Download presentation
Presentation is loading. Please wait.

1
Obesity in Gynecologic Oncology: A Growing Epidemic Paola A. Gehrig, MD Professor and Chief Division of Gynecologic Oncology University of North Carolina Chapel Hill, NC

2
Objectives To review the impact of obesity To discuss the pharmacotherapy options for the treatment of the obese woman To review obesity’s impact on cancer To review some very exciting research in obesity as it relates to gynecologic malignancies

3
Objectives To review the impact of obesity To discuss the pharmacotherapy options for the treatment of the obese woman To review obesity’s impact on cancer To review some very exciting research in obesity as it relates to gynecologic malignancies

4
Disclosures I have nothing to disclose.

5
25 years in the US CDC.gov

6
Link between obesity and income ObesityIncome

7
Putting BMI in context DescriptionClassBMI5’4”5’4”5’10” Normal18.5-24.9110-145135-175 Overweight25.0-29.9146-175176-210 ObesityI30.0-34.9176-205211-245 ObesityII35-39.9 Extreme Obesity III>40235+280+

8
Globesity -250 million people (7%) are obese -2-3 times this are overweight -Across the globe, more people are overweight than malnourished -15% of men and 22% of women in Europe are obese
 are obese -2-3 times this are overweight -Across the globe, more people are overweight than malnourished -15% of men and 22% of women in Europe are obese")
10
BMI Awareness is poor Patient? –22.2% of obese women and 6.7% of obese men correctly classified themselves as obese 1 Provider? –Majority overweight/obese women deny being counseled about weight, weight loss 2 –Knowledge? Comfort? Time? –Study ongoing of health care providers’ ability to correctly recognize BMI 1.Truesdale KP, NC Med J, 2008 2.Evans et al, ASRM, 2010

11
Obesity in the United States Increasing steadily in the United States –One of the top 2 causes of preventable mortality 2/3 of adults are overweight 1/3 are obese (BMI >30) or morbidly obese (BMI >40) Obesity increases other co-morbidities –HTN, Diabetes, Cancer-endometrial $190 billion/year
 or morbidly obese (BMI >40) Obesity increases other co-morbidities –HTN, Diabetes, Cancer-endometrial $190 billion/year")
12
The future: 2030 ? Without intervention, the obesity epidemic escalates: –50% US men –165 million US adults –Health care spending increases $66 billion/yr -Gortmaker et al, Lancet 2011 - Bloomberg News, 8/26/2011

