Download presentation
Presentation is loading. Please wait.

2
تجویز منطقی دارو در دیابت نوع 2 ارائه توسط : دکتر نوشین خلیلی فوق تخصص غدد عضو هیئت علمی دانشکده پزشکی اصفهان

3
شعار WHO: غلبه بر دیابت

4
1. BACKGROUND Overview of the pathogenesis of Type 2 diabetes 2. ANTI-HYPERGLYCEMIC THERAPY Glycemic targets Therapeutic options - Oral agents & non-insulin injectables - Insulin Diabetes Care 2012;35:1364–1379; Diabetologia 2012;55:1577–1596 Diabetes Care 2015;38:140-149; Diabetologia 2015;58:429-442

6
Type 2 diabetes is a chronic metabolic condition characterised by insulin resistance that is, the body's inability to effectively use insulin and insufficient pancreatic insulin production, resulting in high blood glucose levels (hyperglycaemia).
.")
7
Criteria for the diagnosis of diabetes

8
FPG≥126 mg/dL (7.0 mmol/L). Fasting is defined as no caloric intake for at least 8h.* OR 2-h PG ≥ 200 mg/dL (11.1mmol/L) during an OGTT. OR A1C ≥ 6.5% (48 mmol/mol). OR In a patient with classic symptoms of hyperglycemia or hyperglycemic crisis, a random plasma glucose ≥ 200 mg/dL (11.1 mmol/L). *In the absence of unequivocal hyperglycemia, results should be confirmed by repeat testing.
 during an OGTT. OR A1C ≥ 6.5% (48 mmol/mol). OR In a patient with classic symptoms of hyperglycemia or hyperglycemic crisis, a random plasma glucose ≥ 200 mg/dL (11.1 mmol/L). *In the absence of unequivocal hyperglycemia, results should be confirmed by repeat testing..")
9
Overview of the pathogenesis of T2DM - Insulin secretory dysfunction - Insulin resistance (muscle, fat, liver) - Increased endogenous glucose production - Decreased incretin effect - Deranged adipocyte biology Diabetes Care 2012;35:1364–1379; Diabetologia 2012;55:1577–1596
 - Increased endogenous glucose production - Decreased incretin effect - Deranged adipocyte biology Diabetes Care 2012;35:1364–1379; Diabetologia 2012;55:1577–1596")
10
peripheral glucose uptake hepatic glucose production pancreatic insulin secretion pancreatic glucagon secretion gut carbohydrate delivery & absorption incretin effect HYPERGLYCEMIA ? Adapted from: Inzucchi SE, Sherwin RS in: Cecil Medicine 2011 Multiple, Complex Pathophysiological Abnormalities in T2DM _ _ + renal glucose excretion

11
peripheral glucose uptake hepatic glucose production pancreatic insulin secretion pancreatic glucagon secretion gut carbohydrate delivery & absorption incretin effect HYPERGLYCEMIA ? Adapted from: Inzucchi SE, Sherwin RS in: Cecil Medicine 2011 Multiple, Complex Pathophysiological Abnormalities in T2DM _ _ + renal glucose excretion DA agonists T Z D s Metformin S U s Glinides DPP-4inhibitors GLP-1Ragonists A G I s Amylinmimetics Insulin Bile acid sequestrants SGLT2 I

12
2. ANTI-HYPERGLYCEMIC THERAPY Glycemic targets HbA1c < 7.0% (mean PG 150-160 mg/dl [8.3-8.9 mmol/l ]) - Pre-prandial PG <130 mg/dl (7.2 mmol/l ) - Post-prandial PG <180 mg/dl (10.0 mmol/l ) - Individualization is key: Tighter targets (6.0 - 6.5%) - younger, healthier Looser targets (7.5 - 8.0% + ) - older, comorbidities, hypoglycemia prone, etc. - Avoidance of hypoglycemia PG = plasma glucose Diabetes Care 2012;35:1364–1379; Diabetologia 2012;55:1577–1596 Diabetes Care 2015;38:140-149; Diabetologia 2015;58:429-442
 - Pre-prandial PG <130 mg/dl (7.2 mmol/l ) - Post-prandial PG <180 mg/dl (10.0 mmol/l ) - Individualization is key: Tighter targets ( %) - younger, healthier Looser targets ( % + ) - older, comorbidities, hypoglycemia prone, etc. - Avoidance of hypoglycemia PG = plasma glucose Diabetes Care 2012;35:1364–1379; Diabetologia 2012;55:1577–1596 Diabetes Care 2015;38: ; Diabetologia 2015;58:")
13
From guidelines to individual My resident called to inform me that we had just received a new admission with a broken hip Mr. O, an 86 -year –old man, He worked all his life and was still able to take on smaller jobs, such as cutting grass, for pay. He and his older brother, aged 92,lived together. brothers never married and his older brother began to develop dementia, Mr. O was his brother's primary caretaker. Mr. O had never had a serious illness and had not seen doctors until he received his Medicare card. Mr. O’s first encounter with a physician was when he was a robust 80-year- old on no medications. Initial blood pressure was 150/96 mmHg, and he had no abnormalities on physical examination.

14
Baseline laboratories showed a blood glucose of 180 mg/dL. Eye grounds were not examined, ECG was normal, and he had no bruits in his neck. He was advised to come back for a fasting glucose test and total lipids. The repeated blood sugar was 170 mg/dl, cholesterol was 220mg/dl,and A1c was 8.5% Initial therapy consisted of an ACE inhibitor and metformin, and he was seen every 3 months to adjust medications. Both the blood pressure and the A1c remained stubbornly elevated, and a calcium-channel blocker was prescribed. A second oral hypoglycemic agent was started in an attempt to further reduce his A1c. When he began to get up every 2 hours to urinate at night, doxazosin was initiated. It was at that time that he became lightheaded on rising from the sitting position.

