Download presentation
Presentation is loading. Please wait.

1
The importance of outcome measurement from a funding perspective A medical administrator’s view

2
Who am I Executive Director of Medical Services at Sir Charles Gairdner Hospital 530 Bed Tertiary Hospital, State Neurosciences Centre, State Cancer Centre, WA system

3
Pillars of hospital care Safety and Quality Finance and Budget Clinical Governance Patient outcomes and satisfaction Human resources

4
Demand > Funding in next 20 years

5
Projected health expenditure

6
Outcome measurement and funding Its about activity

7
The Australian Health System Policy role- public health, research, national information management Medicare Health research Residential aged care Commonwealth Public hospital services Community and public health services (some) State and Territories Hospital care Allied health/paramedical services 30% subsidy to individuals Private sector
 State and Territories Hospital care Allied health/paramedical services 30% subsidy to individuals Private sector")
8
Commonwealth contribution to funding for public hospitals

9
National Health Reform

10
National Health Reform April 2010 Majority funder of public hospital services- 60% of National efficient price, 60% of research and training. Funding primary health care- GP and over time 100% of national efficient price of ‘primary health care equivalent’ outpatient services to public hospitals. Initially 60% of public hospital outpatient services. Funding national aged care system Commonwealth Government Public hospital service planning, performance, purchasing of public hospital services from Local Hospital Networks, capital planning Supporting GP and primary health care policy State government

