Download presentation
Presentation is loading. Please wait.

1
London Workshop on Public Health Information and Intelligence 26 July 2012 Public Health Informatics, the DH perspective Jürgen Schmidt Public Health England (jurgen.schmidt@dh.gsi.gov.uk)

2
Context for local public health intelligence work What are the relevant changes? –Physical move and changed functions of DPHs and their teams –Local Authority’s public health responsibilities –PHE support Emerging commissioning landscape –Functions and data flows, including data sharing and the integration of health and social care data –Changes to the IT environment, including the NHSCB DMICs –Changes to the information governance environment Formal requirements: –NHS planning guidance for 2012/13: To agree arrangements on public health information requirements and information governance by September 2012 –PHE transition guidance checklist item: Are plans in place to ensure access to IT systems, sharing of data and access to health intelligence in line with information governance and business requirements during transition and beyond?

3
Legal requirements (Act 2012) “Obtaining advice from individuals who taken together have a wide range of professional expertise in the prevention, diagnosis or treatment of illness, and the protection or improvement of public health” Authorisation Criteria “1.3 Widespread involvement of other clinical colleagues providing health services locally [identified by..] Arrangements in place between LA and CCG specifying how public health advice to CCGs will be delivered.” Clinical Commissioning Groups
![Legal requirements (Act 2012) Obtaining advice from individuals who taken together have a wide range of professional expertise in the prevention, diagnosis or treatment of illness, and the protection or improvement of public health Authorisation Criteria 1.3 Widespread involvement of other clinical colleagues providing health services locally [identified by..] Arrangements in place between LA and CCG specifying how public health advice to CCGs will be delivered. Clinical Commissioning Groups](http://images.slideplayer.com/42/11523570/slides/slide_3.jpg "Legal requirements (Act 2012) Obtaining advice from individuals who taken together have a wide range of professional expertise in the prevention, diagnosis or treatment of illness, and the protection or improvement of public health Authorisation Criteria 1.3 Widespread involvement of other clinical colleagues providing health services locally [identified by..] Arrangements in place between LA and CCG specifying how public health advice to CCGs will be delivered. Clinical Commissioning Groups")
4
Commissioning Support Services Potential NHS commissioning support suppliers should: “Develop an understanding of how their offer will relate to other parts of the commissioning support supply chain and the delivery impact of this (for example by engaging with local authorities and the public health team to establish what they are providing)” “Work is on-going to establish which elements of Health Needs Assessment and Business Intelligence for NHS commissioners might be secured as part of a ‘core offer’ from Public Health England (PHE) and which components might be provided by NHS commissioning support functions”
 Work is on-going to establish which elements of Health Needs Assessment and Business Intelligence for NHS commissioners might be secured as part of a ‘core offer’ from Public Health England (PHE) and which components might be provided by NHS commissioning support functions")
5
Local authority public health intelligence

6
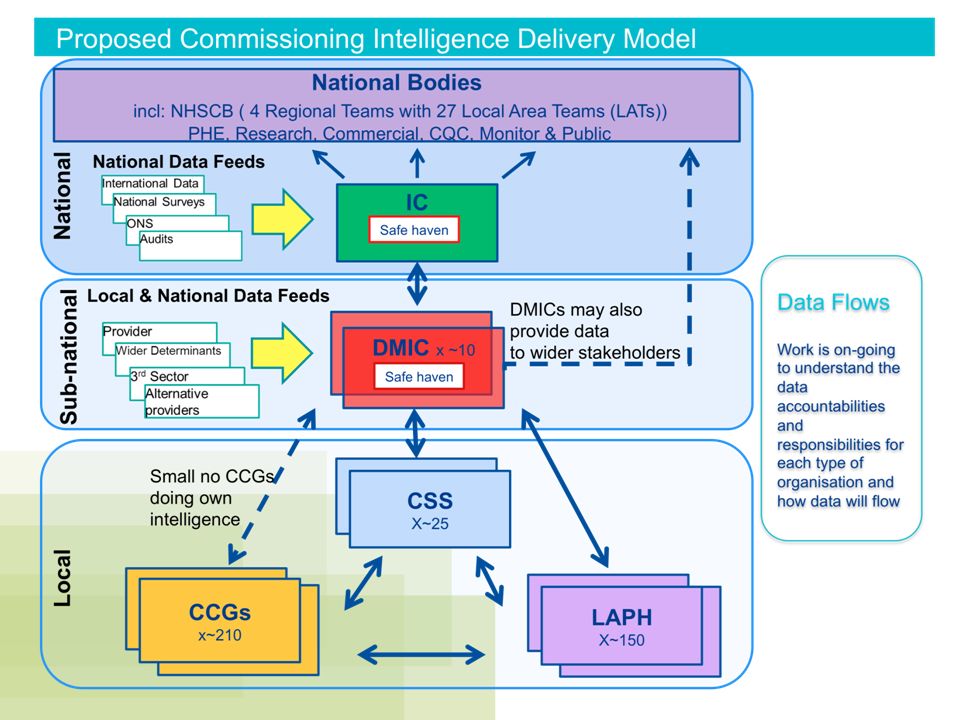
NHSCB Commissioning Intelligence Model The CIM Model is a consolidated view of the different types of commissioning intelligence requirements needed to support evidence based commissioning decisions