13
What about our kids? Newsweek, 2000

15
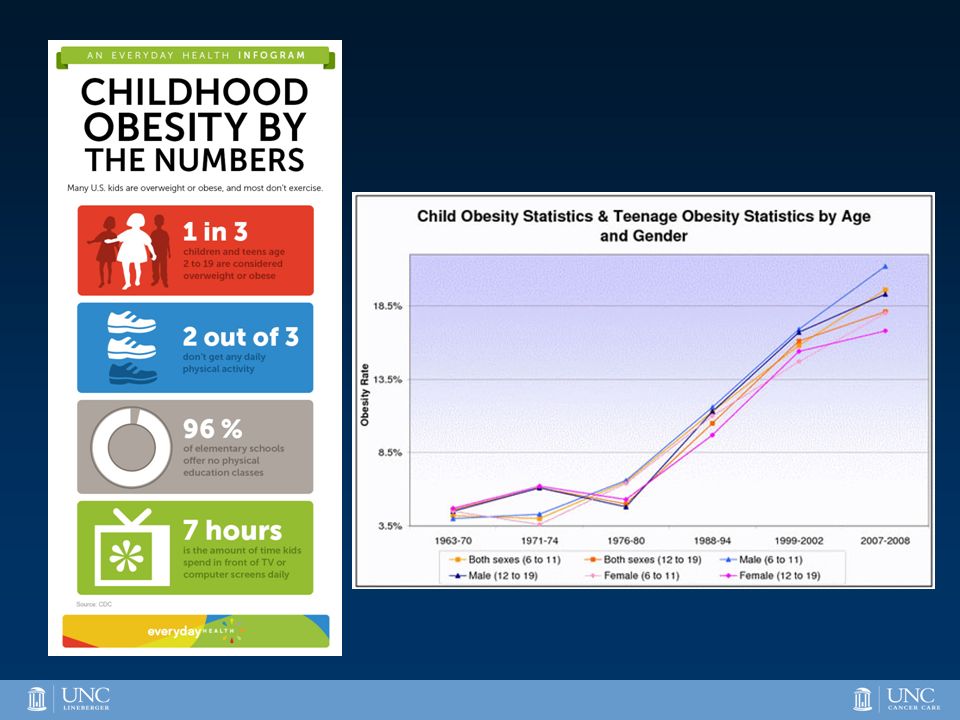
Childhood obesity: 2015 21% of US children >1/3 are overweight or obese Tripled from one generation ago (1980) Life expectancies projected to decline for the first time in a thousand years CDC.gov
 Life expectancies projected to decline for the first time in a thousand years CDC.gov")
16
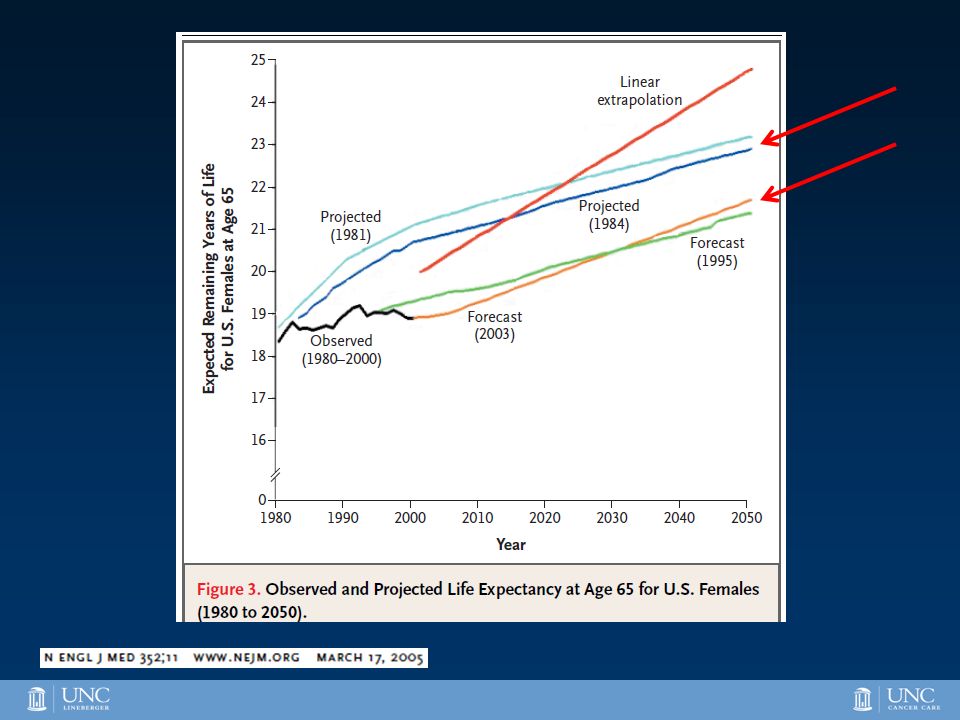
NEJM, March 2005

19
BMI and Mortality 115,000+ Nurses Health Study –Ages 30-55 in 1976 –16 yr follow up –Cancer free Mortality is lowest for BMI 19-26.9 1-3 1. De Gonzalez et al, NEJM 2010 2. Prospective Studies Collaboration, Lancet 2009 3. Manson et al, NEJM 1995 Manson et al, NEJM 1995

20
Weight Loss & Mortality Lowest mortality with BMI 19-27 Weight loss ≥ 20lbs reduces mortality by 25% 1 Manson et al, NEJM 1995 1. Williamson et al, Am J Epi 1995; 141: 1128-41.

21
Good news from The Lancet Gortmaker et al, Lancet 2011

22
Causes of Obesity

23
Objectives To review the impact of obesity To discuss the pharmacotherapy options for the treatment of the obese woman To review obesity’s impact on cancer To review some very exciting research in obesity as it relates to gynecologic malignancies

28
Why is this? Obesity is not only about calories in and calories out Genetic component to obesity? –“heritability of body fatness 1 ” is polygenetic Environmental exposures? Early infant feeding? Socioeconomic status? 1 FM Biro, M Wien. Am J Clin Nutr 2010;91(suppl):1499S-1505S.
:1499S-1505S..")
29
Can we stage Obesity?

