Download presentation
Presentation is loading. Please wait.

1
HISTOPATHOLOGY OF IMMUNOBULLOUS DISORDERS DR.SHUBHA

2
INTRAEPIDERMAL BULLOUS DISORDERS

3
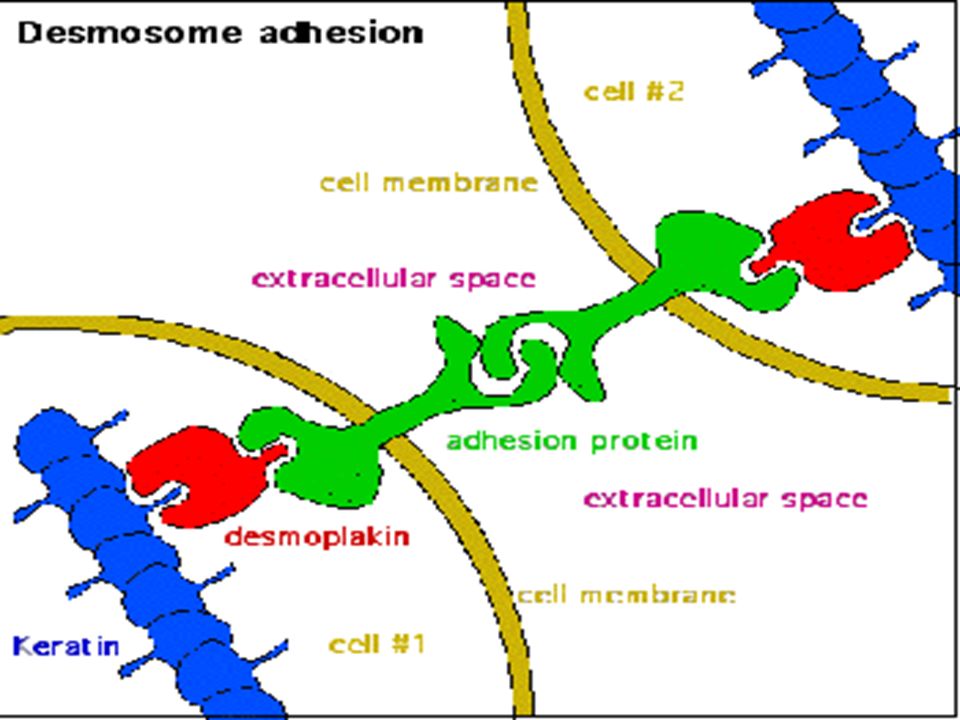
TARGET ANTIGENS Located in the desmosomes the most prominent adhesion junction in stratified squamous epithelium. Located in the desmosomes the most prominent adhesion junction in stratified squamous epithelium. Desmosome complex contains desmogleins and desmocollins as transmembrane components and desmoplakins, phakoglobins as intracellular components. Desmosome complex contains desmogleins and desmocollins as transmembrane components and desmoplakins, phakoglobins as intracellular components.

5
PEMPHIGUS VULGARIS Autoimmune disease characterised by large flaccid blisters ;primarily in older individuals. Autoimmune disease characterised by large flaccid blisters ;primarily in older individuals. Scalp, face, flexures, groin and pressure points. Scalp, face, flexures, groin and pressure points. Lesions characteristically involves the oral mucosa. Lesions characteristically involves the oral mucosa. It is important that early blisters preferably smaller ones are selected for biopsy. It is important that early blisters preferably smaller ones are selected for biopsy.

