Download presentation
Presentation is loading. Please wait.

1
THORACO-LUMBAR FRACTURES OF SPINE Presenter : Dr. Sunil santhosh.g Ms Ortho Narayana medical college

2
Anatomy: Cervical - 7 vertebrae Thoracic - 12 vertebrae Lumbar - 5 vertebrae Sacral - 5 fused vertebrae Coccyx - 4 fused vertebrae

4
Functional spinal unit Functional spinal unit is composed of two adjacent vertebrae Facet joint inter vertebral disc and intervening ligaments This unit is responsible for Movement of joint 4

5
Physiological Anatomy of the Thoracic Spine Facets lie in the frontal plane- allowing rotation Ribs resist rotation and add 3x the normal stiffness in lateral rotation Kyphosis of the T spine loads the anterior column Lower 2 vertebra have floating ribs and no costotransverse articulations Canal size in thoracic spine relatively small

6
Physiological Anatomy of the Lumbar Spine Large discs allow more ROM Facets prevent rotation as they aranged in saggital plain Spinal canal wider Lordosis loads the facets

7
Thoracolumbar Junction The susceptibility of the thoracolumbar junction to injury is attributed mainly to the following anatomical reasons: The transition from a relatively rigid thoracic kyphosis to a more mobile lumbar lordosis occurs at T11–12. The lowest thoracic ribs (T11 and T12) provide less stability at the thoracolumbar junction region compared to the upper thoracic region, because they do not connect to the sternum and are free floating.
 provide less stability at the thoracolumbar junction region compared to the upper thoracic region, because they do not connect to the sternum and are free floating..")
8
The facet joints of the thoracic region are oriented in the coronal (frontal) plane, limiting flexion and extension. In the lumbosacral region, the facetjoints are oriented in a more sagittal alignment, which increases the degree of potential flexion and extension

9
ETIOLOGY High energy trauma Fall from height Sports accident Violent act, such as a gunshot wound osteoporosis tumors other underlying conditions that weaken bone

10
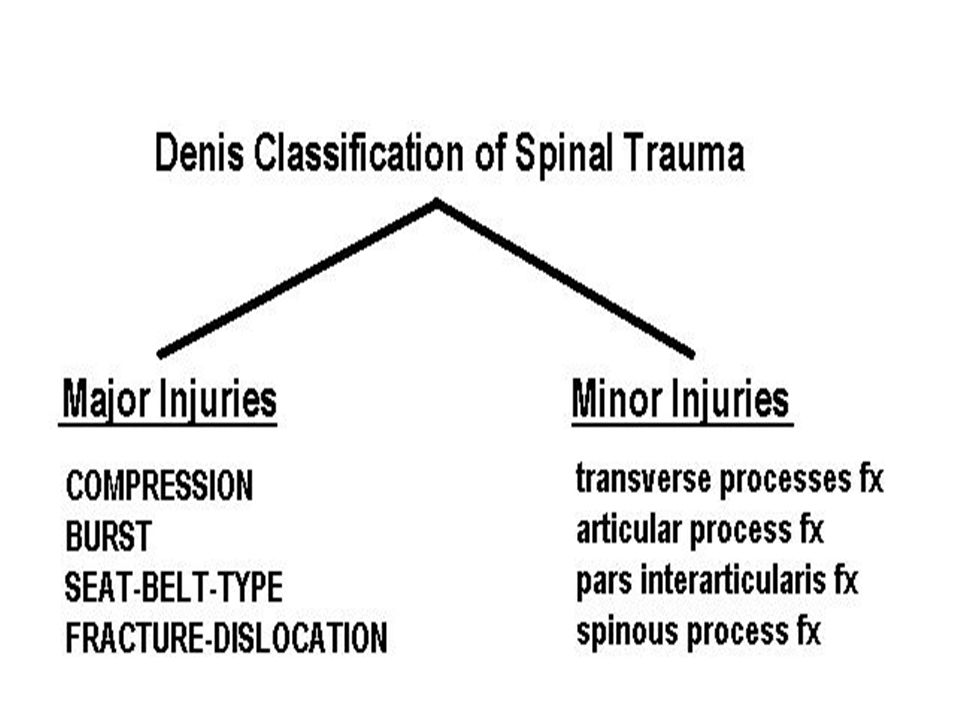
CLASSIFICATION

11
Denis Three column theory : The vertebral column is divided into three columns 1.ANTERIOR 2.MIDDLE 3.POSTERIOR Columns

12
Anterior column : anterior longitudinal ligament, the anterior half of the vertebral body and the anterior portion of the annulus fibrosus.

13
Middle column posterior longitudinal ligament, the posterior half of the vertebral body and the posterior aspect of the annulus fibrosus.

14
posterior column : the neural arch, ligamentum flavum, the facet joint, and the interspinous ligaments

16
COMPRESSION FRACTURE: Results from Anterior or lateral flexion Failure of anterior column The middle column is intact and acts as a hinge. There may be a partial failure of the posterior column, indicating the tension forces at that level. Usually no Neurological deficits are noted.