30
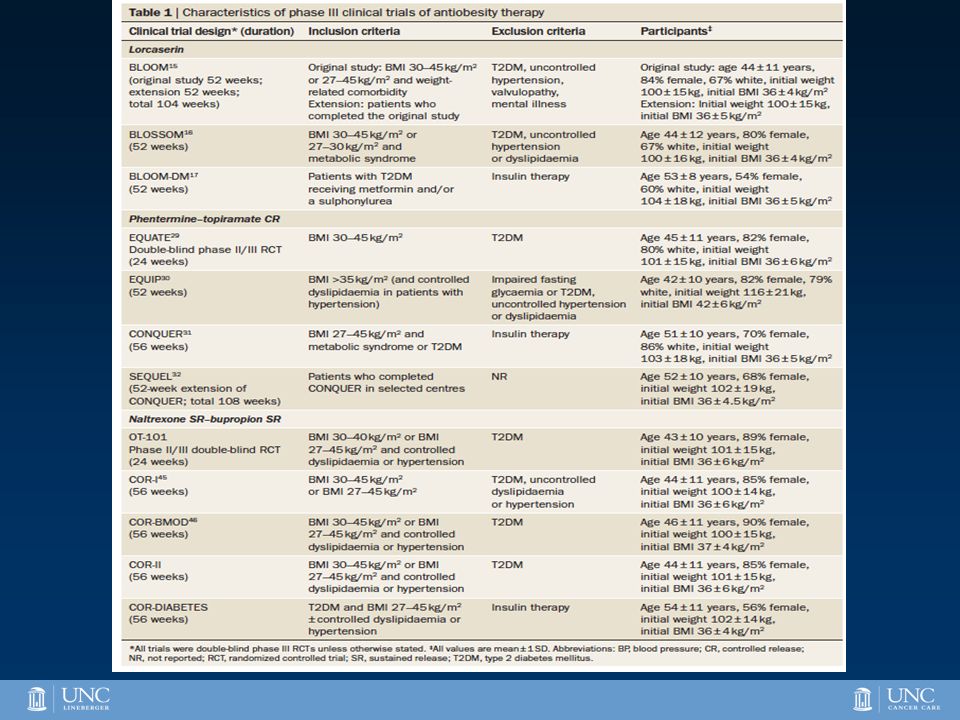
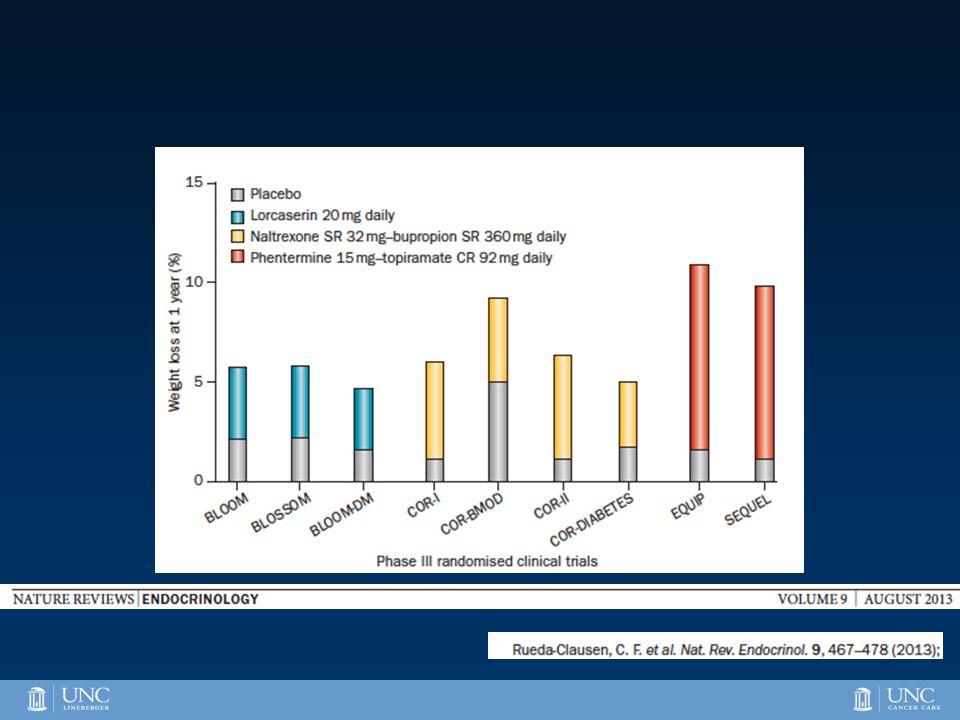
FDA-Approved Drugs for the Treatment of Obesity -Phentermine-Sympathomimetic action releases catecholamine from hypothalamus -Topiramate-anticonvulsant whose anti-obesity effects are incompletely understood -Lorcaserin-selective 5-HT2C agonist which decreases appetite through stimulation of melanocortin receptor 4 (MC4-R) by releasing melanotropin-α (α-MSH) -Bupropion SR-Decreased energy intake and increased thermogenesis via secretion of α-MSH and activation MC4-R; increased β-endorphins -Naltrexone-opioid receptor antagonist; reduces β-endorphin induced pleasure associated with eating food
 by releasing melanotropin-α (α-MSH) -Bupropion SR-Decreased energy intake and increased thermogenesis via secretion of α-MSH and activation MC4-R; increased β-endorphins -Naltrexone-opioid receptor antagonist; reduces β-endorphin induced pleasure associated with eating food")
34
Objectives To review the impact of obesity To discuss the pharmacotherapy options for the treatment of the obese woman To review obesity’s impact on cancer To review some very exciting research in obesity as it relates to gynecologic malignancies