6
Greek pemphix-blister or bubble Greek pemphix-blister or bubble Disruption of intercelular cementing substance Disruption of intercelular cementing substance Most common 80% Most common 80% Fourth to sixth decade Fourth to sixth decade 50-70% mucosal lesions 50-70% mucosal lesions Bullae rupture spontaneously, no tendency to heal spontaneously Bullae rupture spontaneously, no tendency to heal spontaneously Nikolsky’s sign (Asboe-Hansen sign) Nikolsky’s sign (Asboe-Hansen sign)
 Nikolsky’s sign (Asboe-Hansen sign)")
9
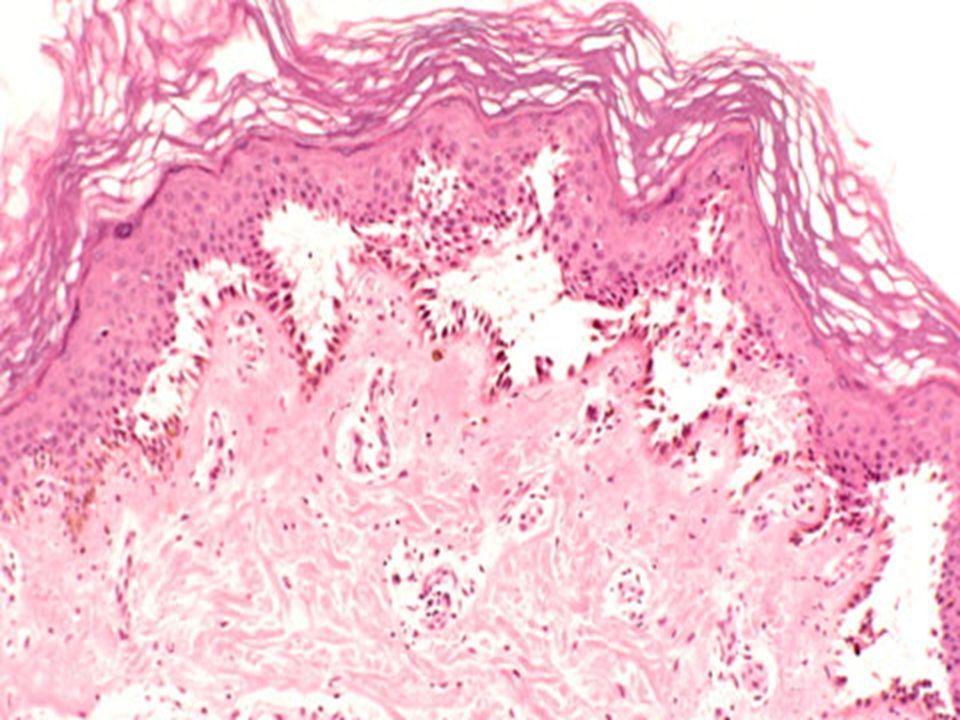
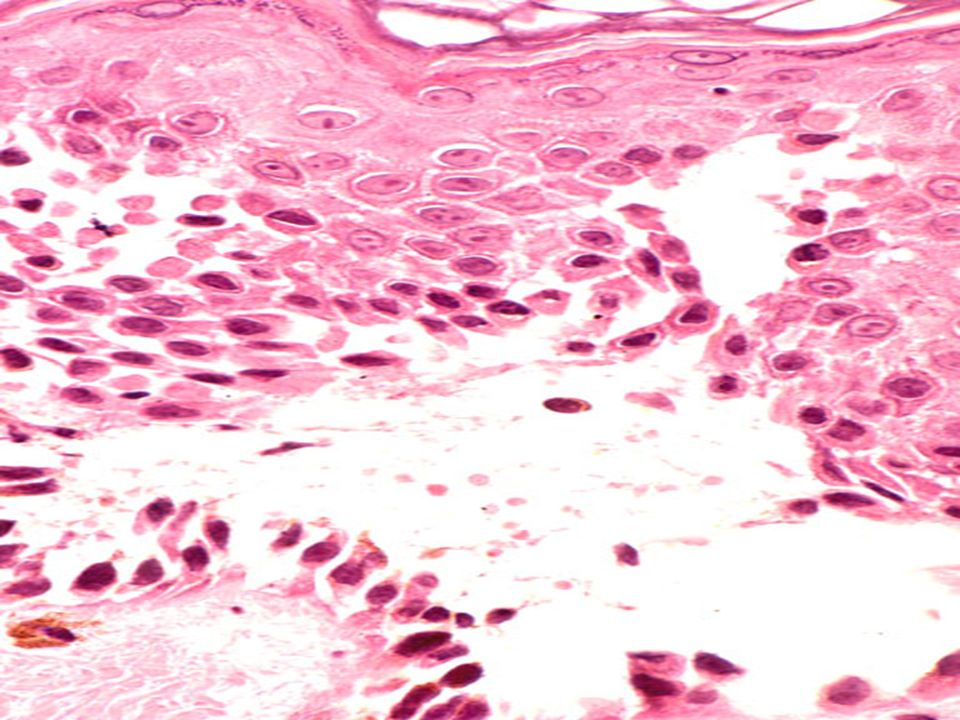
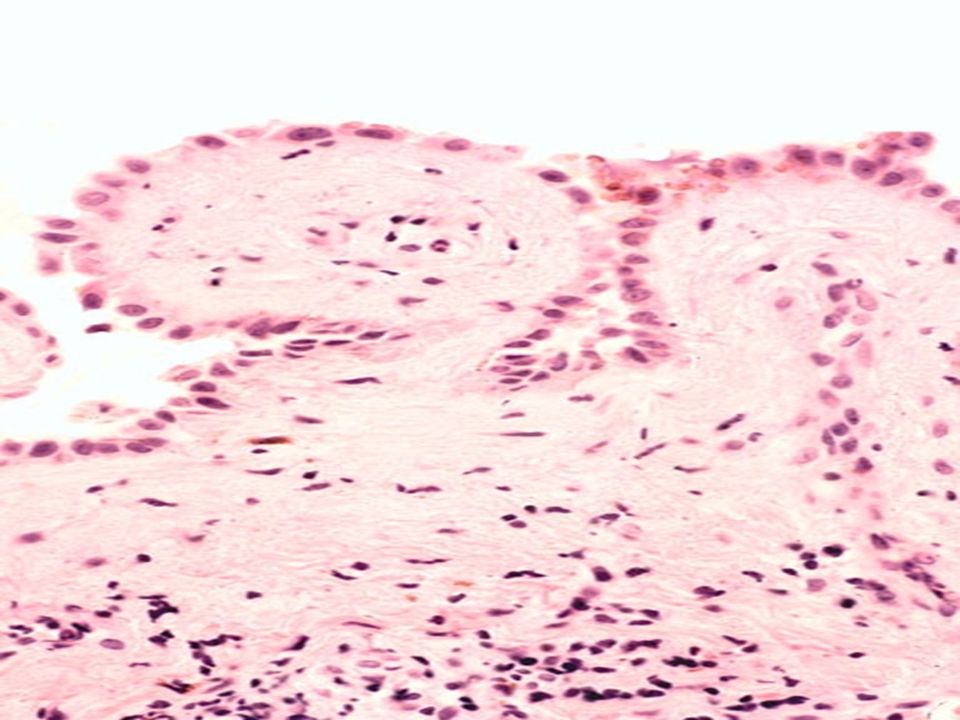
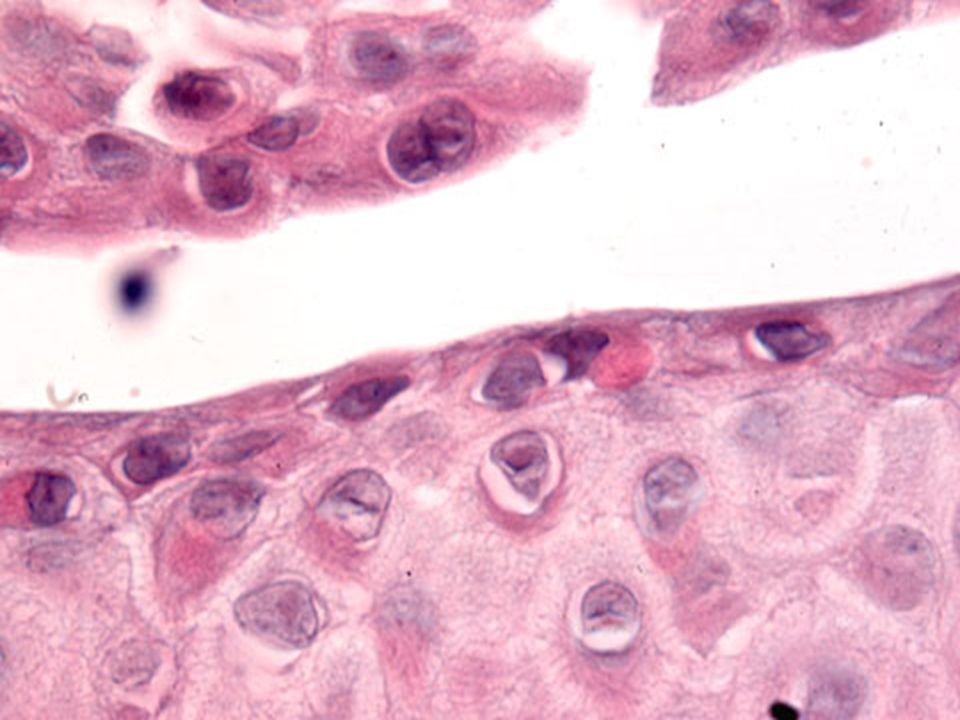
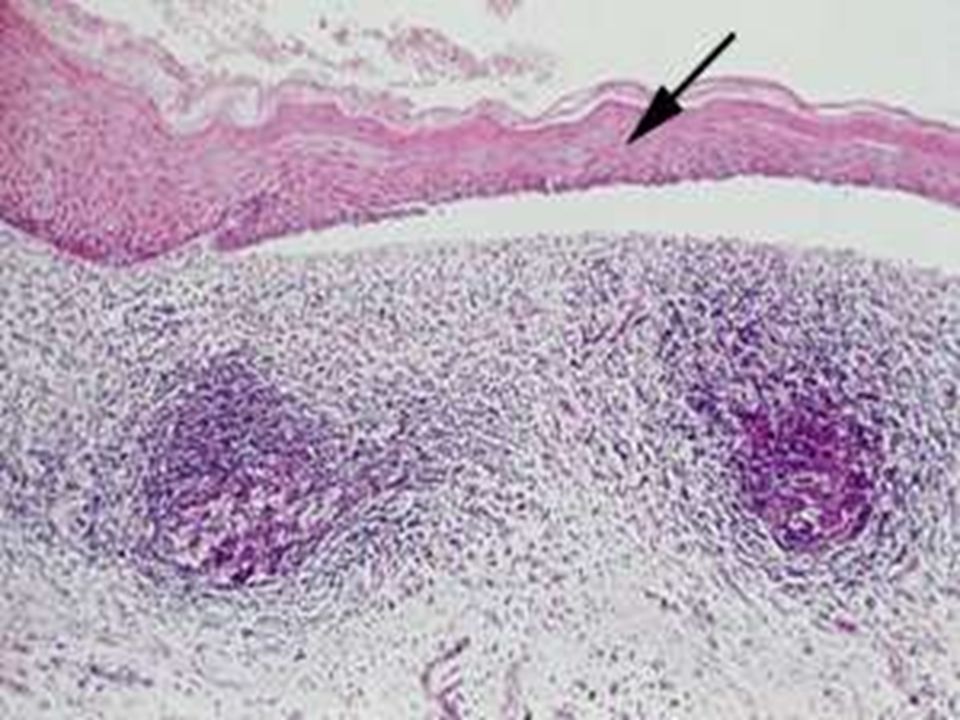
HISTOPATHOLOGY Target antigen is desmoglein 3 which is 130 kD localised in spinous layer and in mucus membrane.Early blisters; smaller in size selected. Earliest change – spongiosis in lower epidermis. Acantholysis is suprabasal,may extend into the adenexa. Basal keratinocytes though seperated from one another remain attached to the basement membrane ;”Row of tombstones appearance”.