15
During the next visit, his new physician gave him a brochure and a copy of the first supplement of American Diabetes Association His systolic blood pressure remained in the 150- to 160-mm Hg range, and his A1c was stuck at 8.5%. Long acting insulin was started. Soon afterward, he developed nightmares and noticed unsteadiness when he got up at night to urinate. His A1c was unchanged at 8%, his blood pressure was 154/92 mm Hg, and his dose of the calcium-channel blocker was doubled. All of these changes occurred about 3 weeks before admission to our hospital.

16
The night before admission, he got up to urinate, fell, and broke his hip. He was able to reach the telephone to call the local volunteer fire department. When the paramedics arrived, his systolic blood pressure was 80 mm Hg and the diastolic pressure was too low to register. His blood sugar was 40 mg/dL, and he was given 50% glucose solution with immediate improvement of all altered vital signs. He was transferred from the local hospital to my hospital, where on admission he was alert and oriented and in pain from the broken hip. His creatinine level was 1.2 mg/dL (the previous level was 0.9 mg/dL).
..")
17
About 16 hours after the fall and fracture, he was taken to the operating room, where he had a total hip arthroplasty under general anesthesia lasting a little more than 2 hours. While in the recovery room, he was noted to have difficulty using his right hand and was not speaking clearly. Over the next few hours, it became clear that he had a cerebrovascular accident. He had a stormy postoperative course with multiple complications, including C. difficile colitis and an increase of creatinine to 2.0 mg/dL. He was started on physical therapy and eventually transferred to a rehabilitation facility where he remained 3 months after the fall, unlikely to ever live independently. Meanwhile, his brother with dementia had to be admitted to a nursing home with a memory care unit. During this ordeal, Mr. O exhausted his meager savings and required Medicaid funding, which resulted in a lien being placed on his home.

18
In retrospect, he got into a relentless downhill medical care spiral fueled by interventions based on “evidence-based” guidelines to tightly control both the blood sugar and the blood pressure—well-known targets on which physicians' performances are judged. His doctor may have received a bonus for adhering to the guidelines, but Mr. O lost his home and independence.

19
Diabetes Care 2015;38:140-149; Diabetologia 2015;58:429-442 Figure 1. Modulation of the intensiveness of glucose lowering therapy in T2DM

20
Diabetes Care 2015;38:140-149; Diabetologia 2015;58:429-442

21
Figure 1. Modulation of the intensiveness of glucose lowering therapy in T2DM Diabetes Care 2015;38:140-149; Diabetologia 2015;58:429-442

22
Figure 1. Modulation of the intensiveness of glucose lowering therapy in T2DM Diabetes Care 2015;38:140-149; Diabetologia 2015;58:429-442

23
Figure 1. Modulation of the intensiveness of glucose lowering therapy in T2DM Diabetes Care 2015;38:140-149; Diabetologia 2015;58:429-442

24
Figure 1. Modulation of the intensiveness of glucose lowering therapy in T2DM Diabetes Care 2015;38:140-149; Diabetologia 2015;58:429-442

25
Figure 1. Modulation of the intensiveness of glucose lowering therapy in T2DM Diabetes Care 2015;38:140-149; Diabetologia 2015;58:429-442

26
Figure 1. Modulation of the intensiveness of glucose lowering therapy in T2DM Diabetes Care 2015;38:140-149; Diabetologia 2015;58:429-442

27
2. ANTI-HYPERGLYCEMIC THERAPY Therapeutic options: Lifestyle - Weight optimization - Healthy diet - Increased activity level Diabetes Care 2012;35:1364–1379; Diabetologia 2012;55:1577–1596

28
3. ANTI-HYPERGLYCEMIC THERAPY Therapeutic options: Oral agents & non - insulin injectables - Metformin - Sulfonylureas - Thiazolidinediones - DPP-4 inhibitors - SGLT-2 inhibitors - GLP-1 receptor agonists - Meglitinides - - glucosidase inhibitors - Colesevelam - Dopamine-2 agonists - Amylin mimetics Diabetes Care 2012;35:1364–1379; Diabetologia 2012;55:1577–1596 Diabetes Care 2015;38:140-149; Diabetologia 2015;58:429-442