36
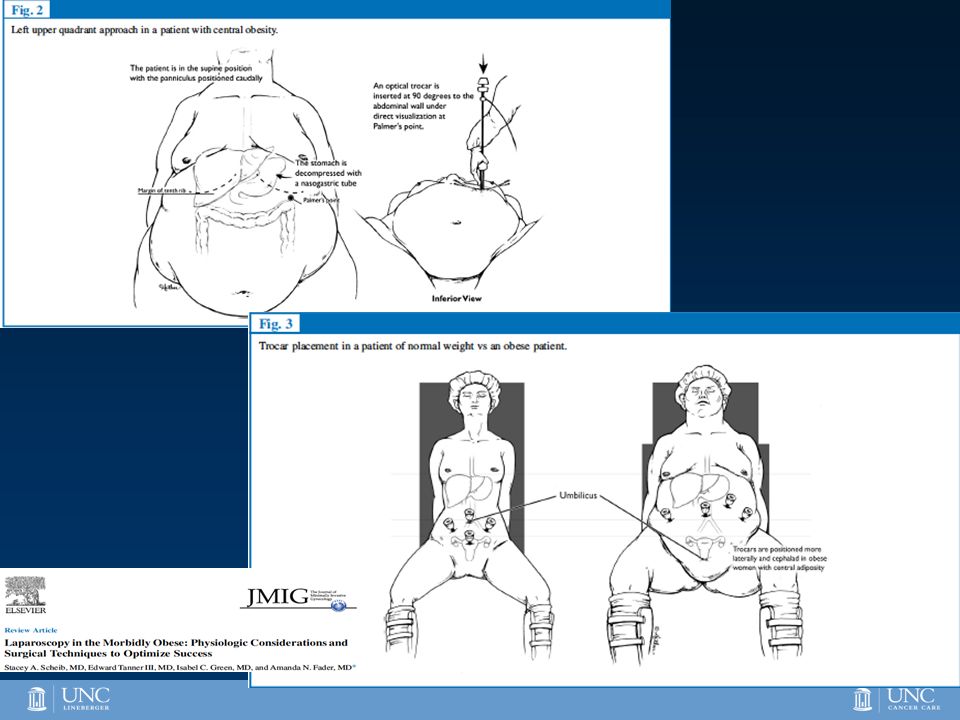
Gynecologic surgery in the Obese Patient Increased intra- and post-operative complications Increased length of hospital stay Longer OR times MIS may be the preferred modality in the obese woman McMahon MD. J Minim Invasive Gynecol. 2013 Sep 4 O’Hanlan KA. Gynecol Oncol, 2006; 103:938-41 Camanni M. J Min Inv Gynecol, 2010; 17:576-82 Gehrig PA. Gynecol Oncol. 2008 Oct;111(1):41-5.
:")
37
Waisbren et al. Percent body fat and prediction of surgical site infection.J Am Coll Surg 2010;210:381-9.

38
Disadvantages of Minimally Invasive versus Open Procedures -Higher operating costs? Probably not 1 -Longer operative time? -Learning curve (? Steeper for conventional L/S as compared to robotic assisted L/S) -Need for pneumoperitoneum -Hernias at port sites? -Seeding of malignant tissue at port sites? Probably not 2 1 Barnett J. Gynecol Oncol 2010:116:685-93. 2 Martinez A. Gynecol Oncol 2010;118:145-50.
 -Need for pneumoperitoneum -Hernias at port sites. -Seeding of malignant tissue at port sites. Probably not 2 1 Barnett J. Gynecol Oncol 2010:116: Martinez A. Gynecol Oncol 2010;118:")
39
Anesthesia Concerns Steep trendelenberg With robotics, patient position cannot be rapidly changed after docking. Paralytic Use “anti-skid” measures to decrease nerve injury Run patient dry Pressure control ventilation –Minimize peak airway pressures –Control CO2 by improving ventilation/perfusion ratios –Increase alveolar recruitment Cooperation from the entire OR team