15
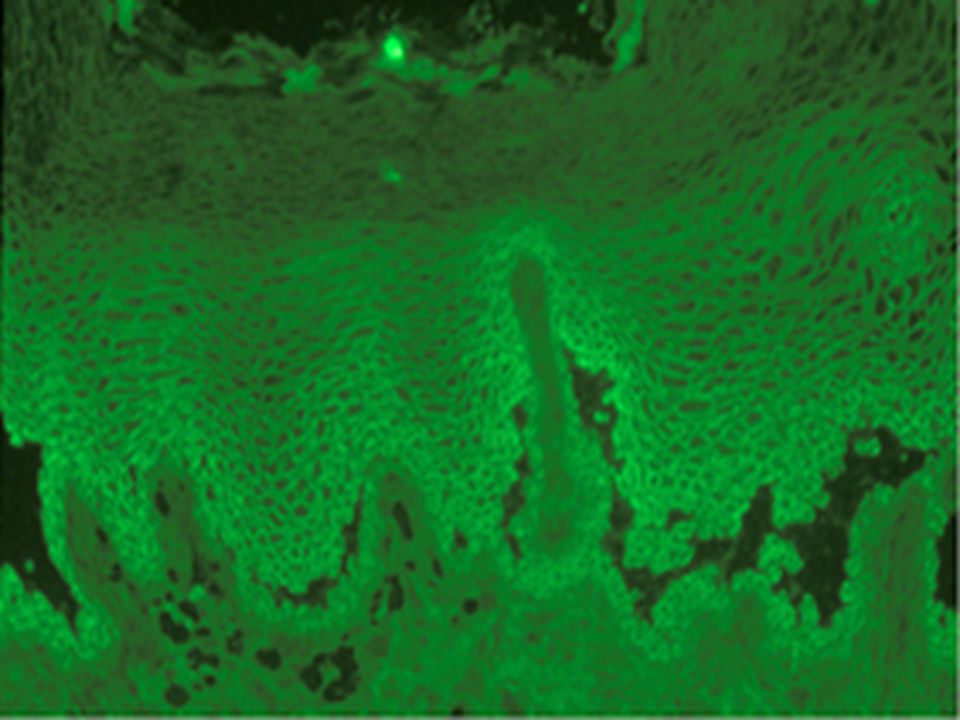
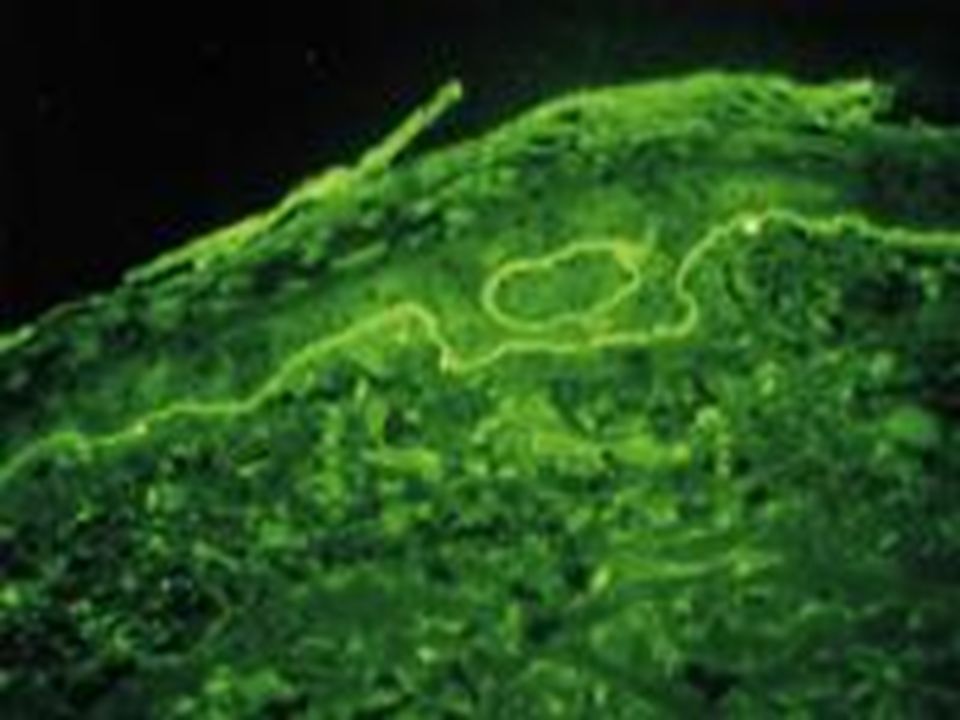
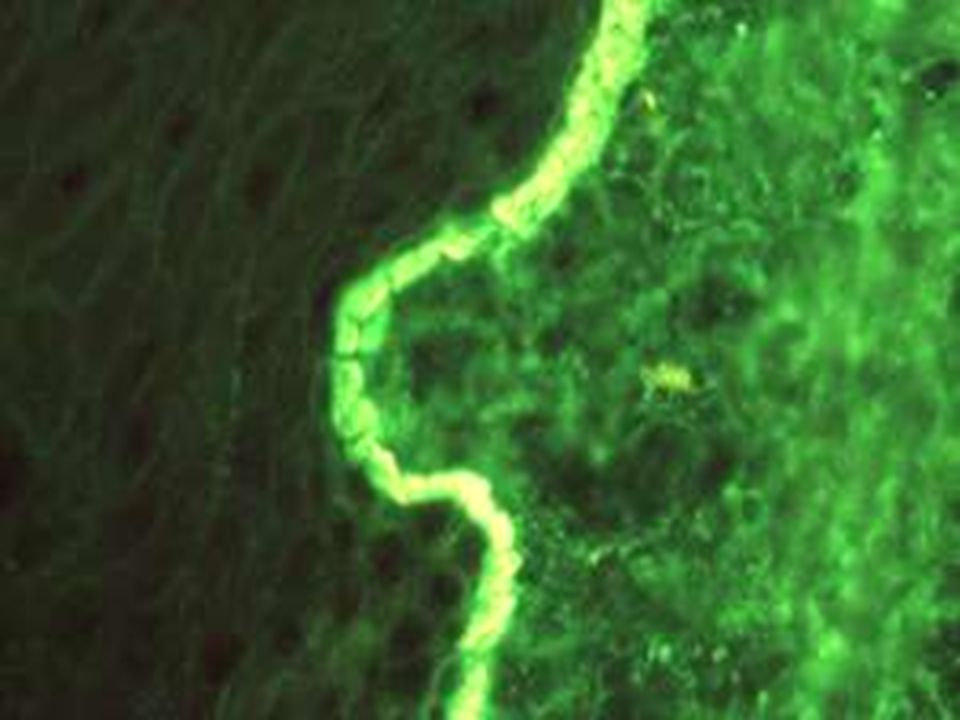
IMMUNOFLOURESCENCE DIF -Edge of the blister with intact sorrounding skin is selected; transported in michael’s medium. DIF -Edge of the blister with intact sorrounding skin is selected; transported in michael’s medium. Very sensitive and reliable test esp. in oral lesions. Very sensitive and reliable test esp. in oral lesions. Squamous intercellular or cell surface IgG deposition seen in 95 % of cases. Squamous intercellular or cell surface IgG deposition seen in 95 % of cases. IDF – IgG antibodies in 80 % of cases using monkey oesophagus as substrate. IDF – IgG antibodies in 80 % of cases using monkey oesophagus as substrate.

17
PEMPHIGUS VEGETANS Rare variant of pemphigus vulgaris. Rare variant of pemphigus vulgaris. Vegetating lesions in flexures. Vegetating lesions in flexures. Initially bullae or pustule Initially bullae or pustule Two types – Neumann and Hallopeau. Two types – Neumann and Hallopeau. Antibodies against Pemphigus vulgaris antigens – 130 KDa. Antibodies against Pemphigus vulgaris antigens – 130 KDa.

19
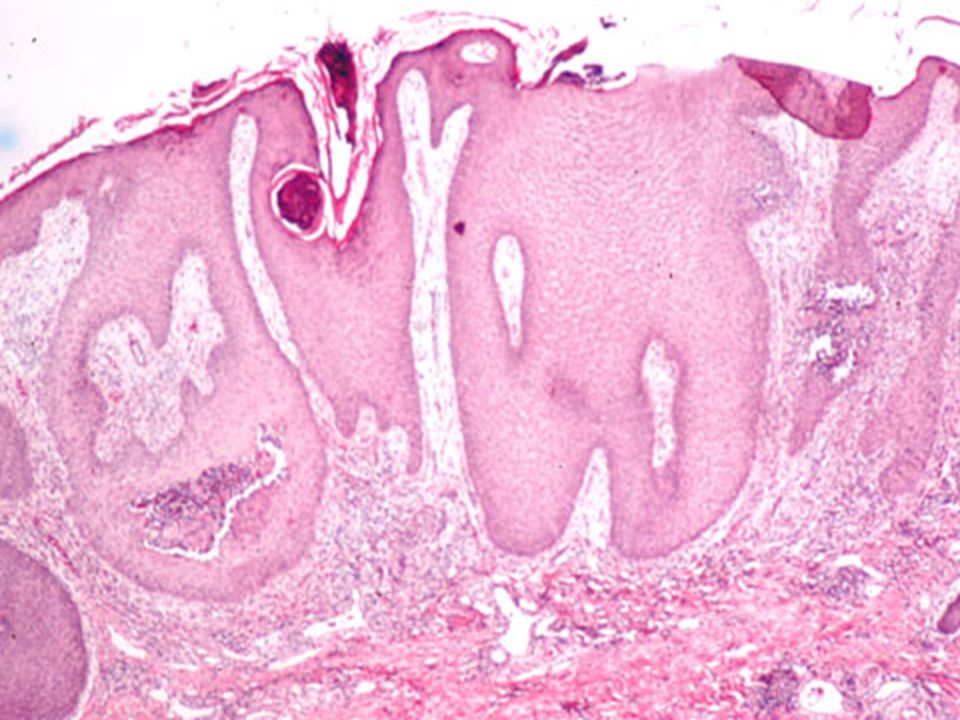
HISTOPATHOLOGY Vegetating lesions are acanthotic, hyperkeratotic and papillomatous. Vegetating lesions are acanthotic, hyperkeratotic and papillomatous. Suprabasal clefts contain acantholytic cells and eosinophils. Intraepidermal eosinophilic abscesses seen in older lesions. Suprabasal clefts contain acantholytic cells and eosinophils. Intraepidermal eosinophilic abscesses seen in older lesions. Hallopeau lesions – pustules on normal skin with acantholysis and small suprabasal clefts. Hallopeau lesions – pustules on normal skin with acantholysis and small suprabasal clefts. Dermis – heavy infiltrate of lymphocytes and eosinophils with few neutrophils. Dermis – heavy infiltrate of lymphocytes and eosinophils with few neutrophils.