29
Oral Class MechanismAdvantagesDisadvantagesCost Biguanides Activates AMP- kinase (?other) Hepatic glucose production Extensive experience No hypoglycemia Weight neutral ? CVD Gastrointestinal Lactic acidosis (rare) B-12 deficiency Contraindications Low Sulfonylureas Closes K ATP channels Insulin secretion Extensive experience Microvascular risk Hypoglycemia Weight Low durability ? Blunts ischemic preconditioning Low Meglitinides Closes K ATP channels Insulin secretion Postprandial glucose Dosing flexibility Hypoglycemia Weight ? Blunts ischemic preconditioning Dosing frequency Mod. TZDs PPAR- activator Insulin sensitivity No hypoglycemia Durability TGs (pio) HDL-C ? CVD events (pio) Weight Edema/heart failure Bone fractures LDL-C (rosi) ? MI (rosi) Low Table 1. Properties of anti-hyperglycemic agents Diabetes Care 2015;38:140-149; Diabetologia 2015;58:429-442
 B-12 deficiency Contraindications Low Sulfonylureas Closes K ATP channels Insulin secretion Extensive experience Microvascular risk Hypoglycemia Weight Low durability . Blunts ischemic preconditioning Low Meglitinides Closes K ATP channels Insulin secretion Postprandial glucose Dosing flexibility Hypoglycemia Weight . Blunts ischemic preconditioning Dosing frequency Mod. TZDs PPAR- activator Insulin sensitivity No hypoglycemia Durability TGs (pio) HDL-C . CVD events (pio) Weight Edema/heart failure Bone fractures LDL-C (rosi) . MI (rosi) Low Table 1. Properties of anti-hyperglycemic agents Diabetes Care 2015;38: ; Diabetologia 2015;58:")
30
Oral Class MechanismAdvantagesDisadvantagesCost -Glucosidase inhibitors Inhibits -glucosidase Slows carbohydrate digestion / absorption No hypoglycemia Nonsystemic Postprandial glucose ? CVD events Gastrointestinal Dosing frequency Modest A1c Mod. DPP-4 inhibitors Inhibits DPP-4 Increases incretin (GLP-1, GIP) levels No hypoglycemia Well tolerated Angioedema / urticaria ? Pancreatitis ? Heart failure High Bile acid sequestrants Bind bile acids ? Hepatic glucose production No hypoglycemia LDL-C Gastrointestinal Modest A1c Dosing frequency High Dopamine-2 agonists Activates DA receptor Alters hypothalamic control of metabolism insulin sensitivity No hypoglyemia ? CVD events Modest A1c Dizziness, fatigue Nausea Rhinitis High SGLT2 inhibitors Inhibits SGLT2 in proximal nephron Increases glucosuria Weight No hypoglycemia BP Effective at all stages GU infections Polyuria Volume depletion LDL-C Cr (transient) High Table 1. Properties of anti-hyperglycemic agents Diabetes Care 2015;38:140-149; Diabetologia 2015;58:429-442
 levels No hypoglycemia Well tolerated Angioedema / urticaria . Pancreatitis . Heart failure High Bile acid sequestrants Bind bile acids . Hepatic glucose production No hypoglycemia LDL-C Gastrointestinal Modest A1c Dosing frequency High Dopamine-2 agonists Activates DA receptor Alters hypothalamic control of metabolism insulin sensitivity No hypoglyemia . CVD events Modest A1c Dizziness, fatigue Nausea Rhinitis High SGLT2 inhibitors Inhibits SGLT2 in proximal nephron Increases glucosuria Weight No hypoglycemia BP Effective at all stages GU infections Polyuria Volume depletion LDL-C Cr (transient) High Table 1. Properties of anti-hyperglycemic agents Diabetes Care 2015;38: ; Diabetologia 2015;58:")
31
Injectabl e ClassMechanismAdvantagesDisadvantagesCost Amylin mimetics Activates amylin receptor glucagon gastric emptying satiety Weight Postprandial glucose Gastrointestinal Modest A1c Injectable Hypo if insulin dose not reduced Dosing frequency Training requirements High GLP-1 receptor agonists Activates GLP-1 R Insulin, glucagon gastric emptying satiety Weight No hypoglycemia Postprandial glucose Some CV risk factors Gastrointestinal ? Pancreatitis Heart rate Medullary ca (rodents) Injectable Training requirements High Insulin Activates insulin receptor Myriad Universally effective Unlimited efficacy Microvascular risk Hypoglycemia Weight gain ? Mitogenicity Injectable Patient reluctance Training requirements Variable Table 1. Properties of anti-hyperglycemic agents Diabetes Care 2015;38:140-149; Diabetologia 2015;58:429-442
 Injectable Training requirements High Insulin Activates insulin receptor Myriad Universally effective Unlimited efficacy Microvascular risk Hypoglycemia Weight gain . Mitogenicity Injectable Patient reluctance Training requirements Variable Table 1. Properties of anti-hyperglycemic agents Diabetes Care 2015;38: ; Diabetologia 2015;58:")
32
Noninsulin Agents Available for T2D ClassPrimary Mechanism of ActionAgent(s)Available as -Glucosidase inhibitors Delay carbohydrate absorption from intestine Acarbose Miglitol Precose or generic Glyset Amylin analogue Decrease glucagon secretion Slow gastric emptying Increase satiety PramlintideSymlin Biguanide Decrease HGP Increase glucose uptake in muscle MetforminGlucophage or generic Bile acid sequestrant Decrease HGP? Increase incretin levels? ColesevelamWelChol DPP-4 inhibitors Increase glucose-dependent insulin secretion Decrease glucagon secretion Alogliptin Linagliptin Saxagliptin Sitagliptin Nesina Tradjenta Onglyza Januvia Dopamine-2 agonist Activates dopaminergic receptors BromocriptineCycloset Glinides Increase insulin secretion Nateglinide Repaglinide Starlix or generic Prandin DPP-4 = dipeptidyl peptidase; HGP = hepatic glucose production. Garber AJ, et al. Endocr Pract. 2013;19(suppl 2):1-48. Inzucchi SE, et al. Diabetes Care. 2012;35:1364-1379. Continued on next slide
:1-48. Inzucchi SE, et al. Diabetes Care. 2012;35: Continued on next slide.")
33
Noninsulin Agents Available for T2D ClassPrimary Mechanism of ActionAgent(s)Available as GLP-1 receptor agonists Increase glucose-dependent insulin secretion Decrease glucagon secretion Slow gastric emptying Increase satiety Albiglutide Dulaglutide Exenatide Exenatide XR Liraglutide Tanzeum Trulicity Byetta Bydureon Victoza SGLT2 inhibitors Increase urinary excretion of glucose Canagliflozin Dapagliflozin Empagliflozin Invokana Farxiga Jardiance Sulfonylureas Increase insulin secretion Glimepiride Glipizide Glyburide Amaryl or generic Glucotrol or generic Dia eta, Glynase, Micronase, or generic Thiazolidinediones Increase glucose uptake in muscle and fat Decrease HGP Pioglitazone Rosiglitazone Actos Avandia GLP-1 = glucagon-like peptide; HGP = hepatic glucose production; SGLT2 = sodium glucose cotransporter 2. Garber AJ, et al. Endocr Pract. 2013;19(suppl 2):1-48. Inzucchi SE, et al. Diabetes Care. 2012;35:1364-1379. Continued from previous slide
:1-48. Inzucchi SE, et al. Diabetes Care. 2012;35: Continued from previous slide.")
34
Effects of Agents Available for T2D AGI = -glucosidase inhibitors; BCR-QR = bromocriptine quick release; Coles = colesevelam; DPP4I = dipeptidyl peptidase 4 inhibitors; FPG = fasting plasma glucose; GLP1RA = glucagon-like peptide 1 receptor agonists; Met = metformin; Mod = moderate; PPG = postprandial glucose; SGLT2I = sodium-glucose cotransporter 2 inhibitors; SU = sulfonylureas; TZD = thiazolidinediones. *Mild: albiglutide and exenatide; moderate: dulaglutide, exenatide extended release, and liraglutide. MetGLP1RASGLT2IDPP4ITZDAGIColesBCR-QR SU/ Glinide InsulinPram FPG lowering Mod Mild to mod* ModMildModNeutralMildNeutral SU: mod Glinide: mild Mod to marked (basal insulin or premixed) Mild PPG lowering Mild Mod to marked MildModMildModMild Mod Mod to marked (short/ rapid- acting insulin or premixed) Mod to marked Continued on next slide
 Mild PPG lowering Mild Mod to marked MildModMildModMild Mod Mod to marked (short/ rapid- acting insulin or premixed) Mod to marked Continued on next slide.")
35
Effects of Agents Available for T2D AGI = -glucosidase inhibitors; BCR-QR = bromocriptine quick release; Coles = colesevelam; DPP4I = dipeptidyl peptidase 4 inhibitors; GLP1RA = glucagon-like peptide 1 receptor agonists; Met = metformin; Mod = moderate; NAFLD, nonalcoholic fatty liver disease; SGLT2I = sodium-glucose cotransporter 2 inhibitors; SU = sulfonylureas; TZD = thiazolidinediones. *Especially with short/ rapid-acting or premixed. MetGLP1RASGLT2IDPP4ITZDAGIColesBCR-QR SU/ Glinide InsulinPram NAFLD benefitMild Neutral ModNeutral Hypo- glycemia Neutral SU: mod to severe Glinide: mild to mod Mod to severe* Neutral WeightSlight lossLoss NeutralGainNeutral Gain Loss Continued from previous slide