11
New national bodies National Health and Hospitals Network Funding Authority Independent Hospitals Pricing Authority

12
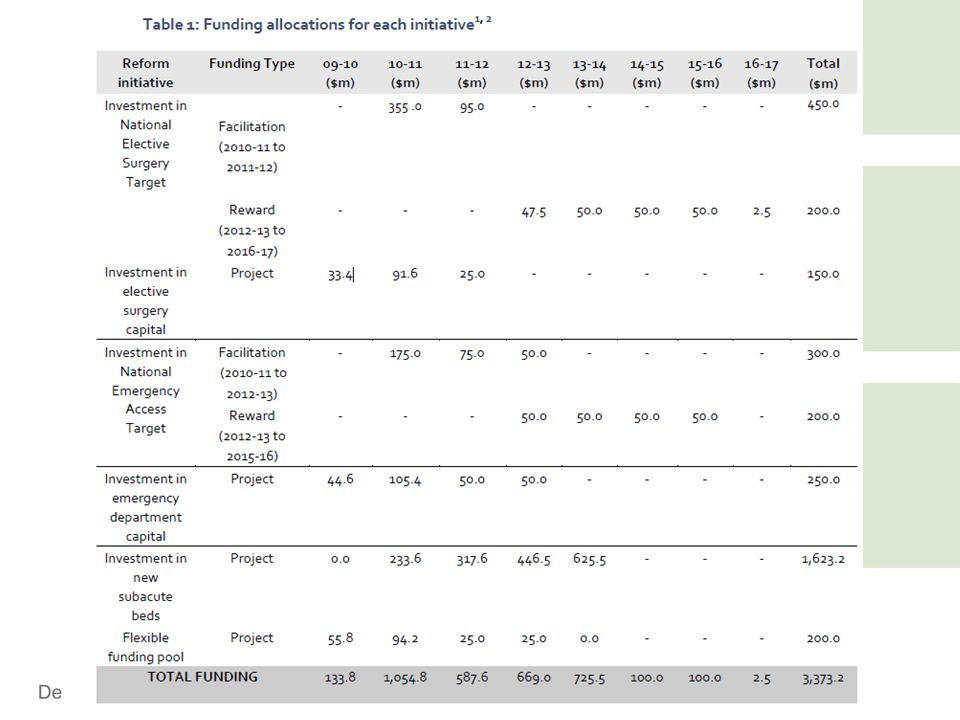
State funding

13
Activity based funding

14
Diagnostic Related Groups as a measure of activity for acute inpatients

15
What activities can’t currently be funded under activity based model? Teaching (eg, medical, nursing, allied health) Learning (eg, intern, resident and registrar medical training, student nurses) Research Services for boarders (eg, a mother staying at the hospital while her child is an inpatient) Patient travel (eg, isolated patient travel schemes) and medical retrieval services (eg, air ambulance) Support for affiliated agencies (eg, hospitals that prepare food for Meals on Wheels) Public health and health promotion services (eg, healthy lifestyle programs, parent education for new mothers) Interpreter services Aboriginal liaison and support.
 Learning (eg, intern, resident and registrar medical training, student nurses) Research Services for boarders (eg, a mother staying at the hospital while her child is an inpatient) Patient travel (eg, isolated patient travel schemes) and medical retrieval services (eg, air ambulance) Support for affiliated agencies (eg, hospitals that prepare food for Meals on Wheels) Public health and health promotion services (eg, healthy lifestyle programs, parent education for new mothers) Interpreter services Aboriginal liaison and support..")
16
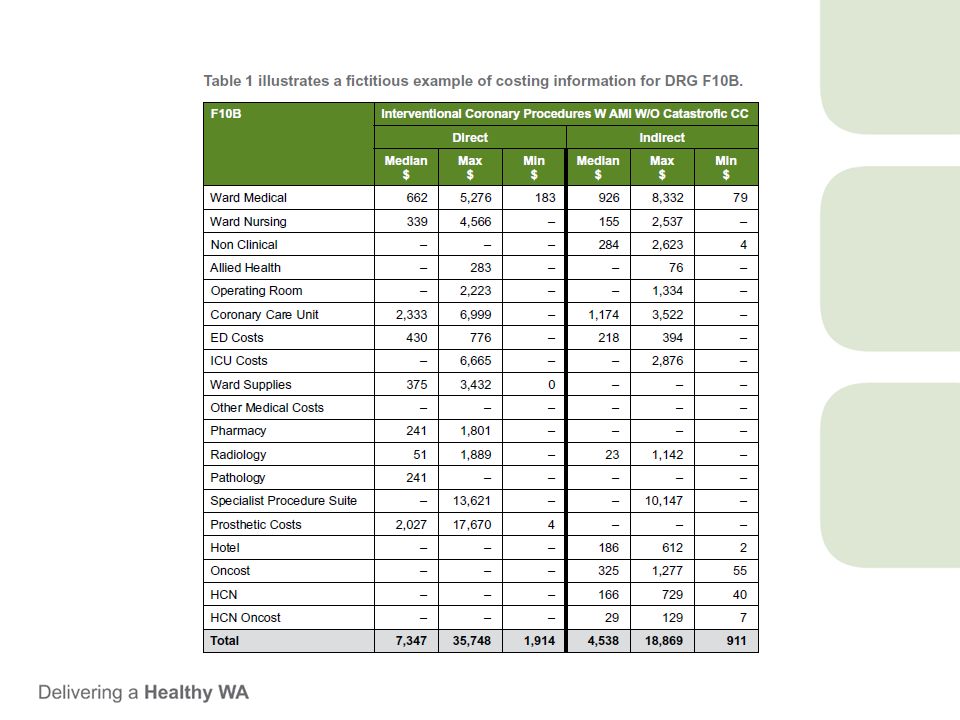
Casemix funding

17
Funds received for a knee replacement= iwau measure for a knee replacement * price per iwau

18
How do the states determine what is in casemix?

20
Hospital Revenue Total iauw= sum of projected activity (casemix) Total Hospital Funding= total iwau * price per iwau
 Total Hospital Funding= total iwau * price per iwau")
21
First, rewarding hospitals at full average cost for activity provides an incentive to increase activity as long as marginal cost is less than or equal to price/average cost; this could result in the provision of care that is financially unsustainable and/or medically inappropriate. Second, the association between prices and average cost encourages convergence to the mean, rather than incentivising improvement in performance. … Third, cost-based prices may not reflect the value of outputs and, therefore, may result in the production of a sub-optimal mix of outputs from a societal perspective (O’Reilly et al. forthcoming). Basing prices on average costs is
. Basing prices on average costs is.")
22
Independent Health Pricing Authority- outpatient funding