21
IMMUNOFLOURESCENCE DIRECT -Intercellular deposition of IgG in all reported cases. DIRECT -Intercellular deposition of IgG in all reported cases. INDIRECT -Positive in most of the patients. INDIRECT -Positive in most of the patients. Differential diagnosis – Pyoderma vegetans ; seen in association with inflammatory bowel disease. Neutrophils are more common. Eosinophilic abscesses and acantholytic cells are rare.Mimicks pemphigus vegetans clinically and histologically. Differential diagnosis – Pyoderma vegetans ; seen in association with inflammatory bowel disease. Neutrophils are more common. Eosinophilic abscesses and acantholytic cells are rare.Mimicks pemphigus vegetans clinically and histologically.

22
PEMPHIGUS FOLIACEOUS Subcorneal blister Subcorneal blister Ig G antibodies against desmoglein 1 Ig G antibodies against desmoglein 1 Les severe, crusted moist, scaly lesions in seborrheic distribution Les severe, crusted moist, scaly lesions in seborrheic distribution Very transient Very transient Better prognosis Better prognosis

23
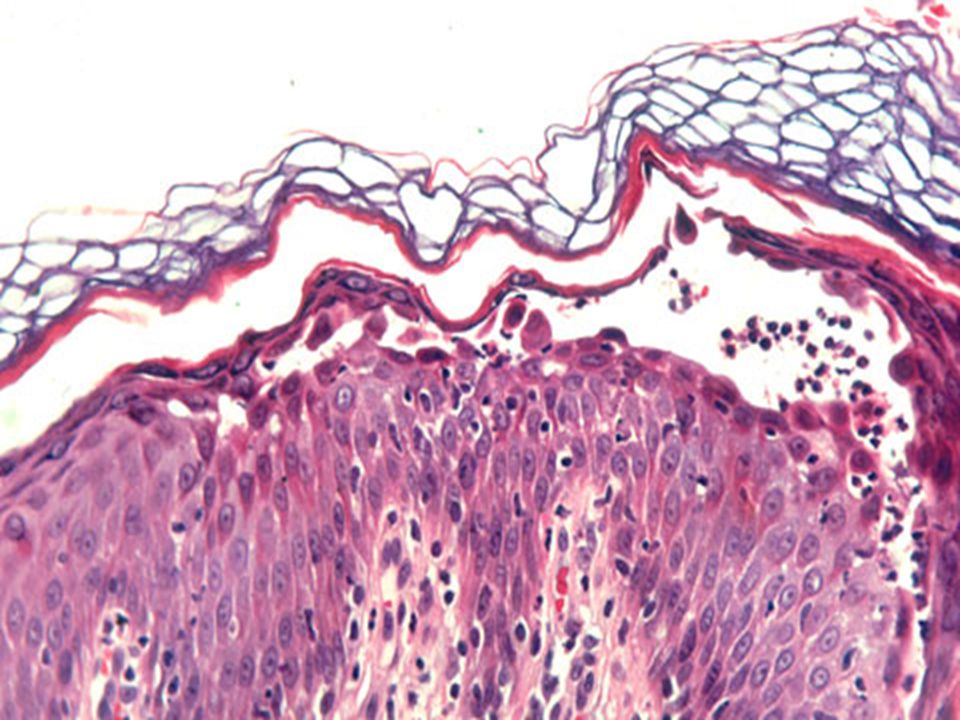
Early lesions – Vacoulation in intracellular spaces in the upper level of epidermis which coalesce to form clefts and bullae in granular layer or immediately beneath the stratum corneum. Early lesions – Vacoulation in intracellular spaces in the upper level of epidermis which coalesce to form clefts and bullae in granular layer or immediately beneath the stratum corneum. Bullae contain fibrin, acantholytic cells and neutrophils. Bullae contain fibrin, acantholytic cells and neutrophils. Dyskeratotic cells in granular layer important. Dyskeratotic cells in granular layer important. Dermis shows mixed infiltrate of eosinophils and neutrophils. Dermis shows mixed infiltrate of eosinophils and neutrophils.

28
IMMUNOFLOURESCENCE DIRECT - Intercellular IgG and C3 deposition throughout the epidermis or restricted to upper part of epidermis. DIRECT - Intercellular IgG and C3 deposition throughout the epidermis or restricted to upper part of epidermis. INDIRECT– Positive in 85 % of sera. INDIRECT– Positive in 85 % of sera. Pemphigus foliaceous antibody DESMOGLEIN 1 is expressed more in the upper layers of epidermis. Pemphigus foliaceous antibody DESMOGLEIN 1 is expressed more in the upper layers of epidermis. Staphylococcal scalded skin syndrome Staphylococcal scalded skin syndrome

29
DIFFERENTIAL DIAGNOSIS Marked dyskeratosis distinguishes pemphigus foliaceous from p.vulgaris.ultrastructurally, there is early loss of intercellular cement substance in lower half of epidermis, perinuclear homogenisation of tonofilaments in mid epidermis. Marked dyskeratosis distinguishes pemphigus foliaceous from p.vulgaris.ultrastructurally, there is early loss of intercellular cement substance in lower half of epidermis, perinuclear homogenisation of tonofilaments in mid epidermis. Impetigo Impetigo Subcorneal pustular dermatosis Subcorneal pustular dermatosis SSSS. SSSS.

30
PEMPHIGUS ERYTHEMATOSUS Senear Usher syndrome Senear Usher syndrome Variant of pemphigus foliaceous. Variant of pemphigus foliaceous. Clinically resembles lupus erythematosus ; erythematous plaques and patches in butterfly distribution. Clinically resembles lupus erythematosus ; erythematous plaques and patches in butterfly distribution. HPE – Light microscpic changes similar to P. foliaceous. Rarely interface dermatitis in older lesions. HPE – Light microscpic changes similar to P. foliaceous. Rarely interface dermatitis in older lesions. Direct immunoflourescence – squamous intercellular deposition of IgG, granular IgG and IgM at dermoepidermal junction.ANA positive in 30 – 80 % of cases. Direct immunoflourescence – squamous intercellular deposition of IgG, granular IgG and IgM at dermoepidermal junction.ANA positive in 30 – 80 % of cases.

31
IgA pemphigus Pruritic pustular eruption in middle aged and elderly characterised by intercellular IgA deposition and intraepidermal neutrophils. Pruritic pustular eruption in middle aged and elderly characterised by intercellular IgA deposition and intraepidermal neutrophils. Two types –1. Subcorneal pustular dermatosis type – subcorneal vesicles and pustules with minimal acantholysis.2. intraepidermal neutrophilic dermatosis Two types –1. Subcorneal pustular dermatosis type – subcorneal vesicles and pustules with minimal acantholysis.2. intraepidermal neutrophilic dermatosis Antibodies against Desmocollin -1 in SCPD type and Desmoglein 2 in latter type. Antibodies against Desmocollin -1 in SCPD type and Desmoglein 2 in latter type.

33
PARANEOPLASTIC PEMPHIGUS Most common neoplasm – Nonhodgkins lymphoma, CLL, castlemans tumour,thymomas and sarcomas. Most common neoplasm – Nonhodgkins lymphoma, CLL, castlemans tumour,thymomas and sarcomas. Histological pitcure depends on various clinical presentations – unique combination of erythema multiforme like, lichen planus like, pemphigus vulgaris like and pemphigoid like features. Histological pitcure depends on various clinical presentations – unique combination of erythema multiforme like, lichen planus like, pemphigus vulgaris like and pemphigoid like features.

35
HISTOPATHOLOGY Suprabasal acantholysis. Suprabasal acantholysis. Basal apoptosis Basal apoptosis Interface dermatitis (erythema multiforme like ) Interface dermatitis (erythema multiforme like ) With or without lichenoid inflammation. With or without lichenoid inflammation. desmoplakin desmoplakin
 Interface dermatitis (erythema multiforme like ) With or without lichenoid inflammation. With or without lichenoid inflammation. desmoplakin desmoplakin.")
36
IMMUNOFLOURESCENCE DIRECT – Squamous intercellular deposition of IgG in perilesional skin ; At dermoepidermal junction linear deposition of C3 and IgG seen. DIRECT – Squamous intercellular deposition of IgG in perilesional skin ; At dermoepidermal junction linear deposition of C3 and IgG seen. IgG antibodies directed against desmoplakins, envoplakins and desmogleins. IgG antibodies directed against desmoplakins, envoplakins and desmogleins.