36
Effects of Agents Available for T2D MetGLP1RASGLT2IDPP4ITZDAGIColesBCR-QR SU/ Glinide InsulinPram Renal impair- ment/ GU Contra- indicated in stage 3B, 4, 5 CKD Exenatide contra- indicated CrCl <30 mg/mL GU infection risk Dose adjust- ment (except lina- gliptin) May worsen fluid retention Neutral Increased hypo- glycemia risk Increased risks of hypo- glycemia and fluid retention Neutral GI adverse effects ModMod*NeutralNeutral*NeutralModMildModNeutral Mod CHFNeutral Neutral † ModNeutral CVD Possible benefit Neutral Safe?Neutral BoneNeutral Bone lossNeutral Mod bone loss Neutral Continued from previous slide AGI = -glucosidase inhibitors; BCR-QR = bromocriptine quick release; Coles = colesevelam; CHF = congestive heart failure; CVD = cardiovascular disease; DPP4I = dipeptidyl peptidase 4 inhibitors; GI = gastrointestinal; GLP1RA = glucagon-like peptide 1 receptor agonists; GU = genitourinary; Met = metformin; Mod = moderate; SGLT2I = sodium-glucose cotransporter 2 inhibitors; SU = sulfonylureas; TZD = thiazolidinediones. *Caution in labeling about pancreatitis. † Caution: possibly increased CHF hospitalization risk seen in CV safety trial.

37
Monotherapy, Dual Therapy, and Triple Therapy for T2D 37 Q4. How are glycemic targets achieved for T2D? AGI = -glucosidase inhibitors; BCR-QR = bromocriptine quick release; Coles = colesevelam; DPP4I = dipeptidyl peptidase 4 inhibitors; GLP1RA = glucagon-like peptide 1 receptor agonists; Met = metformin; SGLT2I = sodium-glucose cotransporter 2 inhibitors; SU = sulfonylureas; TZD = thiazolidinediones. *Intensify therapy whenever A1C exceeds individualized target. Boldface denotes little or no risk of hypoglycemia or weight gain, few adverse events, and/or the possibility of benefits beyond glucose-lowering. † Use with caution. Monotherapy*Dual therapy* Metformin (or other first- line agent) plus Triple therapy* First- and second-line agent plus MetforminGLP1RA SGLT2I DPP4ITZD † DPP4ITZD † Basal insulin † AGIBasal insulin † DPP4I TZD † Colesevelam SU/glinide † BCR-QR AGI SU/glinide †
 plus Triple therapy* First- and second-line agent plus MetforminGLP1RA SGLT2I DPP4ITZD † DPP4ITZD † Basal insulin † AGIBasal insulin † DPP4I TZD † Colesevelam SU/glinide † BCR-QR AGI SU/glinide †.")
38
Figure 2. Anti-hyperglycemic therapy in T2DM: General recommendations Diabetes Care 2015;38:140-149; Diabetologia 2015;58:429-442

39
Figure 2. Anti-hyperglycemic therapy in T2DM: General recommendations Diabetes Care 2015;38:140-149; Diabetologia 2015;58:429-442

40
Figure 2. Anti-hyperglycemic therapy in T2DM: General recommendations Diabetes Care 2015;38:140-149; Diabetologia 2015;58:429-442

42
HbA1c ≥9% Metformin intolerance or contraindicati on Uncontrolled hyperglycemia (catabolic features, BG ≥300-350 mg/dl, HbA1c ≥10- 12%)
")
43
Figure 2A. Anti- hyperglycemic therapy in T2DM: Avoidance of hypoglycemia Diabetes Care 2015;38:140-149; Diabetologia 2015;58:429-442

44
Figure 2B. Anti- hyperglycemic therapy in T2DM: Avoidance of weight gain

45
Figure 2C. Anti- hyperglycemic therapy in T2DM: Minimization of costs Diabetes Care 2015;38:140-149; Diabetologia 2015;58:429-442

