Download presentation
Presentation is loading. Please wait.

1
Dr Ben McKenzie Emergency Physician

2
13 year old girl Drinking with friends to see who could take the most panadol and aspirin. Took maybe 60 tablets, 12 aspirin 2 days ago Presents with RUQ pain and vomiting

3
Yes this is a real case! Increasing pill parties in USA....

4
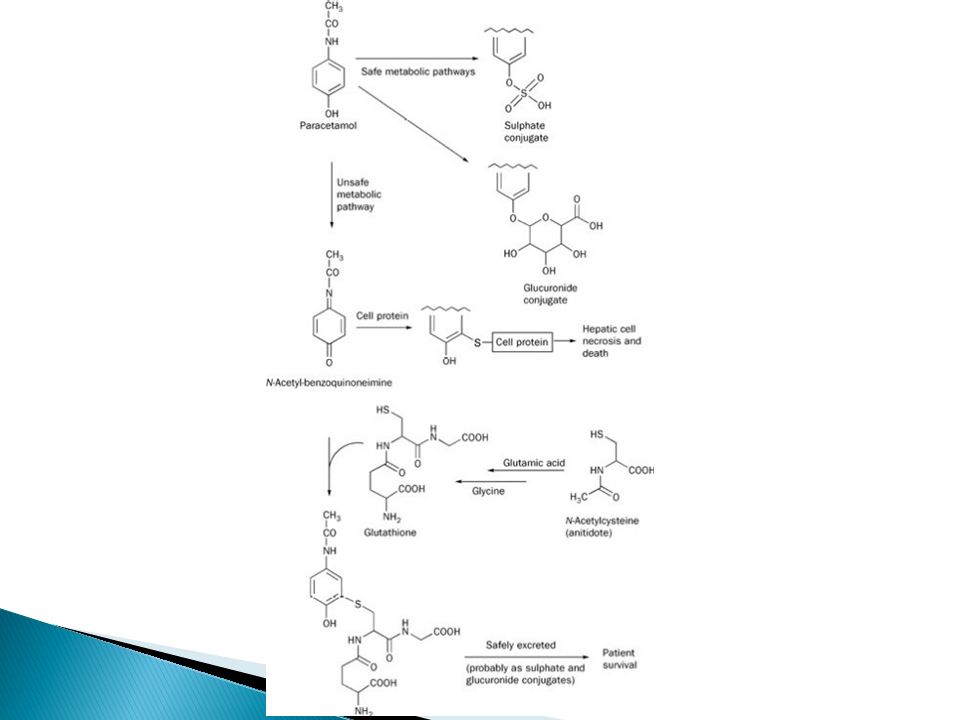
90% conjugated and excreted in urine ◦ Conjugated with sulfate ◦ Conjugated with glucuronide 2% excreted unchanged in urine Rest metabolised by cytochrome P450 mixed function oxidase system (CYP2E1, CYP1A2, CYP3A4) ◦ Forms N-acetyl-p-benzoquinoneimine (NAPQI) ◦ NAPQI is TOXIC!! But luckily is conjugated with Glutathione in the liver under in therapeutic doses of paracetamol.

5
Once sulfation and gluronidation pathways are saturated metabolism is shunted down the CYP450 pathway of oxidation. One glutathione is depleted then NAPQI accumulates. NAPQI starts binding hepatic cells proteins and cell death.

7
When there is overdose If induction of CYT P450 enzymes ◦ Carbamazepine and phenytoin use induce CYP2E1 ◦ Malnourished – less glutathione stores. ◦ Alcoholics with repeated paracetamol insults Induced CYP450 enzymes Malnourished, fasting Not increased risk with single overdose

8
In children under 5 ◦ More conjugation and more glutathione stores

9
<150mg/kg in adults or 7-10g toxicity unlikely <200mg/kg in children toxicity unlikely > 350mg/kg Most patients develop hepatoxicity

10
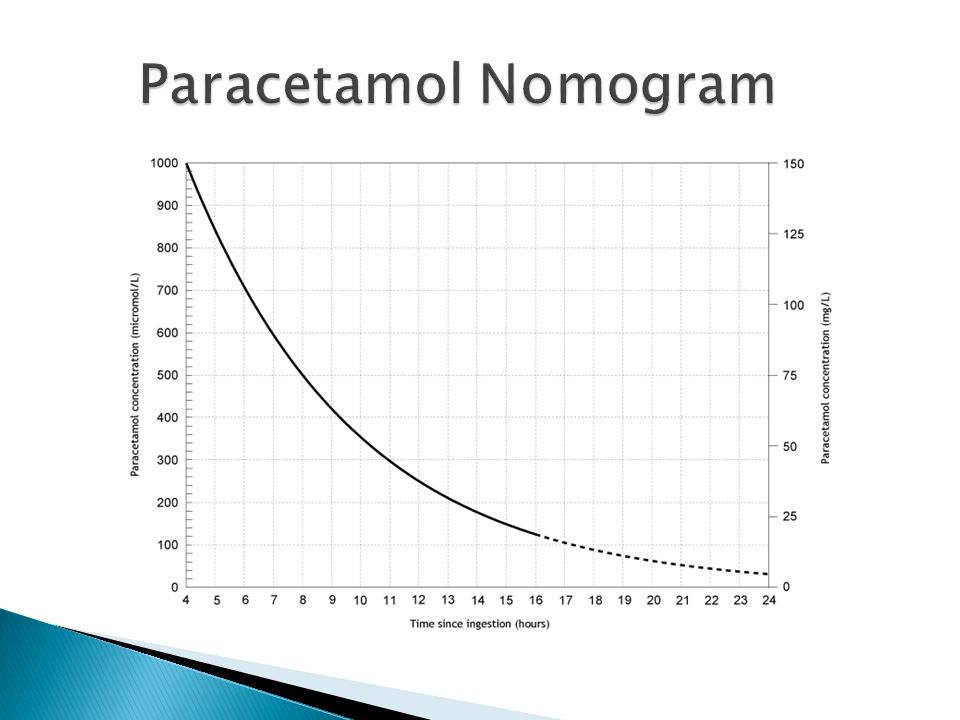
Rumack-Matthew Nomogram was the original plotted graph of untreated patients paraectamol concentration against time. 60% above the line developed hepatoxicity. This has been modified with subsequent evidence taken into account. Lowered by 25% to allow for inaccuracies in assessment.