37
Endemic P.Foliaceous Endemic P.Foliaceous Bite of black fly Bite of black fly Drug Penicillamine,captopril, penicillin,rifampicin Penicillamine,captopril, penicillin,rifampicin Neonatal pemphigus Transplacental transfer, resolves in 2 weeks Transplacental transfer, resolves in 2 weeks

38
Treatment Treatment Systemic steroids Systemic steroids DCP DCP Dapsone Dapsone Methotrexate Methotrexate Azathioprine Azathioprine Ciclosporine Ciclosporine plasmapheresis plasmapheresis

39
SUBEPIDERMAL BLISTERING DISORDERS BULLOUS PEMPHIGOID – BULLOUS PEMPHIGOID – Elderly Preceded by pruritis by 2-3 weeks Tense bullae on flexures Face and scalp relatively spared Heals spontaneously with PIH Nikolsky negative Mucosa rare

40
Underlying malignancy-gastric carcinoma Underlying malignancy-gastric carcinoma DM, RA, psoriasis DM, RA, psoriasis Better prognosis than pemphigus Better prognosis than pemphigus Topical and systemic steroids Topical and systemic steroids

41
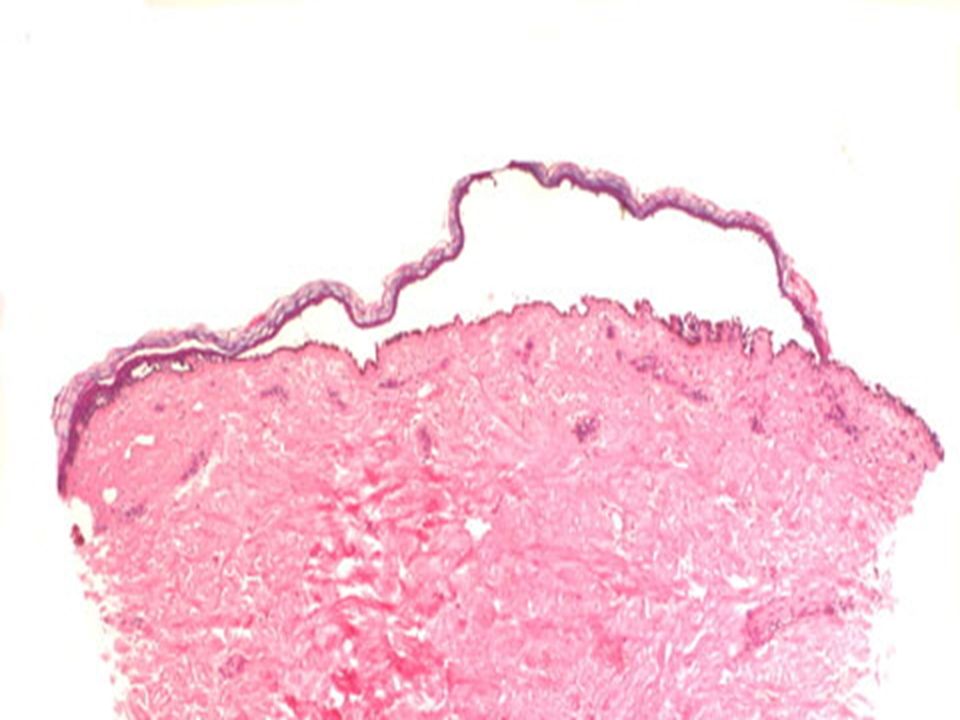
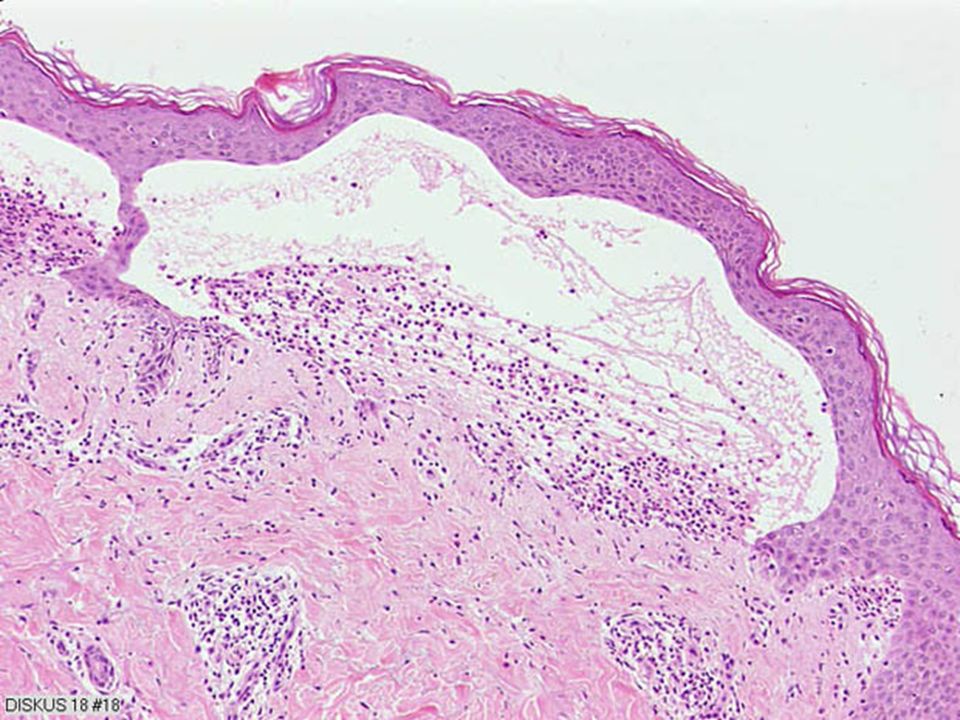
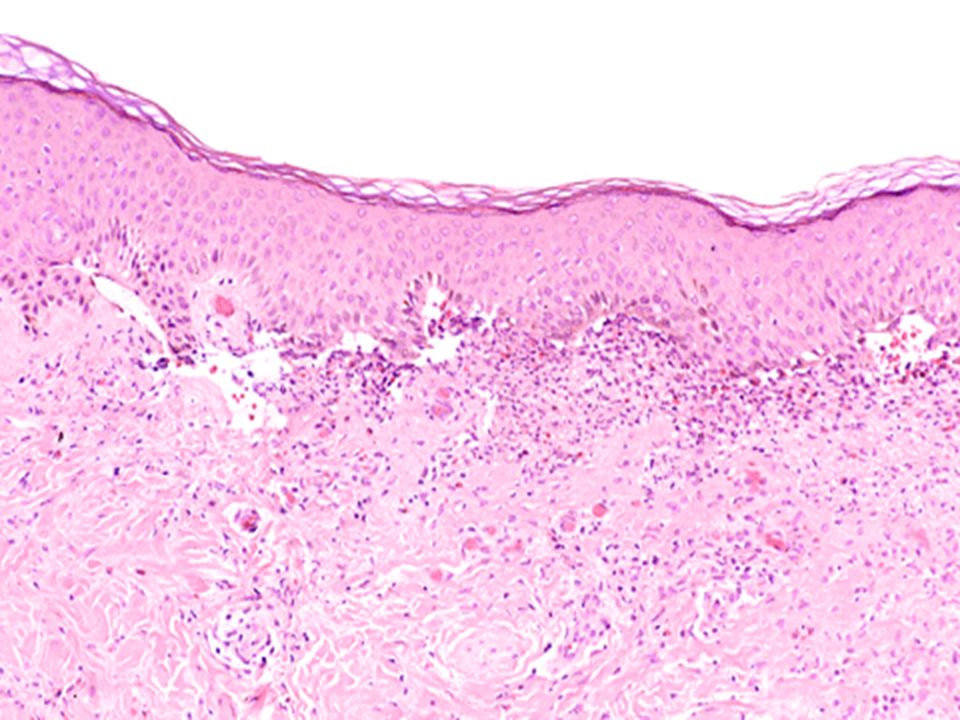
Antibodies react with two antigens ; 230 – kD(BPAg1), 180kD (BPAg2). Antibodies react with two antigens ; 230 – kD(BPAg1), 180kD (BPAg2). Blister is subepidermal with intact and often viable epidermis forming the roof. Blister is subepidermal with intact and often viable epidermis forming the roof. Early lesions show papillary edema with cell rich or cell poor