46
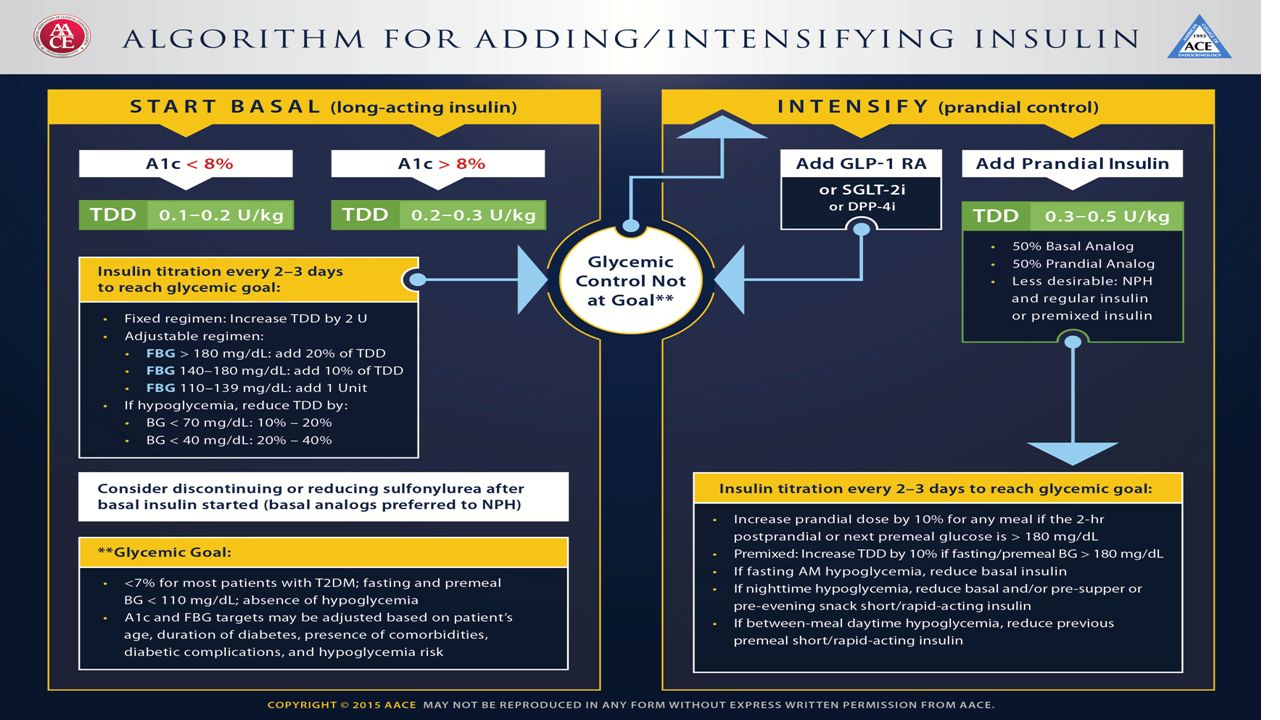
Therapeutic option s: Insulins Human Insulins - Neutral protamine Hagedorn (NPH) - Regular human insulin - Pre-mixed formulations Insulin Analogues - Basal analogues (glargine, detemir, degludec) - Rapid analogues (lispro, aspart, glulisine) - Pre-mixed formulations Diabetes Care 2012;35:1364–1379; Diabetologia 2012;55:1577–1596 Diabetes Care 2015;38:140-149; Diabetologia 2015;58:429-442
 - Regular human insulin - Pre-mixed formulations Insulin Analogues - Basal analogues (glargine, detemir, degludec) - Rapid analogues (lispro, aspart, glulisine) - Pre-mixed formulations Diabetes Care 2012;35:1364–1379; Diabetologia 2012;55:1577–1596 Diabetes Care 2015;38: ; Diabetologia 2015;58:")
47
Long (Detemir) Rapid (Lispro, Aspart, Glulisine) Hours Long (Glargine) 0 2 4 6 8 10 12 14 16 18 20 22 24 Short (Regular) Hours after injection Insulin level (Degludec) 3. ANTI-HYPERGLYCEMIC THERAPY Therapeutic option s: Insulins

48
Rapid analogues (lispro, aspart, glulisine)
")
49
Basal analogues (glargine, detemir, degludec )
")
51
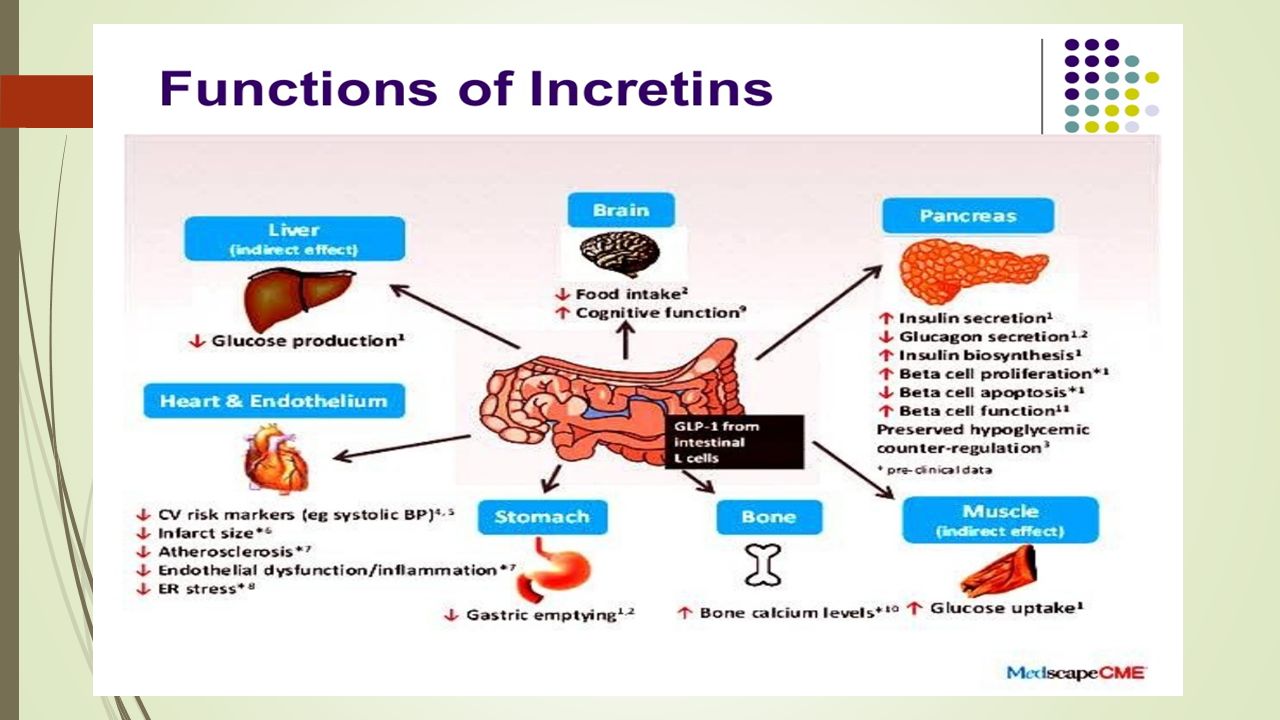
Dipeptidyl peptidase 4 (DPP-4) inhibitors Glucagon-like peptide-1 (GLP-1) is produced from the proglucagon gene in L-cells of the small intestine and is secreted in response to nutrients. GLP-1 exerts its main effect by stimulating glucose-dependent insulin release from the pancreatic islets It has also been shown to slow gastric emptying inhibit inappropriate post-meal glucagon release and reduce food intake.