17
4 subtypes on basis of end plate involvement # of both end plates # of superior end plate # of inferior end plate both end plates intact

18
Burst fractures Occurs due to Axial compression resulting in Failure of anterior and middle column If posterior column involved results in instability Most common at T/L junction

19
5 subtypes on basis of end plate involvement # of both end plates # of superior end plate #of inferior end plate both end plates intact Burst lateral flexion

20
FLEXION-DISTRACTION OR SEAT-BELT- TYPE INJURY or CHANCE # Both posterior and middle columns fail due to hyper-flexion and subsequent tension forces. The anterior part of the anterior column may partially damaged under compression, but still functions like a hinge.

21
Fracture- Dislocation Presents with failure of all three columns under compression, tension, rotation, or shear. It is similar to seat-belt-type injury. However, the anterior hinge is also disrupted and some degree of dislocation is present.

22
Three subtypes of fracture-dislocations based on mechanism of injury: flexion rotation Flexion-distraction Shear type

23
flexion rotation: There is a complete disruption of the posterior and middle columns under tension and rotation. The anterior column in rotation or compression and rotation.

24
Flexion-distraction Tension failure of posterior and middle columns. With tear of the anterior annulus fibrosus, and stripping of the anterior longitudinal ligament. Neurological deficit(75%)
.")
25
Shear : Shear failure of all three columns, commonly in postero- anterior direction All cases present with neurologic deficit

26
AO/MAGREL CLASSIFICATION A B C 123

27
Thoracolumbar Injury Classification and Severity Score POINTS FRACTURE MECHANISM Compression fracture 1 Burst fracture 1 Translation/rotation 3 Distraction 4 NEUROLOGICAL INVOLVEMENT Intact 0 Nerve root 2 Cord, conus medullaris, incomplete 3 Cord, conus medullaris, complete 2 Cauda equina 3 POSTERIOR LIGAMENTOUS COMPLEX INTEGRITY Intact 0 Injury suspected/indeterminate 2 Injured 3

28
SPINAL STABILITY Spinal injury is considered unstable if normal physiological load cause further neurological damage, chronic pain & deformity Instability exists if any of two columns are disrupted In T-L stability if middle column is intact, # is usually stable.

29
Three Degrees of instability: First degree : (Mechanical instability): Severe compression # Seat belt injury Second degree: (Neurological instability) Burst # with out neurological deficit Third degree : (Both) Burst # with neurological deficit Fracture dislocation
: Severe compression # Seat belt injury Second degree: (Neurological instability) Burst # with out neurological deficit Third degree : (Both) Burst # with neurological deficit Fracture dislocation")
30
Clinical presentation History The history of a patient who sustained a thoracolumbar spinal injury is usually obvious. The cardinal symptoms are: pain loss of function (inability to move) sensorimotor deficit bowel and bladder dysfunction
 sensorimotor deficit bowel and bladder dysfunction.")
31
The history should include a detailed assessment of the injury, i.e.: type of trauma (high vs. low energy) mechanism of injury (compression, flexion/distraction, hyperextension, rotation, shear injury)
 mechanism of injury (compression, flexion/distraction, hyperextension, rotation, shear injury).")
32
In patients with neurological deficits, the history must be detailed regarding: time of onset course (unchanged, progressive, or improving)
")
33
Concomitant Non-spinal Injuries one-third of all spine injuries have concomitant injuries Most frequently found concomitant injuries are: 1. head injuries (26%) 2. chest injuries (24%) 3. long bone injuries (23%)
 2. chest injuries (24%) 3. long bone injuries (23%).")
34
Physical Findings The inspection and palpation of the spine should include the search for: swellings Tenderness skin bruises, lacerations, ecchymoses open wounds hematoma spinal (mal)alignment
alignment")
35
Neurological evaluation : ASIA form is used to record the neurological findings Neurological deficit of the patient Depends upon Complete or incomplete injury of the cord.

36
Complete - flaccid paralysis + total loss of sensory & motor functions Incomplete - mixed loss - Anterior sc syndrome - Posterior sc syndrome - Central cord syndrome - Brown sequard’s syndrome - Cauda equina syndrome 36

37
Dermatomal Sensory Testing

38
Lumbar and Sacral Motor Root Function

39
Reflex Examination

40
Grading of Spinal Cord Injury 40

41
Investigations : plain X-rays, CT and MRI studies X-RAYS A-P & Lateral views

42
Antero-posterior view loss of lateral vertebral body height changes in horizontal and vertical interpedicular distance irregular distance between the spinous processes (equivocal sign)
")
43
asymmetry of the spinal alignment subluxation of costotransverse articulations perpendicular or oblique fractures of the dorsal elements

44
Lateral view sagittal profile degree of vertebral body compression height of the intervertebral space

45
interruption or bulging of the posterior line of the vertebral body dislocation of a dorsoapical fragment

46
CT : The axial view allows an accurate assessment of the comminution of the fracture and dislocation of fragments into the spinal canal.

47
Sagittal andcoronal 2D or 3D reconstructions are helpful for determining the fracture pattern

48
MRI : In the presence of neurological deficits, MRI is recommended to identify a possible cord lesion or a cord compression that may be due to disc or fracture fragments or epidural hematoma

49
MRI can be helpful in determining the integrity of the posterior ligamentous structures and thereby differentiate between a stable and an unstable lesion.

Similar presentations