perivascular lymphocytes and eosinophilic infiltrate. Eosinophilic spongiosis or microabscesses may be seen. Early lesions show papillary edema with cell rich or cell poor perivascular lymphocytes and eosinophilic infiltrate. Eosinophilic spongiosis or microabscesses may be seen. Blister lumen contains inflammatory cells. Blister lumen contains inflammatory cells.
, 180kD (BPAg2). Blister is subepidermal with intact and often viable epidermis forming the roof. Blister is subepidermal with intact and often viable epidermis forming the roof. Early lesions show papillary edema with cell rich or cell poor perivascular lymphocytes and eosinophilic infiltrate. Eosinophilic spongiosis or microabscesses may be seen. Early lesions show papillary edema with cell rich or cell poor perivascular lymphocytes and eosinophilic infiltrate. Eosinophilic spongiosis or microabscesses may be seen. Blister lumen contains inflammatory cells. Blister lumen contains inflammatory cells..")
46
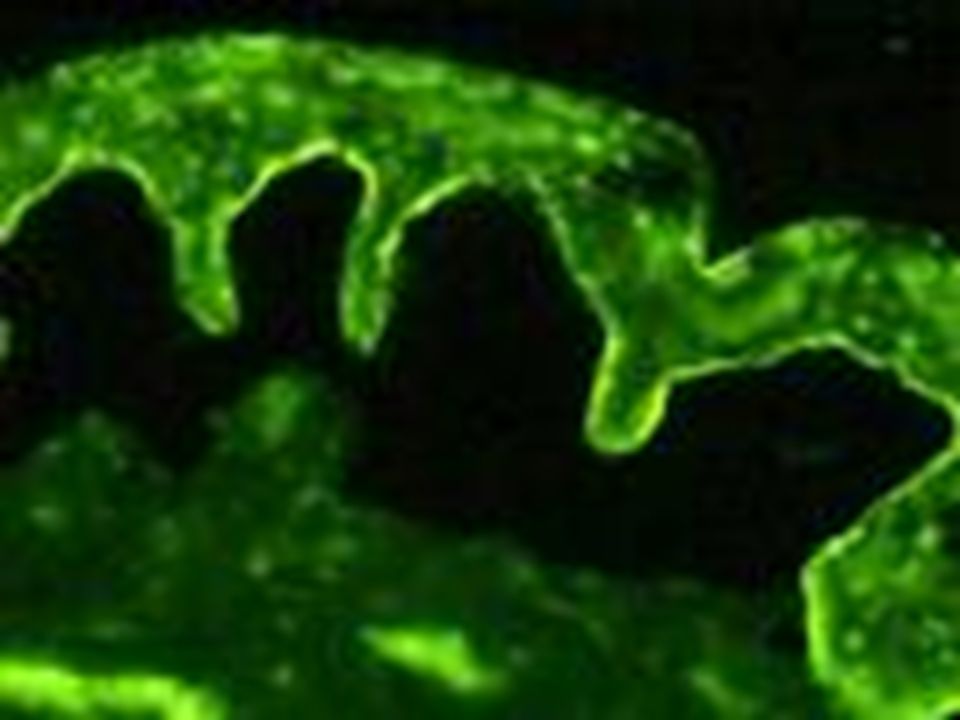
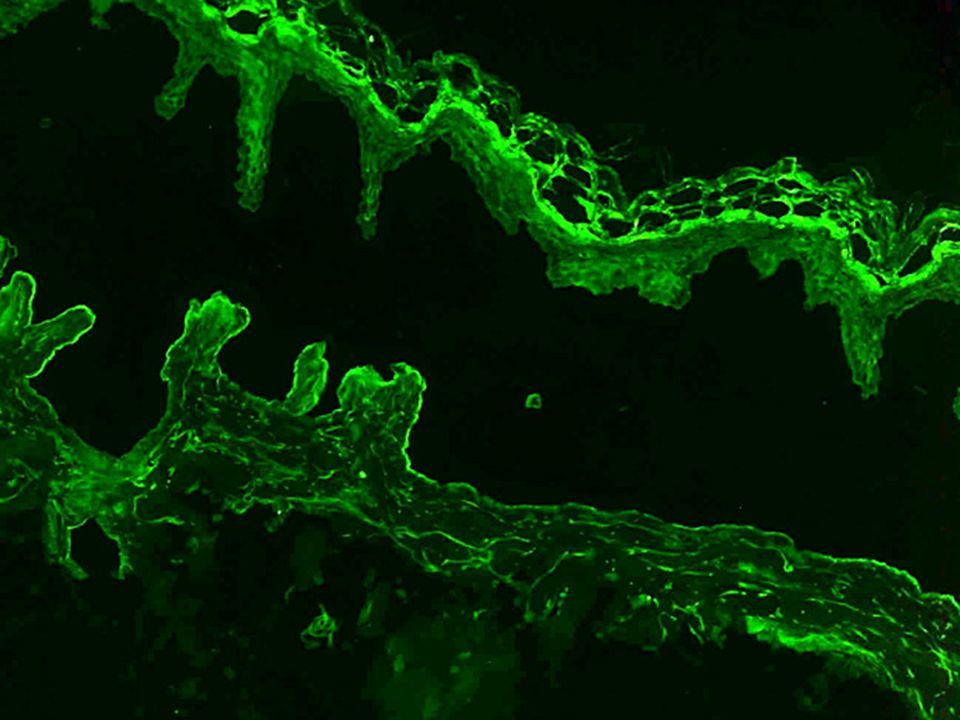
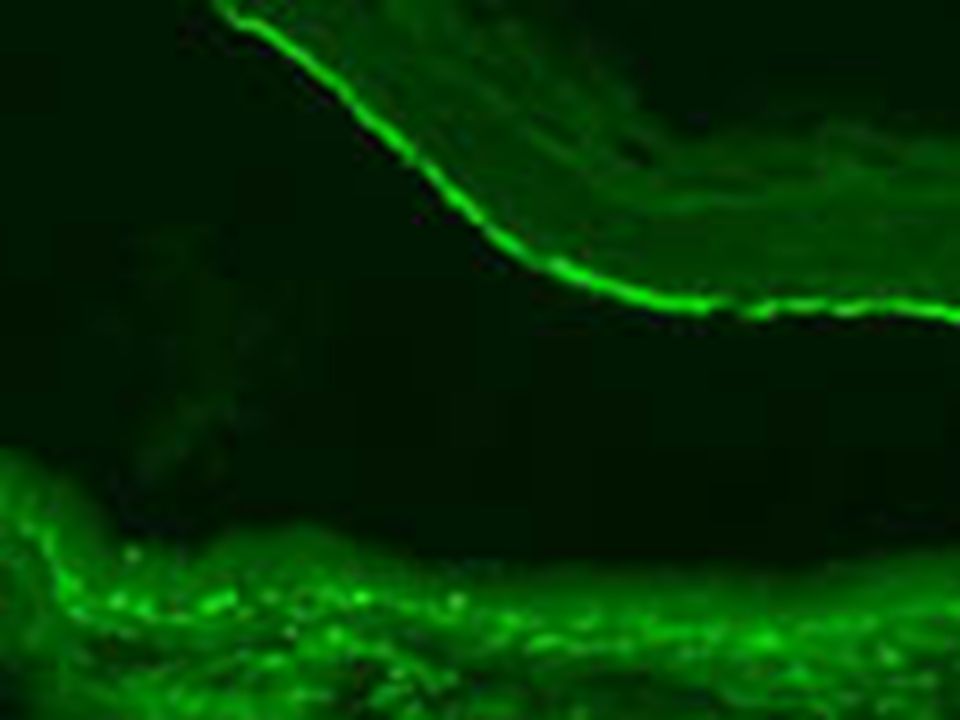
IMMUNOFLOURESCENCE Direct -Linear C3 deposition at dermo – epidermal junction in 100 % of cases and IgG in 65 – 95 %.IgG is located within lamina lucida and specifically bound to hemidesmosomes. Salt split technique – IgG at roof or floor of artificially induced blister. Indirect – circulating IgG antibodies to basement membrane zone in 70 – 80 %.