52
GLP-1 Has a Short Duration of Effect Due to Degradation by Dipeptidyl Peptidase IV (DPP-IV) HisAlaGluGlyThrPheThrSerAsp LysAla GlnGlyGluLeuTyrSer IleAlaTrpLeuVal Lys GlyArgGly Val Ser Glu Phe Lys DPP-IV 7 37 9 Adapted from Mentlein R. Eur. J. Biochem 1993;214:829-835.

53
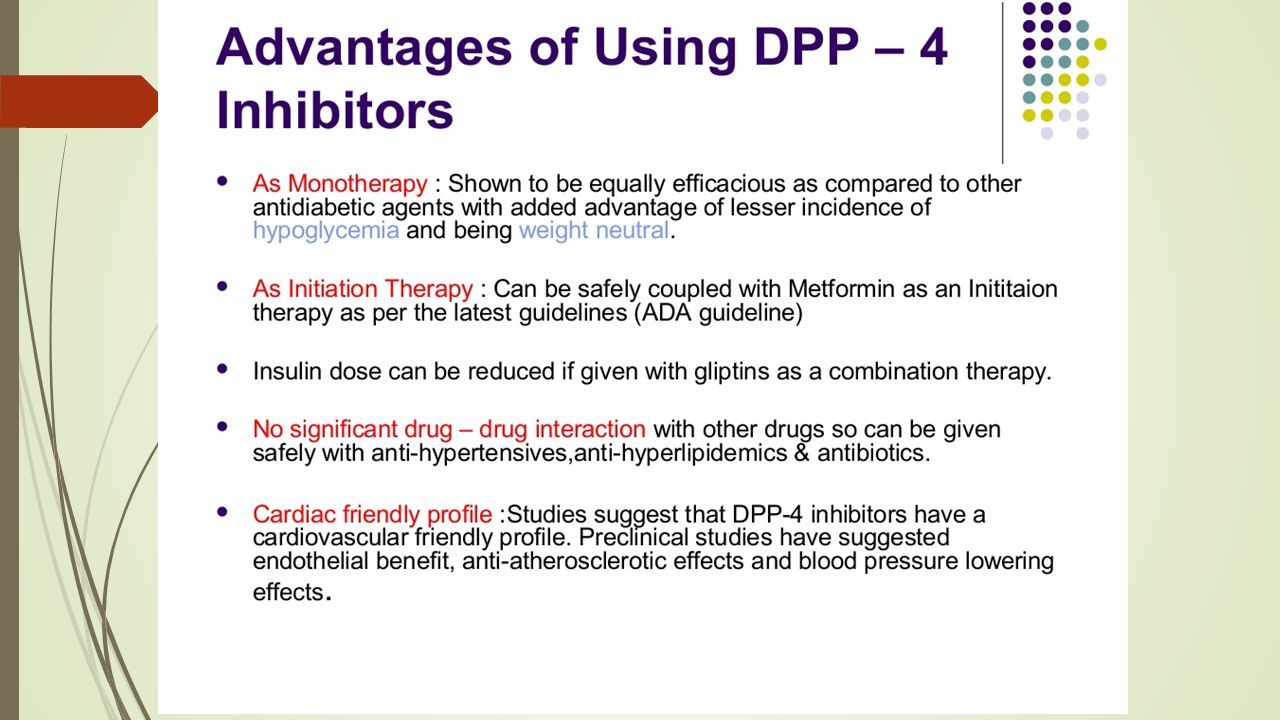
GLP-1-based therapies, including the dipeptidyl peptidase 4 (DPP-4) inhibitors, do not usually cause hypoglycemia unless combined with therapies that can cause hypoglycemia. DPP-4 inhibitors have a modest effect on GLP-1 levels, compared with giving GLP-1 agonists

