
www.thelancet.com Published online January 23, 2012 DOI:10.1016/S0140-6736(11)60276-6.
")
14
Subclinical hypothyroidism Biochemical diagnosis, by definition can not be identified on the basis of signs & symptoms Consensus lacking on the upper limit of normal for serum TSH National Academy of Clinical Biochemistry Laboratory Practice Guidelines, 2003 recommendation (endorsed by AACE ) – 2.5 mU/L Present data support the need for age-based normal ranges for serum TSH Consideration of TSH measurement method is important – Immunometric assay (IMA) using nonisotopic (chemiluminescent or fluorescent ) technique (3 rd generation) commonly give upper limit of normal as less than 4.5 mU/L.
 – 2.5 mU/L Present data support the need for age-based normal ranges for serum TSH Consideration of TSH measurement method is important – Immunometric assay (IMA) using nonisotopic (chemiluminescent or fluorescent ) technique (3 rd generation) commonly give upper limit of normal as less than 4.5 mU/L.")
15
TSH distribution curve shifts to higher TSH concentrations with age (NHANES III & NHENES 1999-2002 databases for thyroid disease-free subjects) Potential for misclassification of older individuals as having subclinical hypothyroidism if age-specific TSH cut-off values not employed JCEM 2007; 92: 4575-82.
 Potential for misclassification of older individuals as having subclinical hypothyroidism if age-specific TSH cut-off values not employed JCEM 2007; 92:")
16
Prevalence Higher in o ? Old age o White compared to black o Area with higher compared to lower, but not deficient, intake of iodine o Patients with Down syndrome, Turner’s syndrome, T1DM & possibly other autoimmune diseases, family history of autoimmune thyroid disease, endocrine or systemic autoimmune disorders In a survey of pregnant women in the US, 2% had subclinical hypothyroidism and 58% had high anti-TPO antibody concentration.

19
JCEM 2002; 87: 3221-3226.

20
Natural History

21
Systemic effects Cardiovascular effects Subclinical hypothyroidism is associated with hypercholesterolemia, atherosclerosis and other CV changes like ↑SVR & arterial stiffness, altered endothelial function & coagulability ? Do they -result in adverse cardiovascular events: Conflicting data A meta-analysis of individual participant data done by Thyroid Studies collaborators o 11 prospective cohort studies o Total no. of participants 55,287 o Subclinical hypothyroidism was defined as TSH between 4.5 to 20 mU/L with normal T4 concentration.

22
The risk of CHD events & CV mortality, but not total mortality, increased significantly with TSH ≥ 10 mU/L

23
Women of reproductive age and during pregnancy Prevalence is 0.5-5% depending on the cut-off value for TSH used to define the condition Associated with serious obstetric complications- increased risk of miscarriage, placental abruption, preterm delivery, gestational HTN, LBW Thyroid hormone essential for fetal brain development & maturation especially during 1 st trimester of pregnancy Impaired mental development has been reported in children born to women who were inadequately treated for subclinical hypothyroidism The Endocrine Practice guidelines recommends treatment of subclinical hypothyroidism in pregnancy. NEJM 1999; 341: 549-55. JCEM 2012; 97:2543-65.

24
Neuropsychiatric health It seems patients with autoimmune thyroid disease (majority will be subclinical hypothyroidism) have increased propensity towards depression Patients with depression and subclinical hypothyroidism compared to those with depression & euthyroidism have o Higher prevalence of associated panic disorder o Poorer response to antidepressant drug therapy. Werner & Ingbar’s The Thyroid- A Fundamental and Clinical Text 10th Edition: p632.

25
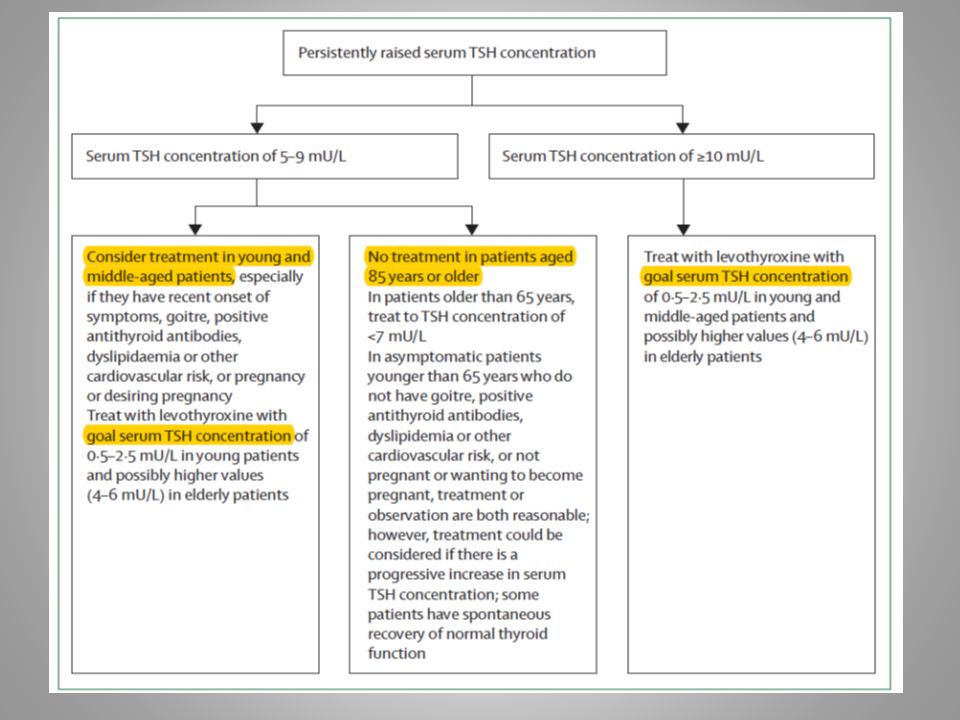
Who would need replacement?

27
Please remember… …

Similar presentations