50
MUCUS MEMBRANE PEMPHIGOID Subepidermal blister that may extend down the adenexa. Subepidermal blister that may extend down the adenexa. Neutrophils, lymphocytes and histiocytes predominate in the infiltrate with less eosinophils. Neutrophils, lymphocytes and histiocytes predominate in the infiltrate with less eosinophils. Late lesions –Lamellar fibrosis is the hallmark. Late lesions –Lamellar fibrosis is the hallmark. Mucosal lesions show cell rich lichenoid infiltrate. Mucosal lesions show cell rich lichenoid infiltrate.

53
HERPES GESTATIONALIS non viral auto immune 21-28 weeks of pregnancy, 1 st post natal Severe pruritis with urticaria, wheals Peri umbilical, lower abdomen, thigh Rarely mucosa Recurs with OCP, pregnancies, premenstrually

54
Early urticated lesions show marked edema of papillary dermis with foci of eosinophilic spongiosis. Blister is subepidermal with split at lamina lucida. DIF – linear deposition of C3 and IgG at basement membrane zone. Split skin – binding at epidermal side of the blister.

55
EPIDERMOLYSIS BULLOSA AQUISITA Acquired autoimmune Trauma induced sub epidermal blistering Mucosal lesions

56
Two forms – 1. Bullous pemphigoid like eruption ; heavy inflammatory infiltrate mainly neutrophils and lymphocytes., heals with scarring, mechanobullous type, dystrophic nails 2.classical form with sparse infiltrate. DIF – Linear C3 deposition at basement membrane ;IgG in some cases. Salt split – Abs bind to lamina densa (type V11 collagen) and hence seen at floor of blister.
 and hence seen at floor of blister..")
59
BULLOUS SLE Three histological patterns – 1.striking basal cell vacuolization with subepidermal blister formation. 2.vasulitis with subepidermal blister formation. 3. dermatitis herpetiformis like lesion. Three histological patterns – 1.striking basal cell vacuolization with subepidermal blister formation. 2.vasulitis with subepidermal blister formation. 3. dermatitis herpetiformis like lesion. Neutrophils prominent in blister cavity and superficial dermis. Neutrophils prominent in blister cavity and superficial dermis. DIF – IgG and C3 at basement membrane zone (linear or granular band like ). DIF – IgG and C3 at basement membrane zone (linear or granular band like ). Salt split – localization at floor. Salt split – localization at floor.
. DIF – IgG and C3 at basement membrane zone (linear or granular band like ). Salt split – localization at floor. Salt split – localization at floor..")
60
Treatment Treatment Steroids Steroids Dapsone Dapsone Immunosuppresive therapy Immunosuppresive therapy

63
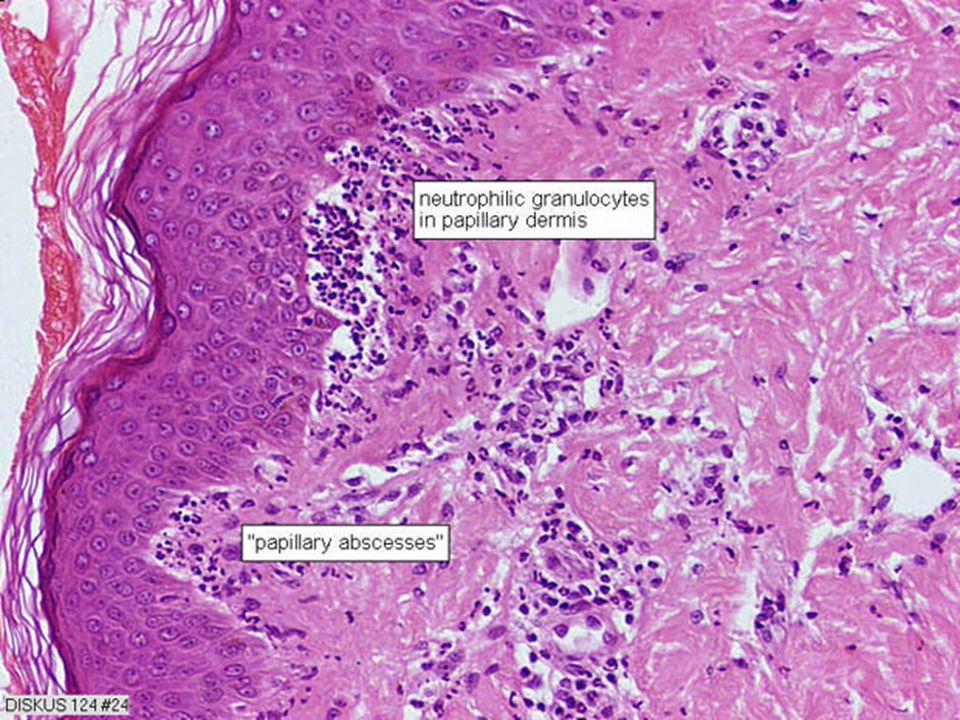
DERMATITIS HERPETIFORMIS Prutitic, chronic, recurrent, papulovesicular lesions extensors, buttocks, shoulders Prutitic, chronic, recurrent, papulovesicular lesions extensors, buttocks, shoulders Gluten sensitivity Gluten sensitivity HLA-B8 HLA-B8 20-55 years 20-55 years MC males MC males Oral lesions Oral lesions Provocation of lesions with iodides Provocation of lesions with iodides

64
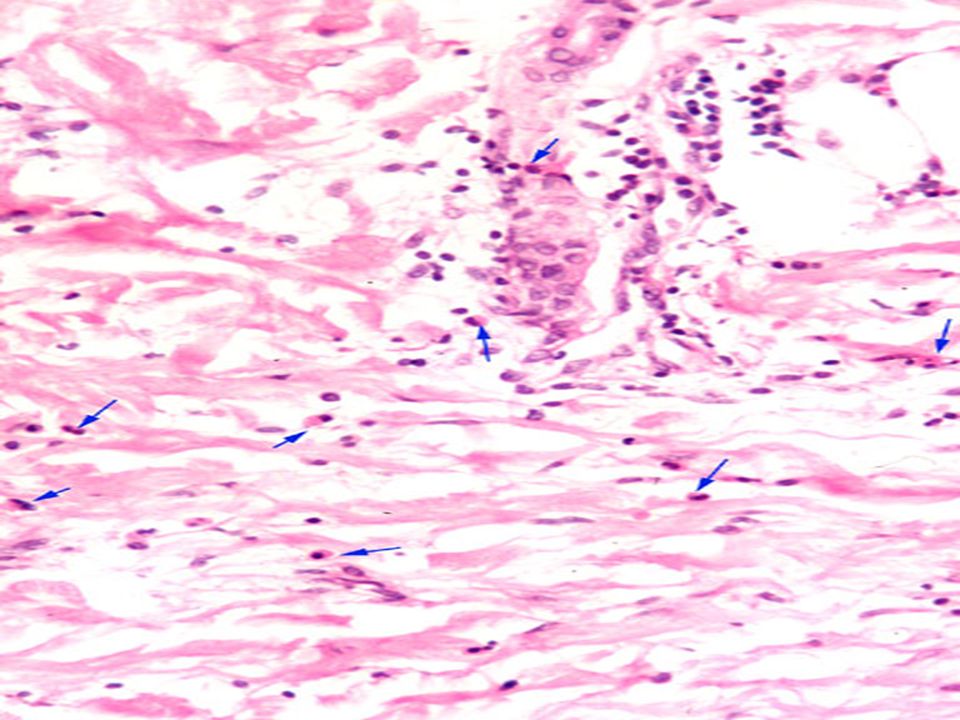
Typically seen in erythematous skin adjacent to the early blisters. Typically seen in erythematous skin adjacent to the early blisters. Characteristic dermal papillary neutrophilic microabscesses which separate the tips of papillae from epidermis to form multilocular blisters. Characteristic dermal papillary neutrophilic microabscesses which separate the tips of papillae from epidermis to form multilocular blisters. Papillary dermis beneath – intense infiltrate of neutrophils and some eosinophils Papillary dermis beneath – intense infiltrate of neutrophils and some eosinophils