55
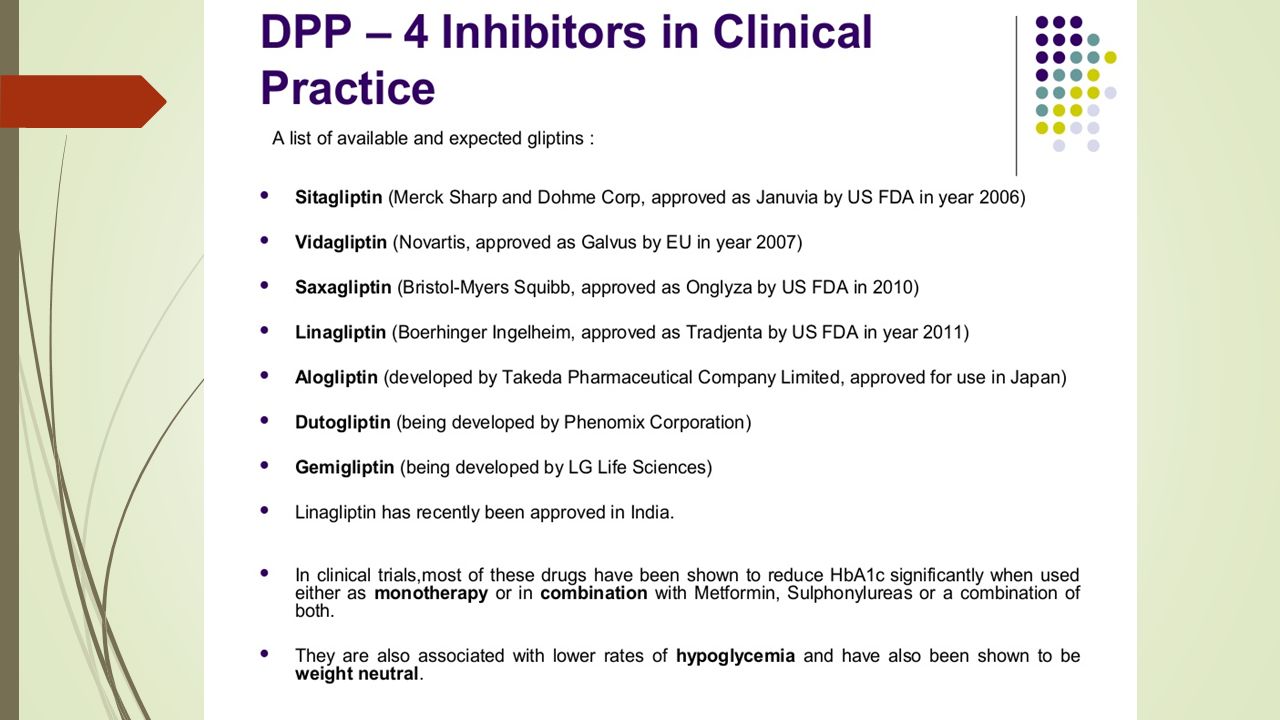
GLP-1 Short half-life ( 2 minutes) Rapidly degraded by dipeptidyl peptidase-IV (DPP-IV) DPP-IV inhibition Extends endogenous GLP-1 half-life Approved in US: Sitagliptin (Merck)
 Rapidly degraded by dipeptidyl peptidase-IV (DPP-IV) DPP-IV inhibition Extends endogenous GLP-1 half-life Approved in US: Sitagliptin (Merck)")
59
GLP-1 receptor agonists Mimic many of the glucoregulatory effects of GLP-1 Resistant to DPP-IV Approved in US: Exenatide Liraglutide

61
Renal Glucose Reabsorption in Type 2 Diabetes Sodium-glucose cotransporter 2 (SGLT2) plays a role in renal glucose reabsorption in proximal tubule Renal glucose reabsorption is increased in type 2 diabetes Selective inhibition of SGLT2 increases urinary glucose excretion, reducing blood glucose Wright EM, et al. J Intern Med. 2007;261:32-43.

62
Sglt2 i

63
SGLT2 I Canagliflozin is taken orally before the first meal of the day. The initial dose is 100 mg once daily, and it can be increased to 300 mg daily Canagliflozin Dapagliflozin (10 mg once daily) can be taken any time of day, with or without food. Dapagliflozin Empagliflozin is taken orally once daily in the morning, with or without food.The initial dose is 10 mg daily, and it can be increased to 25 mg once daily to achieve glycemic goals. Empagliflozin
 can be taken any time of day, with or without food. Dapagliflozin Empagliflozin is taken orally once daily in the morning, with or without food.The initial dose is 10 mg daily, and it can be increased to 25 mg once daily to achieve glycemic goals. Empagliflozin.")
64
Amylin: The Other β Cell Hormone

65
Pramlintide is a stable, soluble amylin analog that is administered by mealtime subcutaneous injection.Pramlintide It is available for use for both type 1 and insulin-treated type 2 diabetes. Pramlintide reproduces the actions of amylin and controls glucose without causing weight gain.

66
Pramlintide

67
HYPERTENSION/BLOOD PRESSURE CONTROL Screening and Diagnosis Blood pressure should be measured at every routine visit. Patients found to have elevated blood pressure should have blood pressure confirmed on a separate day.

68
Goals Systolic Targets People with diabetes and hypertension should be treated to a systolic blood pressure goal of less than140 mmHg. Lower systolic targets, such as <130 mmHg, may be appropriate for certain individuals with diabetes, younger patients, albuminuria, one or more additional atherosclerotic cardiovascular disease risk factors.

69
Diastolic Targets Individuals with diabetes should be treated to a diastolic blood pressure goal of<90 mmHg Lower diastolic targets, such as<80 mmHg, may be appropriate for certain individuals with diabetes

70
Treatment Patients with blood pressure >120/80 mmHg should be advised on lifestyle changes to reduce blood pressure. Patients with confirmed office-based blood pressure >140/90 mmHg should, in addition to lifestyle therapy, have prompt initiation and timely subsequent titration of pharmacological therapy to achieve blood pressure goals.

71
Pharmacological therapy for patients with diabetes and hypertension should comprise a regimen that includes either an ACE inhibitor or an angiotensin receptor blocker but not both.

72
Multiple-drug therapy (including a thiazide diuretic and ACE inhibitor/ angiotensin receptor blocker, at maximal doses) is generally required to achieve blood pressure targets.
 is generally required to achieve blood pressure targets.")
73
LIPID MANAGEMENT In adults, a screening lipid profile is reasonable At first diagnosis At the initial medical evaluation And/or at age 40 years and periodically