26
HOSPITALS AND OUTCOME MEASUREMENT

28
Key Performance indicators SQ3. Hospital standardised mortality ratio (HSMR) SQ4. Death in low-mortality Diagnosis Related Groups (DRGs) SQ5. In-hospital mortality rates for: acute myocardial infarction (AMI) heart failure stroke fractured neck of femur, and pneumonia SQ6. Unplanned hospital re-admissions of patients discharged following management of: AMI heart failure knee and hip replacements depression schizophrenia, and paediatric tonsillectomy and adenoidectomy SQ7. Healthcare associated Staphylococcus aureus (including MRSA) bacteraemia SQ8. Clostridium difficile infections ResultTarget Proportion of privately managed public patients discharged to home 98.79% (all persons) 98.86% Unplanned readmission rate for the same or related condition for privately managed public patients 0.5%2.3% Survival rates for sentinel conditions of privately managed public patients Stroke – 85.1% Acute Myocardial Infarction (AMI) – 98.1%; Fractured Neck of Femur (FNOF) – 95.6% Stroke ≥85.9% AMI ≥96.6%; FNOF ≥98.7% Average cost of public admitted patient treatment episodes in private hospitals $2,676 $2,675 Cost per capita of supporting treatment of patients in public hospitals $26.09 $26.43
 SQ5. In-hospital mortality rates for: acute myocardial infarction (AMI) heart failure stroke fractured neck of femur, and pneumonia SQ6. Unplanned hospital re-admissions of patients discharged following management of: AMI heart failure knee and hip replacements depression schizophrenia, and paediatric tonsillectomy and adenoidectomy SQ7. Healthcare associated Staphylococcus aureus (including MRSA) bacteraemia SQ8. Clostridium difficile infections ResultTarget Proportion of privately managed public patients discharged to home 98.79% (all persons) 98.86% Unplanned readmission rate for the same or related condition for privately managed public patients 0.5%2.3% Survival rates for sentinel conditions of privately managed public patients Stroke – 85.1% Acute Myocardial Infarction (AMI) – 98.1%; Fractured Neck of Femur (FNOF) – 95.6% Stroke ≥85.9% AMI ≥96.6%; FNOF ≥98.7% Average cost of public admitted patient treatment episodes in private hospitals $2,676 $2,675 Cost per capita of supporting treatment of patients in public hospitals $26.09 $")
30
Effect of these outcome measures Meet minimum targets Does not affect funding except that have to look at meeting minimum KPI Important in hospital accreditation Some targets come with incentive payments

31
Outcome measurement and funding Its about activity

32
The problem of measuring health outcome to determine funding of hospitals The effectiveness of a procedure depends on who gets it. The person, sociodemographics The effectiveness and costs of a procedure depend on where the procedure is performed and who does it Tertiary vs secondary centres etc

33
WHAT ARE THE CONSTRAINTS ON FUNDING AT A HOSPITAL LEVEL? That way we can understand what sort of outcomes administrators are looking at.

35
The problem of free healthcare

36
Implications Demand>supply leads to rationing Queues Activity caps under ABF funding Block funding- limited funding

37
Annual income twenty pounds, annual expenditure nineteen pounds nineteen and six, result happiness. Annual income twenty pounds, annual expenditure twenty pounds ought and six, result misery.” (Mr. Micawber, in David Copperfield by Charles Dickens – 1850)
.")
38
Hospital revenue= activity (capped) * price (externally set) Costs= activity (emergency and elective) * cost per activity
 * price (externally set) Costs= activity (emergency and elective) * cost per activity")
39
1. THE IMPORTANCE OF LENGTH OF STAY

40
Hospital costs breakdown Fixed costs Building- capital Utilities- cleaning, food, electricity, gases Nursing cost (NHPD) Medical cost Variable costs Prosthetics Drugs pathology
 Medical cost Variable costs Prosthetics Drugs pathology")
41
How to reduce cost per unit of activity Increasing volume without increasing fixed costs By decreasing LOS Maintaining volume and decreasing fixed costs (e.g. number of wards open) By decreasing LOS
 By decreasing LOS.")
43
2. Reduction in negative events that are not funded Some events are not funded. E.g. cost of falls and hip fractures, hospital acquired infections They are costs without revenue

44
Meet KPI’s and receive incentive payments NEAT and NEST Elective surgery targets 3. Increase revenue or avoid losing revenue