42
Predicted probability curve for risk of conversion by body mass index (BMI), age, and metastatic disease. Walker J L et al. JCO 2009;27:5331-5336 ©2009 by American Society of Clinical Oncology

44
Literature Review 2.Eltabbakh GH,et al. Hysterectomy for obese women with endometrial cancer: laparoscopy or laparotomy? Gynecol Oncol 2000;78:329-335. 3.Scribner DR, et al. Pelvic and paraaortic lymph node dissection in the obese. Gynecol Oncol 2002;84:426-30. 4.Eisenhauer EL, et al. Comparing surgical outcomes in obese women undergoing laparotomy, laparoscopy, or laparotomy with panniculectomy for the staging of uterine malignancy. Ann Surg Oncol 2007;14:2384-91. 5. Gehrig, et al. What is the optimal minimally invasive surgical procedure for endometrial cancer staging in the obese and morbidly obese woman? Gynecol Oncol 2008;111:41-5. 6. Seamon et al. Comprehensive surgical staging for endometrial cancer in obese patients. Obstet Gynecol 2009;114:16-21.

45
Literature Review 2.Eltabbakh GH,et al. Hysterectomy for obese women with endometrial cancer: laparoscopy or laparotomy? Gynecol Oncol 2000;78:329-335. 3.Scribner DR, et al. Pelvic and paraaortic lymph node dissection in the obese. Gynecol Oncol 2002;84:426-30. 4.Eisenhauer EL, et al. Comparing surgical outcomes in obese women undergoing laparotomy, laparoscopy, or laparotomy with panniculectomy for the staging of uterine malignancy. Ann Surg Oncol 2007;14:2384-91. 5. Gehrig, et al. What is the optimal minimally invasive surgical procedure for endometrial cancer staging in the obese and morbidly obese woman? Gynecol Oncol 2008;111:41-5. 6. Seamon et al. Comprehensive surgical staging for endometrial cancer in obese patients. Obstet Gynecol 2009;114:16-21.

46
© 2009 The American College of Obstetricians and Gynecologists. Published by Lippincott Williams & Wilkins, Inc. 3 Comprehensive Surgical Staging for Endometrial Cancer in Obese Patients: Comparing Robotics and Laparotomy. Seamon, Leigh; Bryant, Shannon; Rheaume, Patrick; Kimball, Kristopher; Huh, Warner; Fowler, Jeffrey; Phillips, Gary; Cohn, David Obstetrics & Gynecology. 114(1):16-21, July 2009. DOI: 10.1097/AOG.0b013e3181aa96c7
:16-21, July DOI: /AOG.0b013e3181aa96c7.")
47
© 2009 The American College of Obstetricians and Gynecologists. Published by Lippincott Williams & Wilkins, Inc. 5 Comprehensive Surgical Staging for Endometrial Cancer in Obese Patients: Comparing Robotics and Laparotomy. Seamon, Leigh; Bryant, Shannon; Rheaume, Patrick; Kimball, Kristopher; Huh, Warner; Fowler, Jeffrey; Phillips, Gary; Cohn, David Obstetrics & Gynecology. 114(1):16-21, July 2009. DOI: 10.1097/AOG.0b013e3181aa96c7
:16-21, July DOI: /AOG.0b013e3181aa96c7.")
48
2015 US Cancer Cases* *Excludes basal and squamous cell skin cancers and in situ carcinomas except urinary bladder. Source: American Cancer Society, 2014. Men 848,200 Women 810,170 231,840Breast 105,590 Lung & bronchus 63,160 Colon & rectum 54,870 Uterine corpus 32,000 Non-Hodgkin lymphoma 48,340 Thyroid 31,200 Melanoma of skin 23,290Kidney & renal pelvis 21,290 Ovary 23,370 Leukemia ~22%All Other Sites Prostate220,800 Lung & bronchus115,610 Colon & rectum69,090 Urinary bladder56,320 Melanoma of skin42,670 Non-Hodgkin 39,850 lymphoma Kidney & renal pelvis38,270 Oral cavity32,670 Leukemia 30,900 Pancreas24,840 All Other Sites~20%

49
9/28/2016 49 Obesity and GYN Cancers UNC ovarian cancer patients –33% are obese/morbidly obese –58% are overweight/obese/morbidly obese UNC Endometrial cancer patients –62% are obese/morbidly obese –84% are overweight/obese/morbidly

