Download presentation
Presentation is loading. Please wait.

1
Wheezing and Asthma

2
Adventitious Airway Sounds Snoring Stridor Wheezing Crepitations

3
Acute Wheezing Asthma Bronchiolitis Foreign body

4
Bronchiolitis 4

5
What Is Bronchiolitis? Bronchiolitis is acute inflammation of the airways, characterised by wheeze Bronchiolitis can result from a viral infection Respiratory Syncytial Virus (RSV) may be responsible for up to 90% of bronchiolitis cases in young children Hall CB, McCarthy CA. In: Principles and Practice of Infectious Diseases 2000:1782-1801; Panitch HB et al. Clin Chest Med 1993;14:715-731 5
 may be responsible for up to 90% of bronchiolitis cases in young children Hall CB, McCarthy CA. In: Principles and Practice of Infectious Diseases 2000: ; Panitch HB et al. Clin Chest Med 1993;14:")
6
Common cause of illness in young children Common cause of hospitalization in young children Associated with chronic respiratory symptoms in adulthood May be associated with significant morbidity or mortality

7
Chronic Wheezing Thriving child – Happy wheezer Child failing to thrive – Causes?

8
DIAGNOSIS Acute infectious inflammation of the bronchioles resulting in wheezing and airways obstruction in children less than 2 years old

9
MICROBIOLOGY Typically caused by viruses – RSV-most common – Parainfluenza – Human Metapneumovirus – Influenza – Rhinovirus – Coronavirus – Human bocavirus Occasionally associated with Mycoplasma pneumonia infection

10
RSV Is a Common Virus Causing Bronchiolitis in Children In a clinical study in Argentina, RSV was the most common virus isolated from a sample of children aged <5 years with acute lower respiratory infection 0.7% 6.5% 6.8% 7.8% 78.2% RSV Adenovirus Parainfluenza Influenza A Influenza B Carballal G et al. J Med Virol 2001;64:167-174 10 New viruses (Human Metapneumovirus, Bocca, Corona)
.")
11
EPIDEMIOLOGY Typically less than 2 years with peak incidence 2 to 6 months May still cause disease up to 5 years Leading cause of hospitalizations in infants and young children Accounts for 60% of all lower respiratory tract illness in the first year of life

12
RISK FACTORS OF SEVERITY Prematurity Low birth weight Age less than 6-12 weeks Chronic pulmonary disease Hemodynamically significant cardiac disease Immunodeficiency Neurologic disease Anatomical defects of the airways

13
PATHOGENESIS Viruses penetrate terminal bronchiolar cells--directly damaging and inflaming Pathologic changes begin 18-24 hours after infection Bronchiolar cell necrosis, ciliary disruption, peribronchial lymphocytic infiltration Edema, excessive mucus, sloughed epithelium lead to airway obstruction and atelectasis

14
CLINICAL FEATURES Begin with upper respiratory tract symptoms: nasal congestion, rhinorrhea, mild cough, low- grade fever Progress in 3-6 days to rapid respirations, chest retractions, wheezing

15
EXAM Tachypnea – 80-100 in infants – 30-60 in older children Prolonged expiratory phase, rhonchi, wheezes and crackles throughout Possible dehydration Possible conjunctivitis or otitis media Possible cyanosis or apnea