7
Business model Data management capabilities could be provided by specialist integration centres supporting CSSs and CCGs using an integrated commissioning data model

8
Health Intelligence Value Chain Historic Public health intelligence roles Data Formulate Query Source data Download data Process & validate data Link data Analyse & interpret data Insight Proposed future Public Health Intelligence roles Proposed future DMIC roles

10
Access to NHS data for public health teams in Local Authorities Technical barriers –Connectivity, N3 access Information Governance –Role-based access (function of public health staff in LAs will be different from the role in PCTs) –IG system is itself undergoing transition (NIGB, Caldicott 2) –LAs compliance with NHS IG toolkit Business model barriers Management of record level NHS data with CSSs who will most likely also analyse the data on behalf of CCGs –CSSs may consider LAs additional customers –CSSs may charge for analytical services that may not be available within the LA public health function, or charge for access to certain local data sets not available from national sources –The CSSs may rely on a small number of Data Management and Integration Centres to provide data services and these may not be ready by April 2013.
 –IG system is itself undergoing transition (NIGB, Caldicott 2) –LAs compliance with NHS IG toolkit Business model barriers Management of record level NHS data with CSSs who will most likely also analyse the data on behalf of CCGs –CSSs may consider LAs additional customers –CSSs may charge for analytical services that may not be available within the LA public health function, or charge for access to certain local data sets not available from national sources –The CSSs may rely on a small number of Data Management and Integration Centres to provide data services and these may not be ready by April 2013.")
11
1.CCGs, CSSs/DMICs & LA PH need to work together in a complementary manner to support CCGs and H&WBs achieve the best population outcomes for local populations 2.Need clear local agreements around access and storage of datasets 3.That where possible PH will use the same common data sources as CSSs and CCGs to facilitate a shared and consistent version of the truth and reduce duplication 4.That PH will have access to patient level datasets and aggregate data required to effectively carry out their roles. 5.Where ever possible de-identified patient level data will be used. 6.The need for PH analysts to manipulate postcode level data is acknowledged in order to undertake aspects of geographical analysis (outcome subject to IG review) 7.Patient level data suggested to be stored with DMICs where it can be linked with other data 8.Aggregate data can either be accessed directly, nationally or via CSS/DMICs if it is something widely used by a number of local agencies 9.Patient level data can only be shared where there is explicit approval / data sharing arrangement with CCGs 10.Additional linkage and cleansing of PH specific data will need to de defined: if they are to be delivered by DMIC, there may be a charge associated with value add services Some of the principles being discussed
 7.Patient level data suggested to be stored with DMICs where it can be linked with other data 8.Aggregate data can either be accessed directly, nationally or via CSS/DMICs if it is something widely used by a number of local agencies 9.Patient level data can only be shared where there is explicit approval / data sharing arrangement with CCGs 10.Additional linkage and cleansing of PH specific data will need to de defined: if they are to be delivered by DMIC, there may be a charge associated with value add services Some of the principles being discussed.")
12
Risk management PHE negotiation with Commissioning Board, Information Centre, ONS, NIGB LAs check connectivity, incl. access to N3 connections LAs work with their local CCGs and CSS to identify technical solution DPHs, LAs, using PH advice to NHS project, need to identify specific purposes for patient identifiable or record level data in LAs DPHs to ensure that proposed use of data has an explicit current legal basis and satisfies current NHS guidance on use of patient data Public Health England continues work on IG LAs consider complying with IG Toolkit Guidance from DH on the LA PH advice function to NHS commissioners needs to be more explicit about the relationship between LAs and CCGs as a single customer for the services of CSSs in relation to data access. NHS CB guidance to CCGs and shadow CSSs needs to clarify that CCGs will be expected to ensure that LAs have access to the data they need to provide advice to CCGs and the CB and that LAs will not be expected to pay CSSs for this function.

