Download presentation
Presentation is loading. Please wait.

1
PHARMACOLOGY OF ANTI-ANGINAL DRUGS (ID#580) Dr. Mariam Yousif Pharmacology & Toxicology Dept. November 17 th, 2014

2
References (Textbooks) Pharmacology (Rang et al. 7th ed.) Basic and Clinical Pharmacology (Katzung et al. 11th ed.) Integrated Pharmacology (Page et al. 3rd ed.)
 Basic and Clinical Pharmacology (Katzung et al. 11th ed.) Integrated Pharmacology (Page et al. 3rd ed.).")
3
WLO3834 Explain in summary form the pharmacology and mechanisms of anti-anginal management with an overview of the principles of their use, including adverse drug reactions.

4
Objectives 1. Define the rationale for the treatment of angina pectoris. 2. List the different classes of anti-anginal drugs. 3. Describe the mechanisms of action, uses and side effects of drugs used in the treatment of angina.

5
Definition Angina pectoris: Chest pain due to an inadequate supply of oxygen to the heart muscle. It is the clinical syndrome of transient cardiac ischaemia resulting from inadequate coronary blood flow.

6
characterized by severe chest pain or pressure that radiates to the left shoulder, left arm or to the back.

7
Pathophysiology Angina results when there is an imbalance between the heart's oxygen demand and supply. i.e. an increase in oxygen demand (e.g. during exercise) without a proportional increase in supply (e.g. obstruction or atherosclerosis of the coronary arteries).
 without a proportional increase in supply (e.g. obstruction or atherosclerosis of the coronary arteries)..")
8
Imbalance in myocardial oxygen supply- demand relationship results from spasm or obstruction of the coronary blood vessels occurs when the oxygen supply to the myocardium is not sufficient for its needs.

9
Types of Angina 1- Stable (Classic / Typical / Angina of Effort) 2- Unstable Angina 3- Variant (Prinzmetal's Angina)
 2- Unstable Angina 3- Variant (Prinzmetal s Angina)")
10
Stable Characterized by predictable pain on exertion. Occurs due to a fixed narrowing of the coronary arteries by atherosclerosis.

11
Unstable Angina Characterized by pain that occurs with less exertion, can occur at rest. Occurs due to disruption of an atherosclerotic plaque with subsequent cascade of platelet activation and aggregation, and thrombosis leading to a decrease in coronary blood flow.

12
Variant (Prinzmetal's Angina) Cardiac pain that occurs exclusively at rest. Caused by coronary artery vasospasm (vasospastic angina ) which reduces coronary flow leading to reduction of blood flow to the myocardium.
 which reduces coronary flow leading to reduction of blood flow to the myocardium..")
13
How to achieve the aim? A. Coronary vasodilators Increase blood flow to the myocardium by dilating the coronary arteries. B. Drugs that work load of the heart Decrease oxygen demand by reducing cardiac work.

14
# Nitrates # Beta-adrenergic blocking drugs # Calcium channel blockers Can be used alone or in combination Anti-Anginal Drugs

15
1. Organic Nitrates and Nitrites Nitroglycerin is the prototype drug Isosorbide dinitrate Amyl nitrite Nitrates are extremely important agents for the treatment of angina

16
Nitroglycerin concentrations are affected by the route of administration Preparations Sublingual, Tablet forms, Topical Peak concentrations Sublingual: 2-4 minutes Oral route: 15-30 minutes Transdermal route: 1-2 hours

17
-Nitroglycerin is rapidly inactivated by hepatic metabolism. Given sublingually to avoid the first pass effect and to achieve a therapeutic blood level rapidly. - Oral and transdermal products are acceptable for the long-term prophylaxis.

18
Mechanism of Action Organic nitrates nitric oxide (NO) [activates guanylyl cyclase] synthesis of cGMP vascular smooth muscle relaxation
![Mechanism of Action Organic nitrates nitric oxide (NO) [activates guanylyl cyclase] synthesis of cGMP vascular smooth muscle relaxation](http://images.slideplayer.com/42/11391662/slides/slide_18.jpg "Mechanism of Action Organic nitrates nitric oxide (NO) [activates guanylyl cyclase] synthesis of cGMP vascular smooth muscle relaxation")
19
Molecular and cellular mechanisms of action of nitrate and nitrite vasodilators. The product, phosphorylated protein kinase, leads to de- phosphorylation of myosin light chain and causes vascular smooth muscle relaxation.

20
PHARMACOLOGICAL ACTIONS -Relax vascular smooth muscle and cause vasodilation of blood vessels, both veins and arteries. -The effect on veins starts at lower doses, it is more pronounced than on the arteries.