16
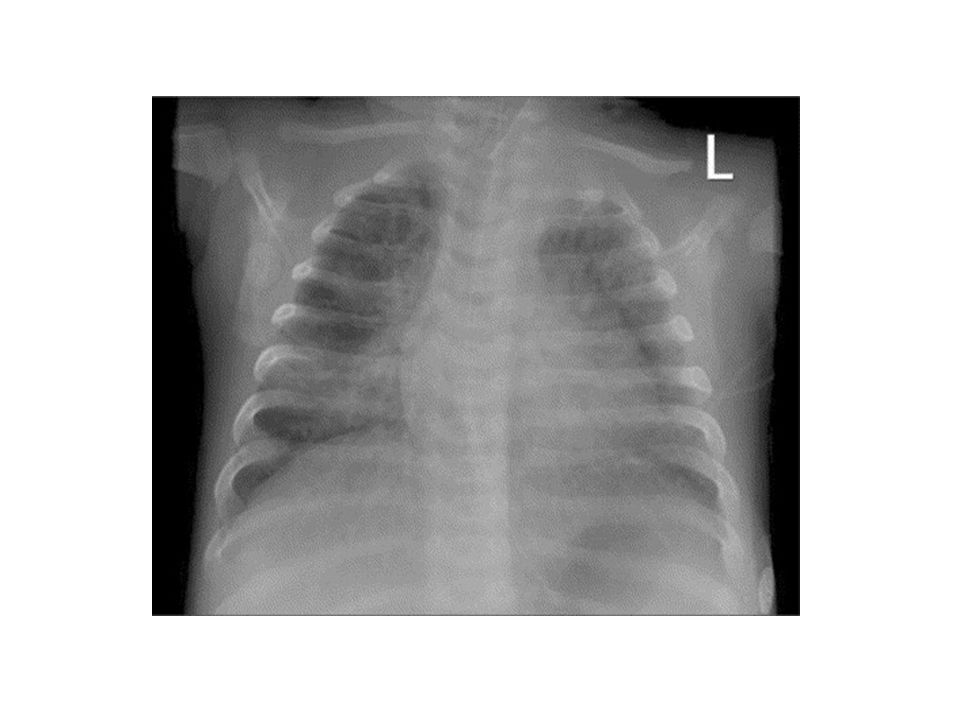
DIAGNOSIS Clinical diagnosis based on history and physical exam Supported by CXR: hyperinflation, flattened diaphragms, air bronchograms, peribronchial cuffing, patchy infiltrates, atelectasis

18
VIRAL IDENTIFICATION Generally not warranted in outpatients and rarely alters treatment or outcomes May decrease antibiotic use May help with isolation, prevention of transmission May help guide antiviral therapy

19
DIFFERENTIAL DIAGNOSIS Viral-triggered asthma Bronchitis or pneumonia Chronic lung disease Foreign body aspiration Gastroesophageal reflux or dysphagia leading to aspiration Congenital heart disease or heart failure Vascular rings, bronchomalacia, complete tracheal rings or other anatomical abnormalities

20
COURSE Depends on co-morbidities Usually self-limited Symptoms may last for weeks but generally back to baseline by 28 days In infants > 6 months, average hospitalization stays are 3-4 days, symptoms improve over 2-5 days but wheezing often persists for over a week Disruption in feeding and sleeping patterns may persist for 2-4 weeks

21
RISK FOR SEVERE DISEASE Toxic or ill-appearing Oxygen saturation < 95% on room air Age less than 3 months Respiratory rate > 70 Atelectasis on CXR

22
HOSPITALIZATION Children with severe disease Toxic with poor feeding, lethargy, dehydration Moderate to severe respiratory distress (RR > 70, dyspnea, cyanosis) Apnea Hypoxemia Parent unable to care for child at home
 Apnea Hypoxemia Parent unable to care for child at home")
23
TREATMENT Supportive care Pharmacologic therapy Ancillary evaluation

24
SUPPORTIVE CARE Respiratory support and maintenance of adequate fluid intake Saline nasal drops with nasal bulb suctioning Routine deep suctioning not recommended Antipyretics Rest

25
RESPIRATORY SUPPORT Oxygen to maintain saturations above 90-92% Keep saturations higher in the presence of fever, acidosis, hemoglobinopathies Wean carefully in children with heart disease, chronic lung disease, prematurity Mechanical ventilation for pCO2 > 55 or apnea

26
FLUID ADMINISTRATION IV fluid administration in face of dehydration due to increased need (fever and tachypnea) and decreased intake (tachypnea and respiratory distress) Monitor for fluid overload as ADH levels may be elevated
 and decreased intake (tachypnea and respiratory distress) Monitor for fluid overload as ADH levels may be elevated")
27
- Steroids whether inhaled or systemic : controversy? - Bronchodilators not usually recommended. - Antibiotics are not useful. - Ribavirin in those who at risk to develop severe disease. -

28
PREVENTION Good hand washing Avoidance of cigarette smoke Avoiding contact with individuals with viral illnesses Influenza vaccine for children > 6 months and household contacts of those children

