Download presentation
Presentation is loading. Please wait.

1
Artificial Lung Medical device to take over or supplement the respiratory function of the lungs. Used in cardiopulmonary bypass for open-heart surgery. Extracorporeal Membrane Oxygenation (ECMO) to treat respiratory insufficiency. Classification Extracorporeal : - External blood circuit, temporary support. - Currently used. - e.g. : CPB, EMO Paracorporeal : - Integrated pump/oxygenator. - Wearable. - Temporary to semi-pemanent.
 to treat respiratory insufficiency. Classification Extracorporeal : - External blood circuit, temporary support. - Currently used. - e.g. : CPB, EMO Paracorporeal : - Integrated pump/oxygenator. - Wearable. - Temporary to semi-pemanent..")
2
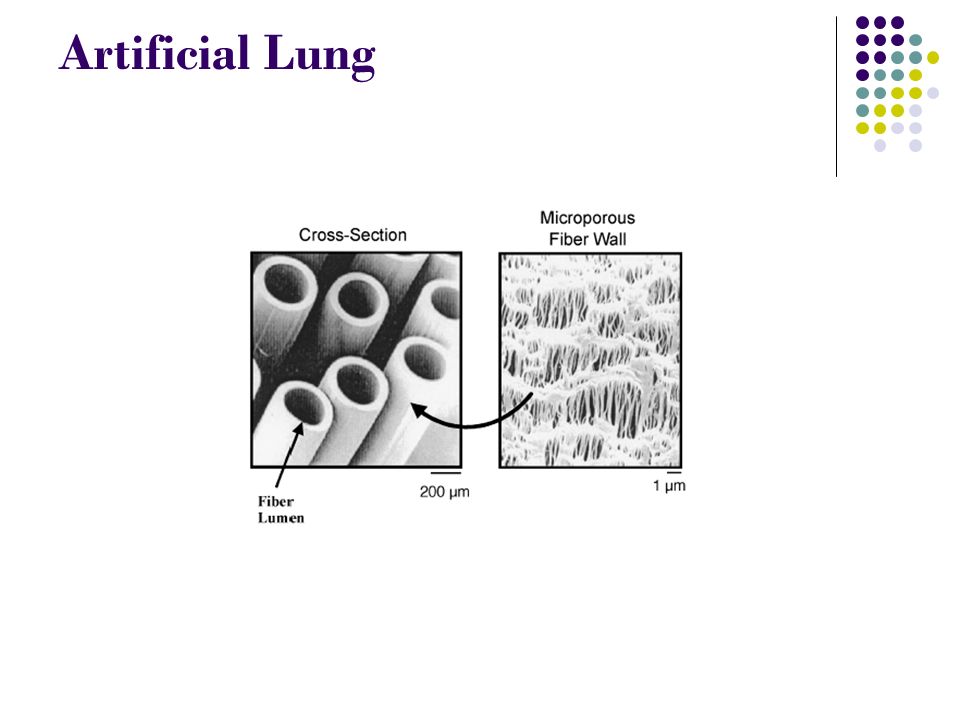
Artificial Lung Intracorporeal : - Surgical implant. - Percutaneous insertion. - Semi-permanent, temporary support. Hollow Fiber Hollow of fiber membranes form basic gas exchange unit. Small polymer tubes, microporous walls 20 to 50 um, outer diameters 200 to 400 um. Made of hydrophobic polymers, often polypropylene, so that membrane wall pores remain gas-filled and respiratory gases can diffuse readily across it. Principle Operation Oxygen (O2) ‘‘sweep gas’’ flows through the inside lumens of the hollow fibers. Blood flows outside the hollow fibers through spaces in the hollow fiber bundle
 ‘‘sweep gas’’ flows through the inside lumens of the hollow fibers. Blood flows outside the hollow fibers through spaces in the hollow fiber bundle.")
3
Artificial Lung Oxygen diffuses down its concentration gradient across the fiber wall into blood. Carbon dioxide (CO 2 ) diffuses down its concentration gradient from the blood into the sweep gas. CO 2 removed when the sweep gas exits the device. Gas Exchange O 2 exchange rate is : where K is gas exchange permeance. PO 2g and PO 2b are the average O 2 partial pressures in the sweep gas and blood phases. A is the total membrane area of the hollow fiber bundle. Similar to previous equation, CO 2 gas exchange rate is :
 diffuses down its concentration gradient from the blood into the sweep gas. CO 2 removed when the sweep gas exits the device. Gas Exchange O 2 exchange rate is : where K is gas exchange permeance. PO 2g and PO 2b are the average O 2 partial pressures in the sweep gas and blood phases. A is the total membrane area of the hollow fiber bundle. Similar to previous equation, CO 2 gas exchange rate is :.")
4
Artificial Lung Overall transfer resistance in artificial lung device : where Km and Kb are the membrane and blood-side permeances for each gas. 1/Km represents a diffusional resistance for the membrane. 1/Kb represents a resistance for gas diffusing between the membrane and the flowing blood stream. Membrane Permeance Microporous hollow fibers used as membrane. Fixed submicron pores within the membrane wall. Gas exchange occurs by diffusion through these gas-filled pores. Nature of hydrphobic polymers prevent blood plasma from entering fiber pores under normal condition.