69
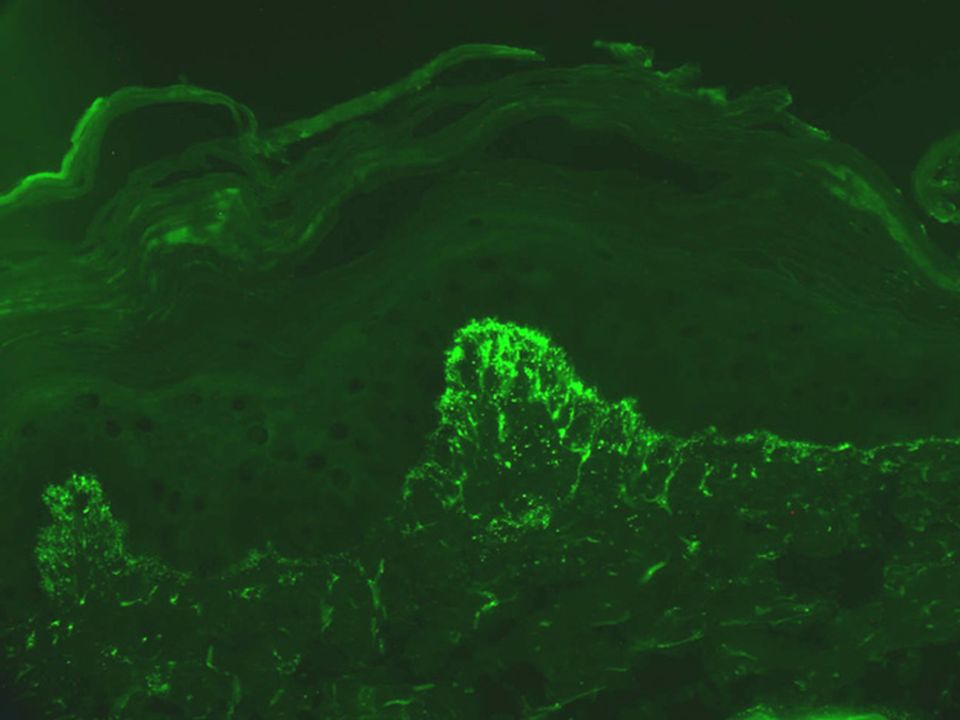
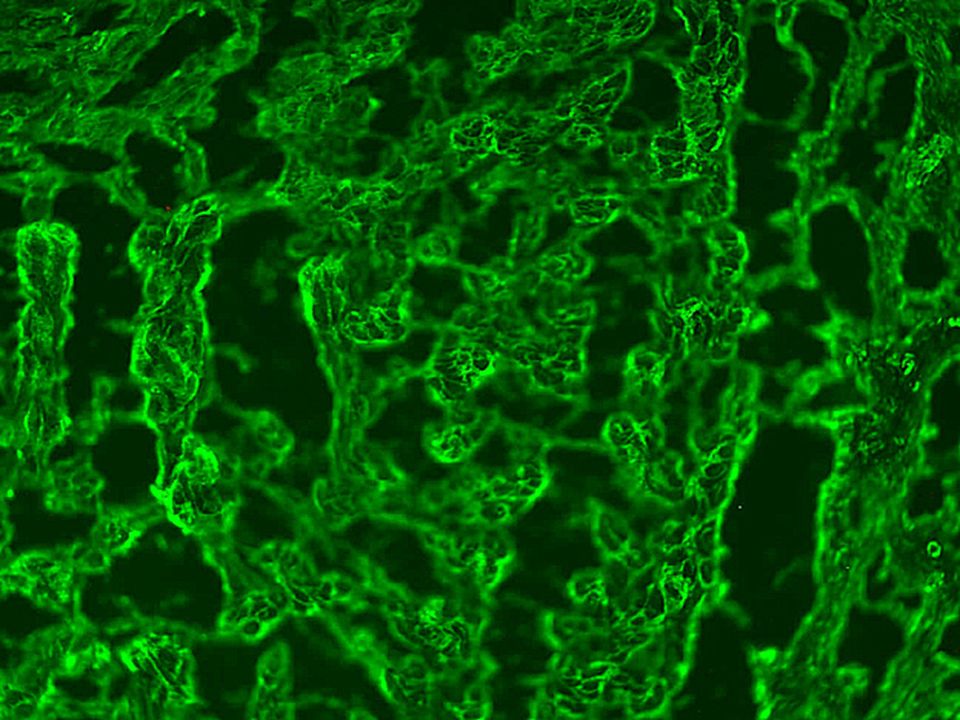
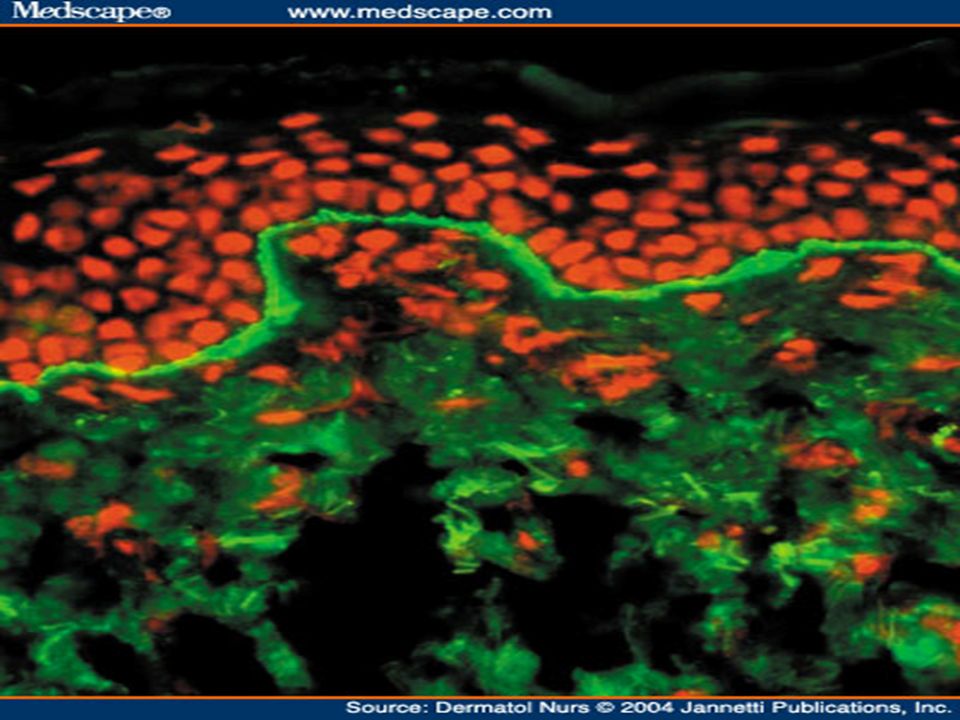
IMMUNOFLOURESCENCE DIF – Granular IgA deposition in papillary dermis in both lesional and perilesional skin. DIF – Granular IgA deposition in papillary dermis in both lesional and perilesional skin. IgA is exclusively IgA1, both monomeric and polymeric with J chain and secretory components, associated with microfibrils. IgA is exclusively IgA1, both monomeric and polymeric with J chain and secretory components, associated with microfibrils. IIF – Antiendomysial antibodies (smooth muscle ), antireticulin, antigliadin antibodies. IIF – Antiendomysial antibodies (smooth muscle ), antireticulin, antigliadin antibodies. Antibodies against Trans-glutaminase II. Antibodies against Trans-glutaminase II.
, antireticulin, antigliadin antibodies. IIF – Antiendomysial antibodies (smooth muscle ), antireticulin, antigliadin antibodies. Antibodies against Trans-glutaminase II. Antibodies against Trans-glutaminase II..")
71
Treatment Treatment Dapsone 100-200 mg/day Dapsone 100-200 mg/day Gluten free diet Gluten free diet

72
LINEAR IgA DERMATOSES Two types 1.adult linear IgA dermatoses. 2.chronic benign bullous dermatoses of childhood. Two types 1.adult linear IgA dermatoses. 2.chronic benign bullous dermatoses of childhood. Adult – similar to dermatitis herpetiformis i.e.papillary neutrophilic abscesses or neutrophils along dermoepidermal junction. Adult – similar to dermatitis herpetiformis i.e.papillary neutrophilic abscesses or neutrophils along dermoepidermal junction. Children – string of pearl appearance.- urticarial plaques blistering at edge Children – string of pearl appearance.- urticarial plaques blistering at edge

74
IMMUNOFLOURESCENCE DIF – linear deposition of IgA along basement membrane zone. DIF – linear deposition of IgA along basement membrane zone. Salt split at lamina lucida – majority bind to upper part of blister, few combined and few to lower. Salt split at lamina lucida – majority bind to upper part of blister, few combined and few to lower. IIF – more positivity in children. IIF – more positivity in children. Drug induced – most common to vancomycin, diclofenac, lithium and captopril. Drug induced – most common to vancomycin, diclofenac, lithium and captopril.

77
Disease Direct IMF Isoty pe Target antige ns Antig ens Location Pemphigus vulgaris Intercell- ular IgG,IgM Desmo glein3 130Desmosomes Vegetans Intercell- ular IgG Desmo glein1 160Desmosomes Foliaceus Intercell- ular IgG Desmo glein1 160Desmosomes Paraneoplast ic pemphigus Intercell- ular and subepide rmal IgGplakins 230,2 50 Desmosomes, BMZ

78
Disease Direct IMF Isotype Bindin g to split skin Target Antige ns Locatio n Structu re Bullous Pemphi goid Linear BMZ IgG Epider mal BP230 BP180 Hemid esmoso me Dense plaque Mucou s membr ane pemphi goid Linear BMZ IgG Epider mal BP180, BP230 Lamina lucida Anchor ing Filame nt Pemphi goid gestatio nis Linear BMZ IgG Epider mal BP180, BP230 Hemid esmoso me Dense plaque Linear IgA disease Linear BMZ IgA Epider mal DermalBP180 Collage n VII Hemid esmoso me Epider molysis bullosa acquisti a Linear BMZ IgGDermal Collage n VII Lamina Densa Anchor ing Fibril Bullous SLE Linear BMZ IgG,Ig A Dermal Collage n VII Lamina Densa Anchor ing Fibril

79
Linear IgA disease Linear BMZ IgA Epider mal Derma l BP180 Collag en VII Hemid esmos ome Epidermolys is bullosa acquistia Linear BMZ IgG Derma l Collag en VII Lamin a Densa Ancho ring Fibril Bullous SLE Linear BMZ IgG,Ig A Derma l Collag en VII Lamin a Densa Ancho ring Fibril

80
THANK YOU

Similar presentations




















>")