30
Asthma

31
Chronic disease of the airways that may cause Wheezing Breathlessness Chest tightness Nighttime or early morning coughing Episodes are usually associated with widespread, but variable, airflow obstruction within the lung that is often reversible either spontaneously or with treatment. What is Asthma ? 319/29/2016

32
Allergens Infections Exercise Abrupt changes in the weather Exposure to airway irritants, such as tobacco smoke Potential Asthma Triggers 329/29/2016

33
Recurrent asthma episodes, involving – Shortness of breath – Coughing – Wheezing – Chest pain or tightness Range in severity from – Mild intermittent – Severe persistent Asthma Exacerbations 339/29/2016

34
Increases risk for early death Compromises child’s quality of life Affects family’s quality of life Increased costs associated with Increased utilization of health care Burden of Asthma 349/29/2016

35
Most common cause of school absence – An average of 9.7 days per year for asthma Most prevalent cause of childhood disability (long- term reduction in ability to do normal activities) In 1994-95, 1.4% of U.S. children experienced some disability due to asthma – This is 21% of all children with asthma Children with asthma have higher rates of social and emotional problems Asthma and Quality of Life 359/29/2016

36
Asthma is the most common chronic disease among children It has increased at epidemic rates since the early 1980s Most common cause of ED visits, hospitalization and missed school days In past 2 decades, African American children had 2-4 times more ED visits than other races Studies show a rise in worldwide prevalence Seems to be more prevalent in affluent nations Epidemiology of Asthma 369/29/2016

37
Etiology of asthma is due to the interaction of environmental and genetic factors – Atopy, the genetically inherited susceptibility to asthma, cannot account for epidemic. Probably NOT due to outdoor air quality Indoor air contaminants may be a factor – Tighter construction trapping contaminants. – Children spending more time indoors. What Accounts for this Epidemic? 379/29/2016

38
By gender – Males 0 – 17 years are more likely than girls to have asthma or experience an asthma attack By race/ethnicity – Higher for Black non-Hispanic children – Higher for Hispanic children Variability in Asthma Prevalence 389/29/2016

39
Parental Asthma Allergy Atopic dermatitis Allergic rhinitis Food allergy Inhalant allergen sensitization Food allergen sensitization Early Childhood Risk Factors 399/29/2016

40
Severe lower respiratory tract infections Wheezing apart from colds Male gender Low birth weight Tobacco smoke exposure Exposure to chlorinated swimming pools Possible use of Acetaminophen Contd. 409/29/2016

41
Common Viral infections Aeroallergens Animal dander Dust mite Cockroaches Molds Pollen Asthma Triggers 419/29/2016

42
Air pollutants Ozone Sulfur dioxide Particulate matter Dust Tobacco smoke Strong/ noxious fumes Cold, dry air Exercise Contd. 429/29/2016

43
Occupational exposures Farm and barn exposure Formaldehyde, paint fumes Crying, laughter, hyperventilation Co morbid conditions: Rhinitis, Sinusitis Contd. 439/29/2016

44
Symptoms: Intermittent dry cough Expiratory wheezing Shortness of breath Chest tightness Chest pain Fatigue Difficulty keeping up with peers in physical activities Clinical Manifestations 449/29/2016

45
Signs: Expiratory wheezing Prolonged expiratory phase Decreased breath sounds Crackles/ rales Accessory muscle use Nasal flaring Absence of wheezing in severe cases Pulses paradoxus Contd. 459/29/2016

46
Spirometry: Feasible in children >6 years of age Monitoring Asthma and efficacy of treatment Measures FVC, FEV 1 and FEV1/FVC Ratio Normal values for children available on the basis of height, gender and ethnicity. Lab Findings 469/29/2016

47
Airflow Limitation: Low FEV1 FEV1/ FVC ratio < 0.80 Bronchodilator response to β-agonist: Improvement in FEV1 ≥ 12% Exercise challenge: Worsening of FEV1 ≥ 15% Daily peak flow or FEV1 AM-PM variation ≥ 20% Contd. 479/29/2016

48
Often normal Hyperinflation Helpful in identifying masqueraders Radiology: 489/29/2016

49
Treatment 499/29/2016

50
509/29/2016

51
519/29/2016

52
Managing Asthma: Asthma Management Goals Achieve and maintain control of symptoms Maintain normal activity levels, including exercise Maintain pulmonary function as close to normal levels as possible Prevent asthma exacerbations Avoid adverse effects from asthma medications Prevent asthma mortality 529/29/2016