45
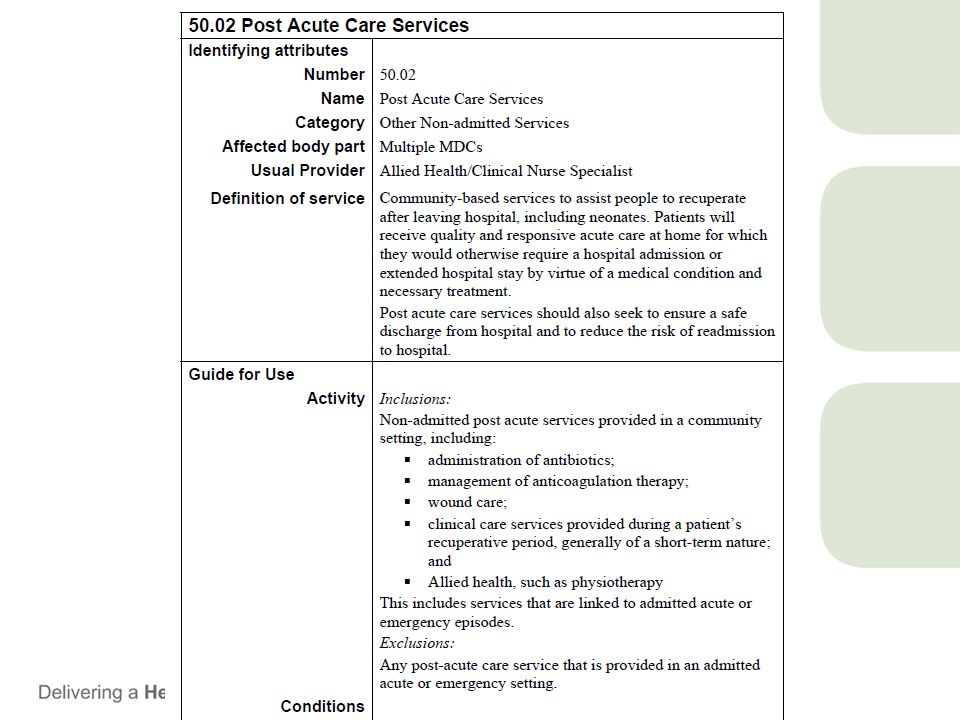
4. Alternatives to inpatient care Early discharge programs Hospital avoidance programs State governments will fund ambulatory care and (maybe) hospital avoidance programs
 hospital avoidance programs.")
46
Summary Cost control reduction in LOS Reduction in negative events which are unfunded Increase revenue and incentive payments Hospital avoidance/early discharge