74
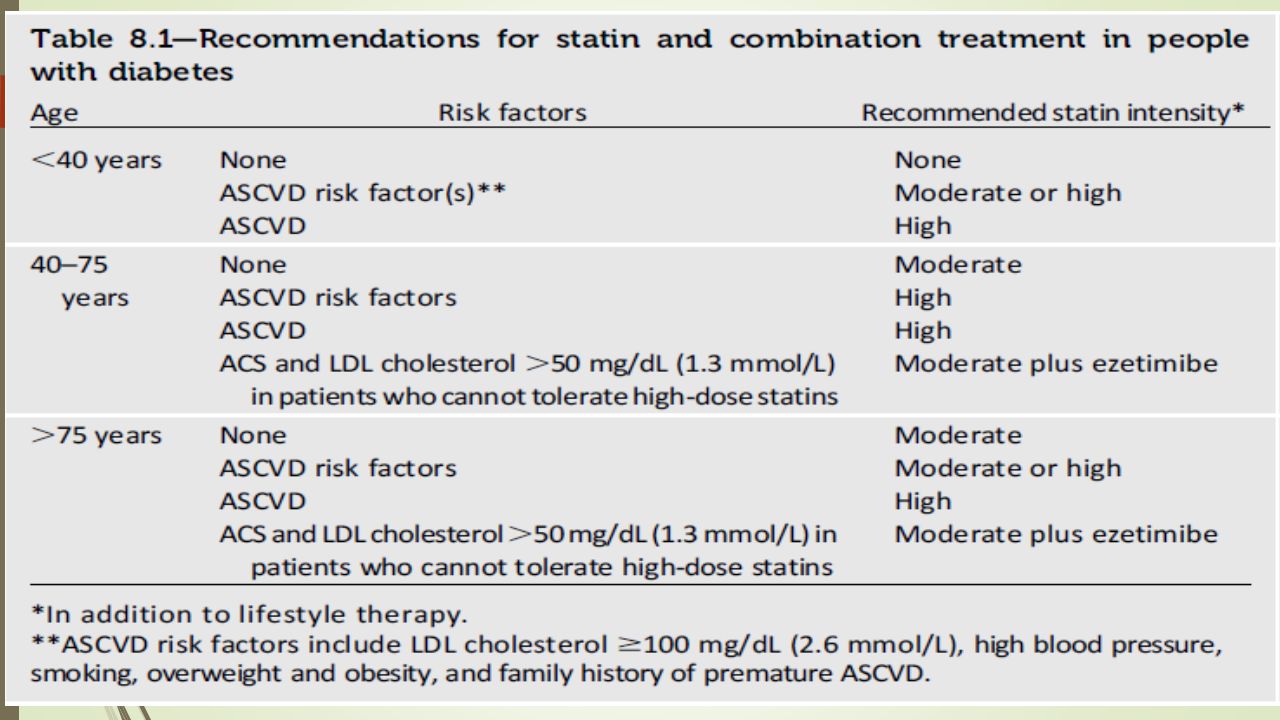
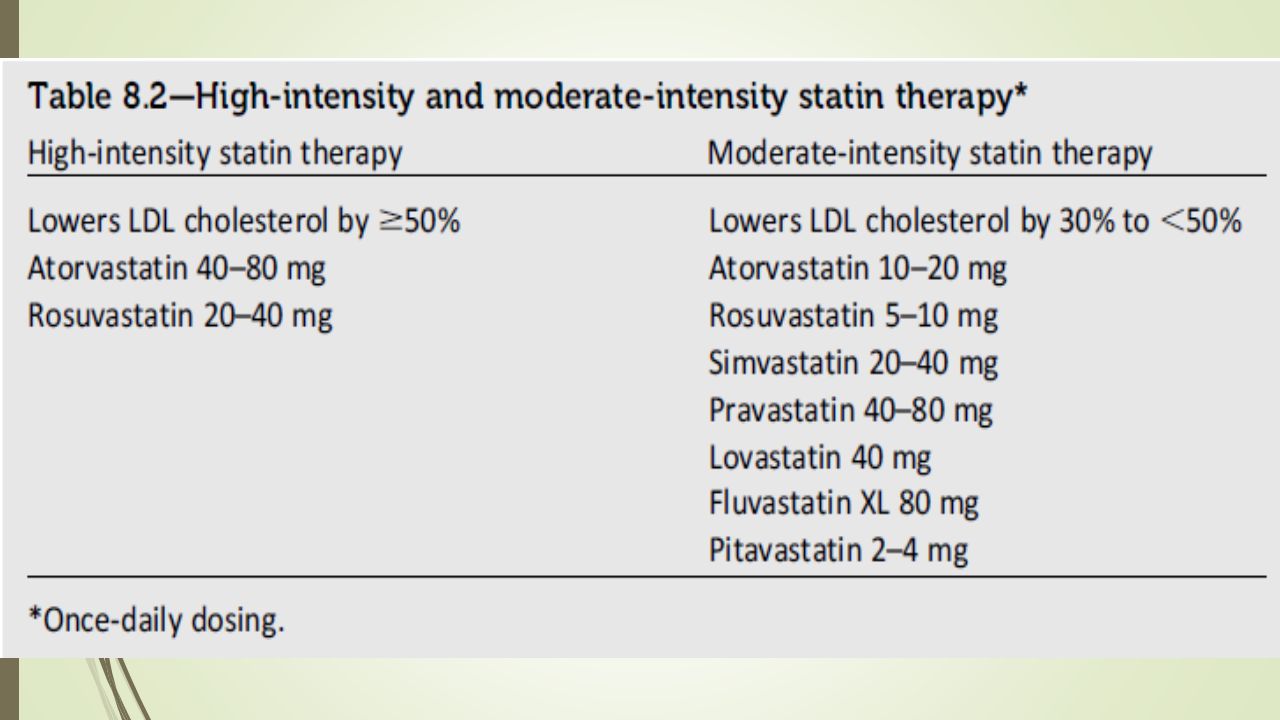
Treatment recommendations and goals Intensify lifestyle therapy and optimize glycemic control for patients with Triglyceride levels >150 mg/dL and/or HDL cholesterol >40 mg/dL in men and >50 mg/dL in women For patients with fasting triglyceride levels > 500 mg/dL, evaluate for secondary causes and consider medical therapy to reduce the risk of pancreatitis For patients of all ages with diabetes and atherosclerotic cardiovascular disease, high-intensity statin therapy should be added to lifestyle therapy.

77
Questions? 77

78
78

Similar presentations






 HbA1c – IFFC (mmol/mol) 6.042 6.548 7.053 7.559 8.064 9.075.>")

















 FPG (mg/dL) Postprandial glucose (mg/dL) ADA>")