21
Pharmacological Actions At low doses: venodilation (pooling of blood in veins) venous capacitance preload ( venous return) work on the heart oxygen consumption.
 venous capacitance preload ( venous return) work on the heart oxygen consumption.")
22
Pharmacological Actions At higher doses: Nitroglycerin dilates arterioles peripheral resistance after-load myocardial O 2 demand Blood pressure reflex tachycardia HR O2 consumption (combination therapy with blockers).
.")
23
# Nitroglycerin dilates the coronary arteries Blood supply to the heart muscle # Nitroglycerin diverts blood from normal to ischaemic areas of the myocardium through dilatation of collateral vessels (redistribution)
")
24
Development of Tolerance Continuous exposure to high doses of organic nitrates most of their pharmacological effects. The offset of tolerance is as rapid as its onset Therefore, one alternative dosing strategy to minimize tolerance is to provide a daily nitrate-free interval of 6-8 hours

25
Adverse Effects & Toxicity Postural hypotension Headache Reflex tachycardia

26
2. -Adrenergic Blocking Agents e. g. Propranolol, Atenolol, Metoprolol Predominant receptor subtype in the myocytes is 1 -receptor Blockade of 1 -receptors reduces the influence of endogenous catecholamines

27
Molecular mechanism of action of beta1-adrenoceptor antagonists. Stimulation of beta1-adrenoceptors by catecholamines leads to activation of adenylyl cyclase and an elevation of cAMP. This process is inhibited by beta1-adrenoceptor antagonists.

28
Negative chronotropic effect ( HR) and negative inotropic effect ( contractility), therefore reduce oxygen demand by the heart. # 1 selective blockers should be used to minimize bronchospasm in asthmatic patients. # Contraindicated in variant angina. 2. -Adrenergic Blocking Agents

29
3. Ca 2+ Channel Blockers Dihydropyridines: Nifedipine (smooth muscle selective) Non-dihydropyridines: Verapamil (cardioselective) Diltiazem (intermediate) Their main action is to interfere with the entry of calcium into the vascular smooth muscle cells and myocytes.
 Non-dihydropyridines: Verapamil (cardioselective) Diltiazem (intermediate) Their main action is to interfere with the entry of calcium into the vascular smooth muscle cells and myocytes..")
30
Vasodilator effect (nifedipine) on resistance vessels: after-load Coronary artery dilation coronary blood flow (variant angina) Calcium channel block in myocardium AV conduction and myocardial contractility Side effects: Constipation
 on resistance vessels: after-load Coronary artery dilation coronary blood flow (variant angina) Calcium channel block in myocardium AV conduction and myocardial contractility Side effects: Constipation")
31
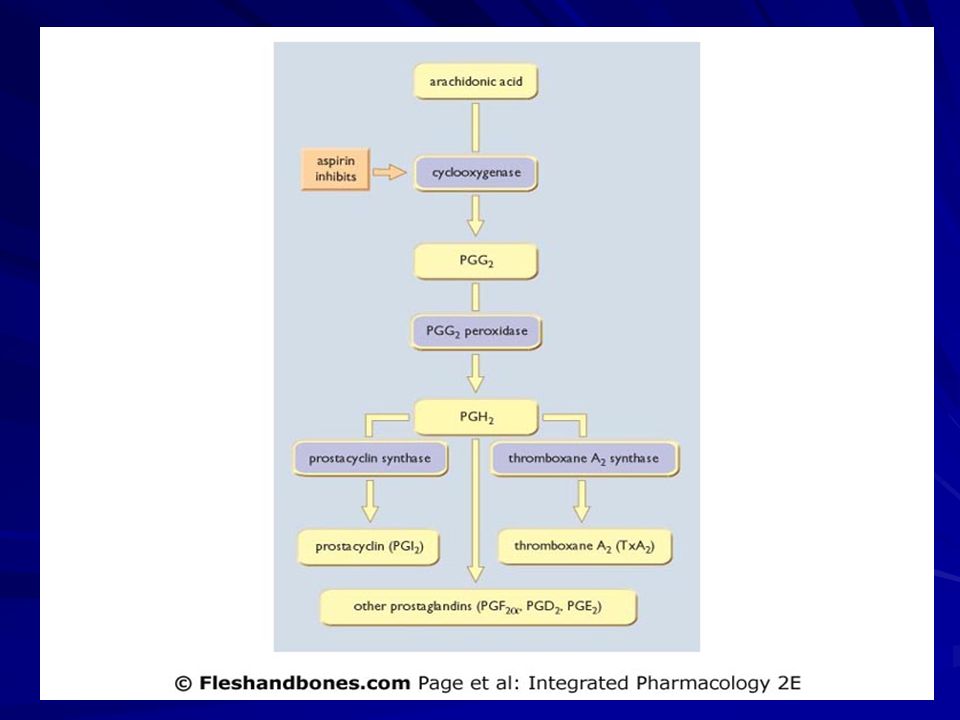
Antithrombotic Therapy In Unstable Angina -Platelet aggregation and thrombosis play a major role in unstable angina. -Both aspirin and heparin are extremely effective. -They reduce the occurrence of recurrent angina and the occurrence of MI or death. -Other antiplatelet agents available e.g clopidogrel.

33
Long term effect of aspirin is selective inhibition of thromboxane synthesis and therefore reduced platelet aggregation. This is achieved because platelets do not possess a cell nucleus and are therefore unable to resynthesize COX

34
Drug List (Anti-anginal Drugs) Nitroglycerin Propranolol, Atenolol, Verapamil, Nifedipine Aspirin, Heparin
 Nitroglycerin Propranolol, Atenolol, Verapamil, Nifedipine Aspirin, Heparin")
Similar presentations




 is the result of myocardial ischemia caused by an imbalance between myocardial blood supply and oxygen demand.>")








 CAD is most common form of heart disease and causes premature death. In UK, 1 in 3 men and.>")