47
WHAT DOES PAIN MEDICINE LOOK LIKE IN AN ABF MODEL

48
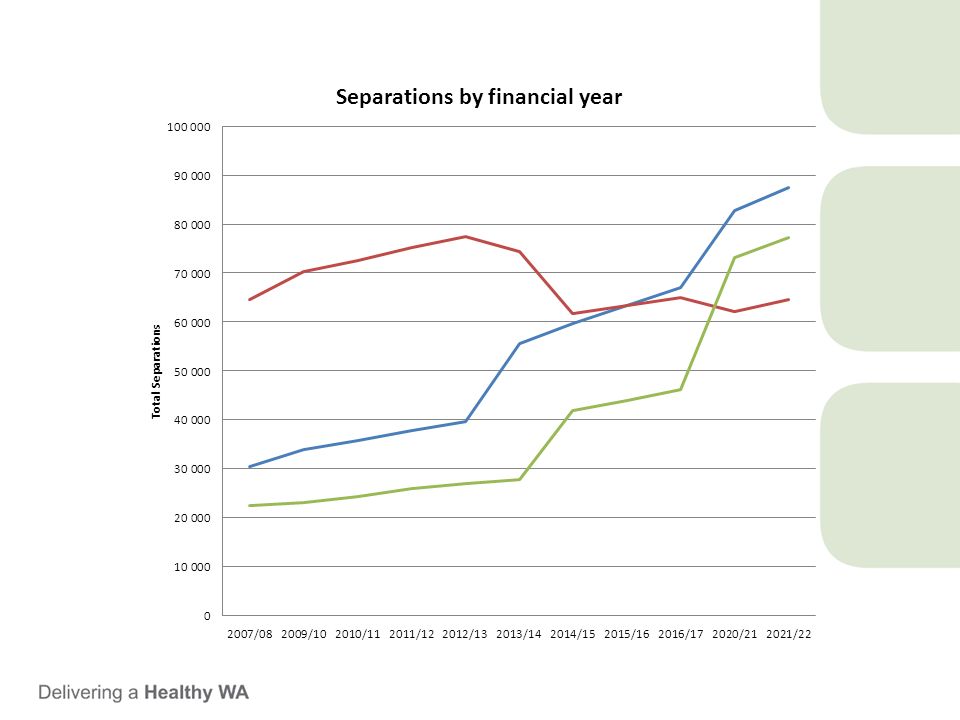
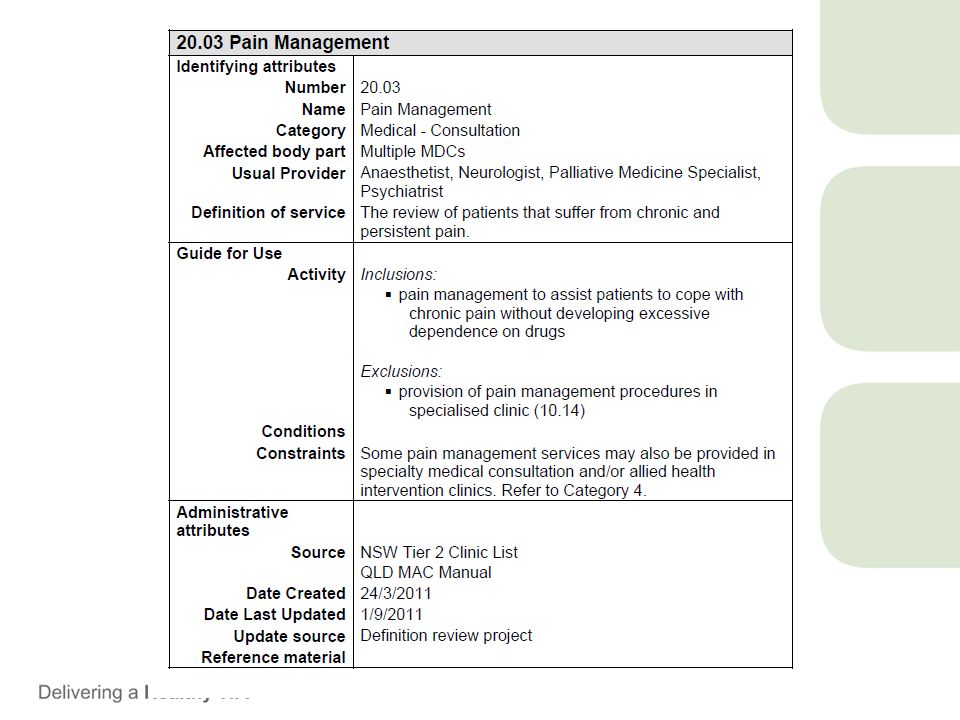
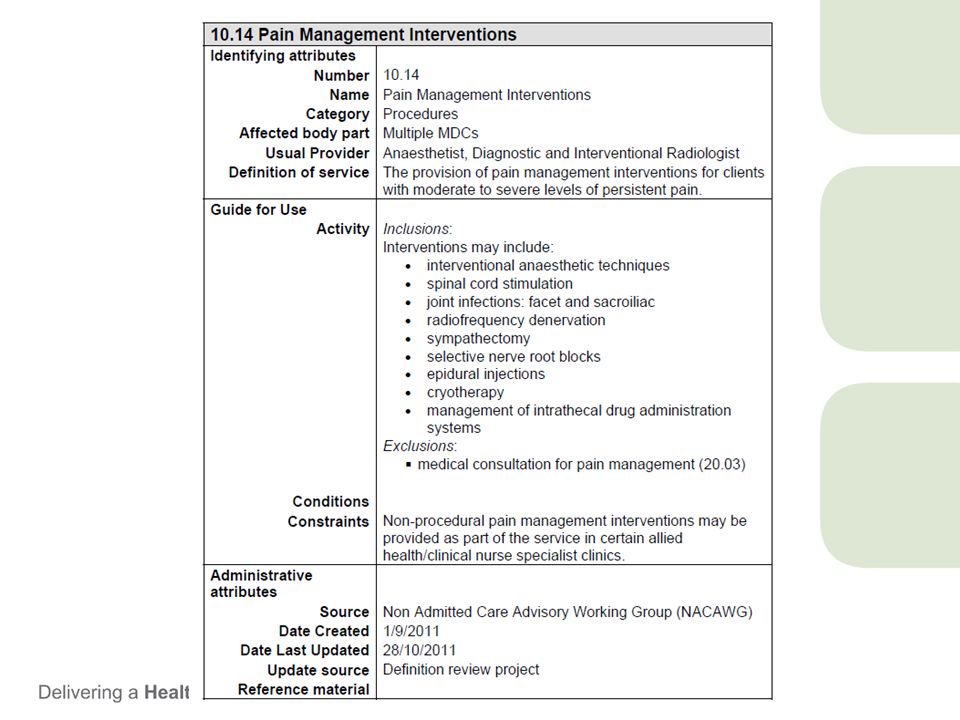
Pain medicine activity Inpatients- pain service Outpatients Individual outpatient clinic review Multidisciplinary intervention Interventional procedures

50
Costing of pain service Pain service consultation does not attract DRG code Therefore Pain service does not directly generate revenue It is a cost an can be considered to be a overhead

51
Justifications for funding Will have to justify outcomes But what sort of outcomes -hospital diversion -reduce LOS -reduce complications

52
Outpatient activity Need to ensure that costs are less than revenue Unlikely Therefore states will have to fund the difference. This will limit outpatient activity

53
Pain services much like any consultatation liaison service Disadvantaged under ABF funding. Does not attract revenue directly Contributes to costs.

54
Questions?

Similar presentations


 Independent Hospital Pricing Authority.>")






 1.5d: Controlling Medical Expenses.>")






 and Domain 5 (C18, C19)>")