5
Artificial Lung

7
Plasma Wetting A process in which blood plasma infiltrates the microporous walls of hollow fibers. A common problem when extracorporeal oxygenators are used in extended respiratory support. Can lead to device failure Diminishes membrane permeance, Km. Gas phase diffusion is replaced by diffusion through stagnant plasma within fiber pores. Even partial plasma infiltration into fiber membranes can reduce membrane permeance and degrade artificial lung performance. Composite Hollow Fiber Membrane To prevent plasma wetting. Incorporate a thin nonporous polymer layer as a true membrane or ‘‘skin’’ on the microporous fiber surface. True membrane blocks infiltration of plasma into pores

8
Artificial Lung

9
But, nonporous polymer skin diminishes membrane permeance because it can present an impediment to gas diffusion. Membrane permeance of a composite hollow fiber is dominated by the nonporous polymer layer. αp and Dp are the solubility and diffusivity of the gas within the nonporous polymer. δ is polymer layer thickness. Pm is the polymer permeability to specific gases. The design of composite hollow fiber membranes for artificial lungs requires a Km that does not significantly reduce overall gas exchange. Diffusional Boundary Layers Blood-side permeance :

10
Artificial Lung where αb and Db are the effective solubility and diffusion coefficient of the diffusing gas in blood. δbl is an average boundary layer thickness. Diffusional boundary layers exist adjacent to the fiber surfaces. At fiber surfaces, fluid velocity reduced by drag forces.

11
Artificial Lung Blood Oxygenator A type of artificial lung which is widely used. Consist of hollow fiber membrane. Some design use silicone sheet. How it works? Blood enters the oxygenator through an inlet port and flows either along the outside of the hollow fibers. Blood is then collected in a manifolded region, flows through a heat exchanger, and then exits the device through an outlet port. Gas can be pure oxygen or a mixture of oxygen and room air. Gas enters the oxygenator through a gas inlet port and flows through the inside of the hollow fibers. Than it exits the device via an outlet port. Often characterized by rated flow as a measure of gas exchange capacity of the device. Rated flow is flow rate through the oxygenator at which an inlet blood saturation of 70% can be oxygenated to outlet blood saturation of 95%.

12
Artificial Lung

14
Silicone Membrane Oxygenator Often used in extracorporeal membrane oxygenation for respiratory support. Plasma leakage does not occur. Silicone sheet is nonporous. Thus thickness of sheet reduced. Gas exchange efficiency below that of hollow membrane. Resistance to blood flow also higher.

15
Artificial Lung Natural Lungs vs Artificial Lung Natural Lungs : - Alveolar-capillary area : 100-150 m 2. - Surface to blood volume ratio : 300 cm -1. - Diffusion distance : 1-2 um. - Gas exchange rate : 200-250 ml/min at rest and 10-20 times under exercise. Artificial Lung : - Membrane area : 1-4 m 2. - Surface to blood volume ratio : 10 times less than natural lungs. - Diffusion distance : 10-30 um. - Gas exchange rate : 200-400 ml/min.

Similar presentations