13
Key questions for local resolution by LA PH teams The proposed model assumes clear agreement and definition of roles, responsibilities and functions. In order to ensure viability at a local level, the following questions needs to be considered: 1.Does my LA have an SLA with local CCGs about public health intelligence (PHI)? 2.Will my LAPH be served by a CSS/DMIC? Do we have a contract with them to access required PHI data? 3.How much data processing and analysis are we (LAPH) planning to do in- house to provide the health care advice to CCG and the wider intelligence support to LA? 4.What data do we LA PH require access to? 5.What human resources, IT infrastructure do we require to access the data ? 6.If we will access data from CSS/DMIC, do our data analysts have the necessary skills to use sophisticated data warehouse applications (SQL, Oracle, business objects, data cubes)? Will they need training? 7.What may our SLA with our DMIC look like and how much will the service cost?
. 2.Will my LAPH be served by a CSS/DMIC. Do we have a contract with them to access required PHI data. 3.How much data processing and analysis are we (LAPH) planning to do in- house to provide the health care advice to CCG and the wider intelligence support to LA. 4.What data do we LA PH require access to. 5.What human resources, IT infrastructure do we require to access the data . 6.If we will access data from CSS/DMIC, do our data analysts have the necessary skills to use sophisticated data warehouse applications (SQL, Oracle, business objects, data cubes). Will they need training. 7.What may our SLA with our DMIC look like and how much will the service cost .")
14
Business model: Local authority public health intelligence Business model: Clinical Commissioning Group Business model: Commissioning Support Service/DMIC LA - what to do? Thorough description of public health advice and any other service SLA/MoU/ Compact SLA/MoU/ Compact SLA/MoU/ Compact

15
What next? Action plans Regional Workshops Today’s discussion: what should the PHE core offer to the local level contain? IDtask name deliverables/miles tones major dependencies Apr-12 May-12 Jun-12 Jul-12 Aug-12Sep-12 Oct-12 Nov-12Dec-12 Jan-13 Feb-13 Mar-13 1 a) Local model – relationship between LA/PH, HWB, CCGs, CSOs, providers, contractual framework, joint PHI work programme for commissioning, public health, local authority 2 b) Public health intelligence staff 3 · Final destination: 4 i. within the local council, as part of the public health team 5 ii. within the local council, as part of a council-wide intelligence and research capacity 6 iii. with the local (developing) Commissioning Support Organisation 7 · New job descriptions? Induction to new role? 8 · Governance (who is responsible for public health intelligence staff and their output?) 9 · Staff transfer 10 c) Public health intelligence budget 11 · Staff costs 12 · ICT transfer costs (connectivity, hardware, software incl. licences) 13 · PC maintenance on network 14 d) ICT migration proper from the PCT network to the Council (modalities, milestones); 15 · Dedicated programme manager in charge? 16 · Hardware, incl. mobile phones/other handheld devices 17 · Software (from PCT to LA network) 18 · Data held at PH/PCT level 19 · IG compliance 20 · Other, such as a commercial third party providing data management services? 21 e) Access to data 22 · IT connectivity (N3, NHS.net and the rest) 23 · IG, incl. data sharing 24 · Access to HES, SUS, QOF, IC, ONS, others
 Local model – relationship between LA/PH, HWB, CCGs, CSOs, providers, contractual framework, joint PHI work programme for commissioning, public health, local authority 2 b) Public health intelligence staff 3 · Final destination: 4 i. within the local council, as part of the public health team 5 ii. within the local council, as part of a council-wide intelligence and research capacity 6 iii. with the local (developing) Commissioning Support Organisation 7 · New job descriptions. Induction to new role. 8 · Governance (who is responsible for public health intelligence staff and their output ) 9 · Staff transfer 10 c) Public health intelligence budget 11 · Staff costs 12 · ICT transfer costs (connectivity, hardware, software incl. licences) 13 · PC maintenance on network 14 d) ICT migration proper from the PCT network to the Council (modalities, milestones); 15 · Dedicated programme manager in charge. 16 · Hardware, incl. mobile phones/other handheld devices 17 · Software (from PCT to LA network) 18 · Data held at PH/PCT level 19 · IG compliance 20 · Other, such as a commercial third party providing data management services. 21 e) Access to data 22 · IT connectivity (N3, NHS.net and the rest) 23 · IG, incl. data sharing 24 · Access to HES, SUS, QOF, IC, ONS, others.")
Similar presentations
 authorisation>")













 to pathfinders and emerging Clinical Commissioning Groups (CCGs) - What is it? Why should pathfinders.>")