50
RR of death: BMI 30-34 ->2.53 BMI >40 -> 6.25

51
Obesity and Cancer

53
Risk Factors for Endometrial Cancer ◦ Obesity (relative risk of 2–11) ▪ Relative risk of 3.0 in women 21–50 lb overweight and 10 in women more than 50 lb overweight ◦ Nulliparity (relative risk of 2–3) ◦ Late menopause, i.e., occurring in women older than 52 years (relative risk of 2.4) ◦ Exogenous unopposed estrogen (relative risk of 1.6–12) ◦ Tamoxifen (relative risk of 1.7–2.5) ◦ Diabetes (relative risk of 1.3–2.7) ◦ Hypertension (relative risk of 1.2–2.1) ◦ High dietary fat consumption (relative risk of 1.1–2.0) ◦ Radiation therapy (relative risk of 8) ◦ Hereditary Non-polyposis Colorectal Cancer (HNPCC; 39– 60% lifetime risk of EC)
 ▪ Relative risk of 3.0 in women 21–50 lb overweight and 10 in women more than 50 lb overweight ◦ Nulliparity (relative risk of 2–3) ◦ Late menopause, i.e., occurring in women older than 52 years (relative risk of 2.4) ◦ Exogenous unopposed estrogen (relative risk of 1.6–12) ◦ Tamoxifen (relative risk of 1.7–2.5) ◦ Diabetes (relative risk of 1.3–2.7) ◦ Hypertension (relative risk of 1.2–2.1) ◦ High dietary fat consumption (relative risk of 1.1–2.0) ◦ Radiation therapy (relative risk of 8) ◦ Hereditary Non-polyposis Colorectal Cancer (HNPCC; 39– 60% lifetime risk of EC)")
54
- Approximately 60% of endometrial cancer incidence is attributable to obesity and obese women diagnosed with endometrial cancer have six-times the risk of dying of non-obese women… -25% of endometrial cancer cases are in pre- or peri-menopausal women. -50% of women are unaware of the association between being overweight or gaining weight and endometrial cancer.

55
For each 5 kg/m2 increase in BMI, there is an increased risk of development of endometrial cancer (relative risk 1.59) Lancet 2008;371:569
 Lancet 2008;371:569")
56
Adult BMI gain and endometrial cancer risk 50,376 women in the Multiethnic Cohort Study 10.3 year of f/u with 463 endometrial cancer cases Women who were heavier at age 21 had increased risk of endometrial cancer BMI gain >35% had a RR of 4.12 compared to no BMI gain group (even if BMI <25) Women with annual BMI gain >1%/year had a 3.21 RR as compared to women with stable BMI AA and white women showed increase risk at a BMI gain >35%, however, Asian women showed an increased risk with >5% gain Park et al. Int J Cancer 2010;126:490-9.