12
Blood taken at 4 hours post ingestion or immediately if the patient presents after 4 hours. Blood taken prior to 4 hours is a waste of time and money!

13
Panadol Osteo…. Sustained release ◦ Use the same nomogram despite it not being validated for these preparations ◦ No evidence to suggest toxicity is different

14
Some patients take supratherapeutic doses over a number of days. ◦ Dental pain ◦ Codeine abuse ◦ Illness (these patients are often dehydrated, malnourished and higher risk. Risk Assessment Guide 10grams (child 200mg/kg) in 24 hours 6 grams (child 150mg/kg) per day for 48 days
 in 24 hours 6 grams (child 150mg/kg) per day for 48 days.")
15
You do not need to do routine paracetamol levels if a patient is cooperative and able to give a history (BestBets) However if doubt about reliability or unconscious then it is a cheap and easy test to do.
 However if doubt about reliability or unconscious then it is a cheap and easy test to do.")
16
Hepatotoxicity takes 18 – 36 hours to develop. All patients have an ALT/AST rise by 36 hours Prior to hepatotoxity most patients develop nausea, vomiting, feel unwell. But maybe asymptomatic. Liver toxicity – RUQ pain, nausea, unwell, jaundice. ALT/AST peak day 3 and LFTS are repeated in a serial fashion to map the fall. Development of liver failure depends on the amount of hepatic injury

17
Hepatitis Coagulopathy Shock Renal Failure Lactic Acidosis Hypoglycaemia Cerebral oedema - hyperammonaemia Death from multi-organ failure

18
Charcoal if present within 1 hour Only if they are conscious and compliant Remember there is an antidote

19
Thought to provide cysteine to enhance glutathione synthesis. Not contraindicated if a patient is allergic to sulphonamides/”sulfas” 10-20% may develop flushing or anaphyactoid reaction and almost all people tolerate it when it is restarted/slowed rate. All patients who receive NAC within 8 hours do well.

20
ALL PATIENTS WHO RECEIVE NAC WITHIN 8 HOURS DO WELL Regime In Australia 150 mg/kg IV infusion, over 15 to 60 minutes 50 mg/kg IV infusion, over 4 hours 100 mg/kg IV infusion, over 16 hours.

21
People over the nomogram line People who you risk assess as potential toxicity and result will take longer than 8 hours post ingestion to obtain. Patients with abnormal LFTs Supratherapeutic ingestions with high risk/abnormal LFTs – base on dose ingested

22
For how long? - If the patient receives N-Acetylcysteine within 8 hours they maybe discharged after the 20 hour infusion is complete. - Continue the infusion until paracetamol levels are undetectable if hepatic damage occurs (in consultation with clinical toxicologist)
.")
23
Na 137 K3.5 CL98 HCO3 30 Urea 2.6 Cr 46 Alb 49 AST 7234 ALT 5896 GGT 18 ALP 224 Bili 16 Paracetamol <30 BSL 6.4 Lactate 1.6 INR 1.7 Management

24
On presentation AST 7234 ALT 5896 18 hours later: AST 1642 ALT 3392 INR 1.4 26 hours later: AST 895 INR 1.3 34 hours later: AST 28 INR 1.1 Lucky!

25
Refer to liver unit ICU Liver recovery phase commences day 3 Transplant/Death

26
Patient comes in and has taken 20 tablets of olanzepine/respiridone/quetiapine/largactil What is your plan?

27
Risk Assessment Decontamination Enhance Elimination Antidotes Supportive care

28
Is the treatment you initiate to support a patients physiology.

30
Usually GCS of 8 is indication for intubation unless short acting agent involved. Prevent aspiration.

31
BP low because less awake and less endogenous catecholamines Direct pharmacological effects Dehydration Part of multiorgan failure

34
Many patients can’t urinate and its an amazing ICU physiological monitor. Will also stop patients being agitated when their bladder is full!

36
Pressure Care Blood sugar Monitoring

Similar presentations





>")


 John R. Senior, M.D. Senior Scientific Advisor Office of Drug Safety Nonprescription Drugs Advisory.>")




 to: increase polarity of the drug provide a site for phase II reactions.>")

 LIVER FUNCTION AND THE BILIARY TRACT LECTURE FIVE Dr. Essam H. Aljiffri.>")
 COX-3 in CNS PGs (brain)>")

, MCEM (London) Assistant Professor, DEM College of Medicine King Saud University Consultant Emergency Medicine.>")