53
Managing Asthma: Indications of a Severe Attack Breathless at rest Hunched forward Speaks in words rather than complete sentences Agitated Peak flow rate less than 60% of normal 539/29/2016

54
Managing Asthma: Things People with Asthma Can Do Have an individual management plan containing – Your medications (controller and quick-relief) – Your asthma triggers – What to do when you are having an asthma attack Educate yourself and others about – Asthma Action Plans – Environmental interventions Seek help from asthma resources Join an asthma support group 549/29/2016
 – Your asthma triggers – What to do when you are having an asthma attack Educate yourself and others about – Asthma Action Plans – Environmental interventions Seek help from asthma resources Join an asthma support group 549/29/2016")
55
Asthma action plan for management of exacerbation Regular follow up visits Monitor lung functions annually Improve adherence to treatment Contd. 559/29/2016

56
Eliminate/ reduce environmental exposures Tobacco smoke elimination/ reduction Allergen exposure elimination/ reduction Treat co morbid conditions: Rhinitis, Sinusitis, GER Control of Factors Contributing to Severity 569/29/2016

57
Initiate with higher level controller therapy Step-down, once good control is achieved If child has had well controlled asthma for at least 3 months, consider decreasing dose or number of controller medications. Step up for poorly controlled asthma Step-up, Step-down Approach 579/29/2016

58
All persistent Asthmatics require daily controller medications Long Term Controller Medications 589/29/2016

59
Treatment of choice for persistent Asthma Improve lung function Reduce use of rescue medicines Reduce ED visits, hospitalizations May lower the risk of death due to Asthma Inhaled Corticosteroids 599/29/2016

60
Used mainly in treatment of exacerbations Rarely in patients with severe disease Common: Prednisolone, Prednisone, Methyprednisolone When used in long term, cause adverse effects Systemic Corticosteroids 609/29/2016

61
Salmeterol, Formoterol Not used as monotherapy Major role as ad-on agents with ICS LABA use should be stopped once optimal Asthma control is achieved Long Acting β-Agonists 619/29/2016

62
Leukotriene synthesis inhibitor: Zileuton (Not approved for children < 12 years) Leukotriene Receptor Antagonists: Montelukast, Zafirlukast Leukotriene Modifying Agents 629/29/2016
 Leukotriene Receptor Antagonists: Montelukast, Zafirlukast Leukotriene Modifying Agents 629/29/2016")
63
Cromolyn, Nedocromil Inhibit exercise induced bronchospasm Can be used in combination of SABA for exercise induced bronchospasm Non-steroidal Anti- inflammatory Agents 639/29/2016

64
Can reduce Asthma symptoms and need for SABA use Narrow therapeutic window Not used as first line anymore May be used in corticostroid dependent children Can cause cardiac arrhythmias, seizures and death Theophyllin 649/29/2016

65
Anti IgE monoclonal antibody Blocks IgE mediated allergic response Approved for children > 12 years with moderate to severe Asthma Given sub cutaneously every 2-4 weeks Omalizumab 659/29/2016

66
Short Acting Beta Agonists: Albuterol, Levalbuterol, Terbutaline, Pirbuterol Drugs of choice for acute Asthma symptoms Overuse may be associated with increased risk of death Use of at least 1 MDI/ month or at least 3 MDI/ year indicates inadequate Asthma control Anticholinergic Agents: Ipratropium bromide Used in combination with Albuterol Rescue Drugs 669/29/2016

67
Dyspnea at rest Peak flows < 40% of personal best Accessory muscle use Failure to respond to initial treatment -What is status asthmaticus? -What is silent chest? Acute Exacerbations 679/29/2016

68
Brief assessment Administration of SABA: Repeated doses or continuously, every 20 mins. for 1 hour Inhaled anticholinergic in addition of SABA Oxygen: Hypoxemia/ moderate to severe exacerbation Systemic Corticosteroids: Instituted early for moderate to severe exacerbation and failure to respond to early treatment Intramuscular beta agonist in severe cases. Management of Acute Exacerbation 689/29/2016

Similar presentations



>")

