61
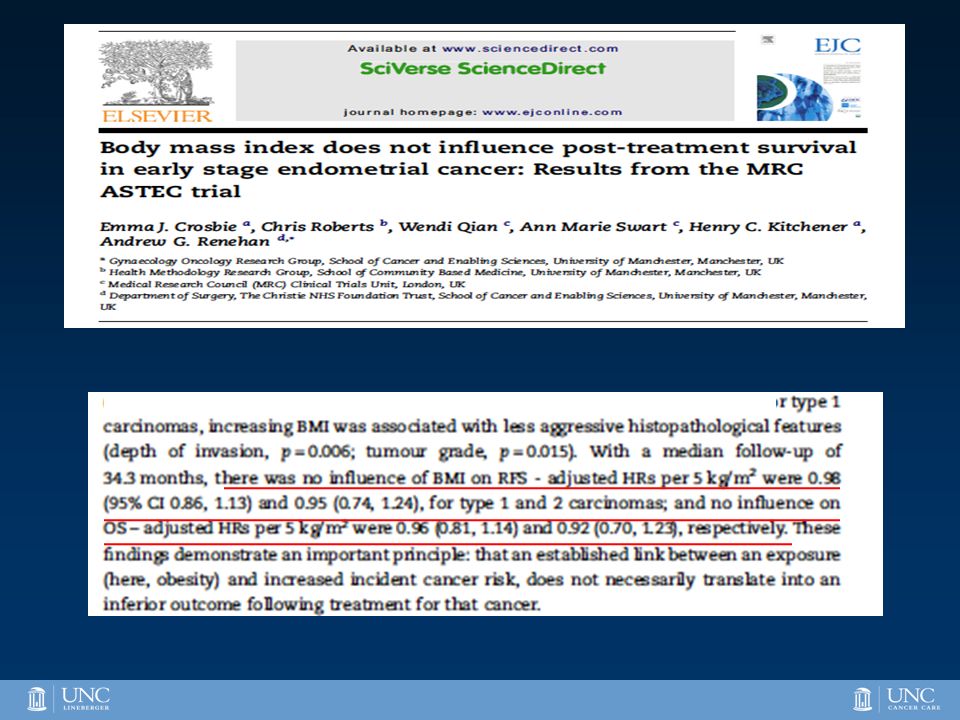
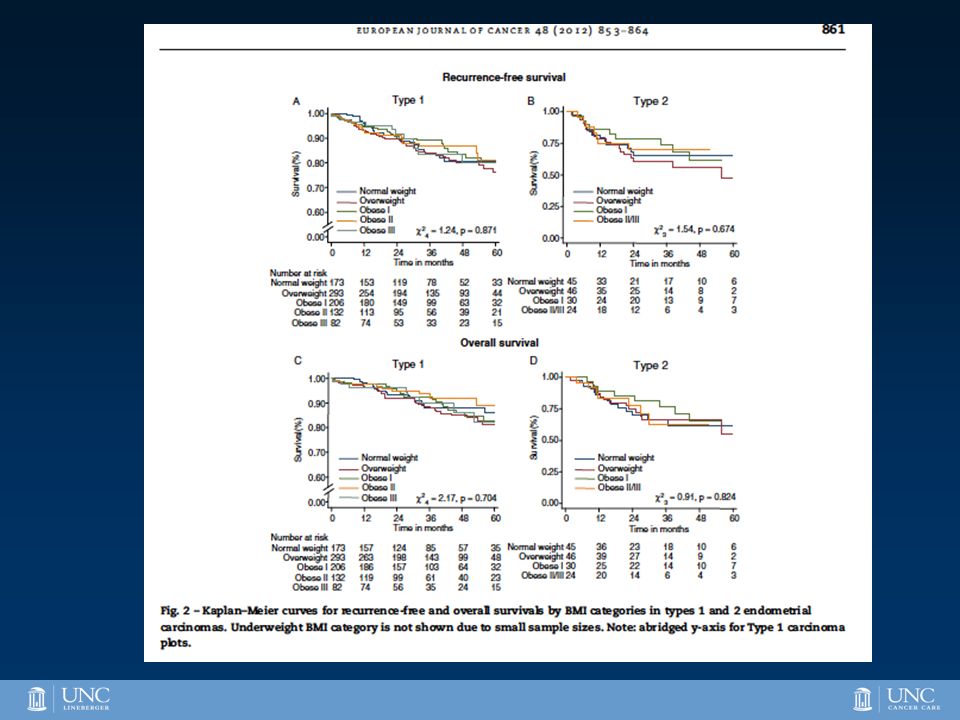
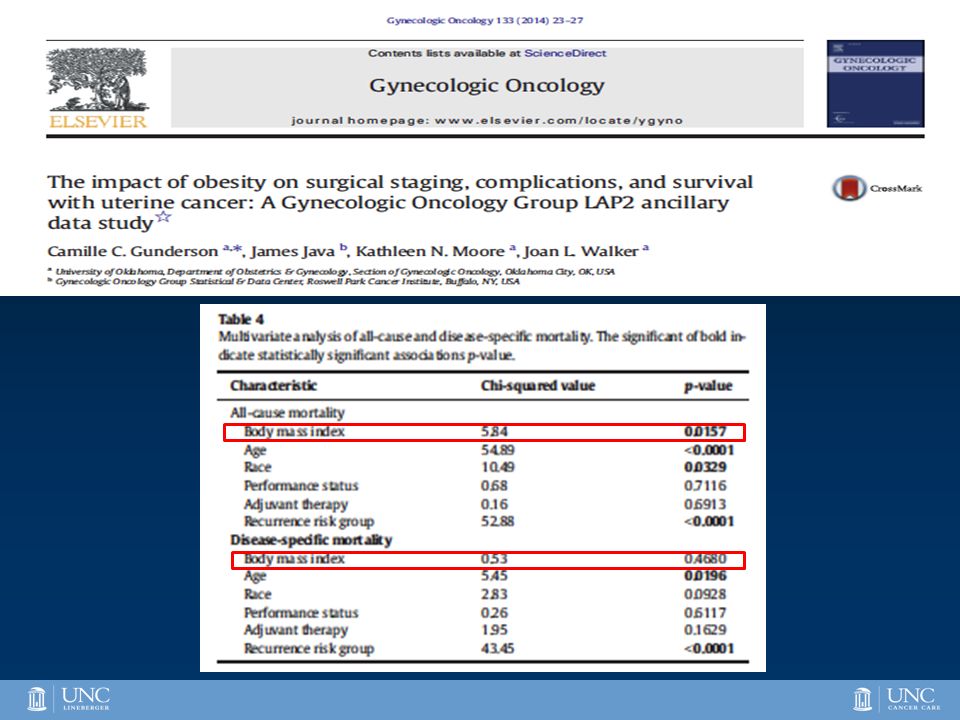
So the jury is still out but increasing evidence does not suggest that BMI impacts DSS in women with EC but all cause may be worse.

62
Increased BMI is also associated with an increased risk of ovarian cancer (odds ratio 1.3) 30% of women with ovarian cancer are overweight and 12% are obese -? Negative prognostic factor -? Inflammation -? Inadequate surgery -? Inadequate chemotherapy dosing SCOTROC -BMI not associated with PFS, OS, tumor stage, grade, debulking status… Jury still out Olsen CM, Eur. J. Cancer 2007;43:690

63
Effect of Obesity on Survival in Epithelial Ovarian Cancer OS for obese patients was 62 months vs. a median of 80 months for ideal body weight patients, P =.30. Pavelka JC et al. Effect of Obesity on Survival in Epithelial Ovarian Cancer. Cancer 2006;107:1520-4. N=216

64
Survival for Women with Stage III-IV Epithelial Ovarian Cancer Pavelka JC et al. Cancer 2006;107:1520-4. P=0.02

65
Obesity and Ovarian Cancer in KpB Mice K18-gT 121 +/- ; p53 fl/fl ; Brca1 fl/fl (KpB) –Deletion of BRCA1 and p53 –Inactivation of retinoblastoma proteins –Invasive cancer develops over 6 months –High Fat versus Low Fat Diet
 –Deletion of BRCA1 and p53 –Inactivation of retinoblastoma proteins –Invasive cancer develops over 6 months –High Fat versus Low Fat Diet")
66
Obesity and Tumor Size

67
Genomic Differences in Ovarian Tumors from Obese vs Lean Mice 131 up- or down-regulated genes –Lipid metabolism –Fatty acid metabolism –Metabolic signaling pathways (AMPK) LeanObese
 LeanObese")
68
What about in Humans? 12,042 genes in high grade serous ovarian cancer samples Gene Expression Linear regression modeling Covariates: –Age, race, stage, grade, residual tumor –BMI status Normal weight: BMI <25 Overweight and obese: BMI ≥25

69
Demographics BMI < 25 Normal Weight (N=99) BMI ≥ 25 Overweight/Obese (N=138) Age (mean)57.959.4 Race White Black Other 89 (90%) 5 (5%) 125 (91%) 11 (8%) 2 (1%) Grade 2 3 11 (11%) 88 (89%) 12 (9%) 126 (91%) Stage I/II III/IV 2 (2%) 97 (98%) 4 (3%) 134 (97%) Residual Disease Optimal Suboptimal 75 (76%) 24 (24%) 99 (72%) 39 (28%)
 BMI ≥ 25 Overweight/Obese (N=138) Age (mean) Race White Black Other 89 (90%) 5 (5%) 125 (91%) 11 (8%) 2 (1%) Grade (11%) 88 (89%) 12 (9%) 126 (91%) Stage I/II III/IV 2 (2%) 97 (98%) 4 (3%) 134 (97%) Residual Disease Optimal Suboptimal 75 (76%) 24 (24%) 99 (72%) 39 (28%)")
70
Genomic Differences in Ovarian Tumors Related to BMI 347 up- or down-regulated genes (q-value <0.1) –Lipid metabolism –Fatty acid metabolism –Metabolic signaling pathways (AMPK) –Ras pathway Cross-species comparison - AMPK on both gene lists.
 –Lipid metabolism –Fatty acid metabolism –Metabolic signaling pathways (AMPK) –Ras pathway Cross-species comparison - AMPK on both gene lists.")
71
Metformin’s Anti-Tumorigenic Effects Indirect – improvement in insulin resistance, decrease in circulating insulin and glucose levels Direct – inhibits mitochondrial complex 1, AMPK activation, leading to inhibition of the PI3K/Akt/mTOR pathway

72
Metformin and Ovarian Cancer Cell Lines Inhibits ovarian cancer cell growth. Induces ovarian cancer cell death. Inhibits targets of the mTOR pathway. Behaves synergistically with paclitaxel and platinums.

73
Metformin Inhibits Tumor Growth Lean Obese p=0.0003

74
Metformin in KpB Mice Induced obesity through HFD Induced ovarian cancer through adenovirus injection Treated for 4 weeks with: –Placebo –Metformin 200 mg/kg/day PO Tumors were evaluated for: –Size –Immunohistochemistry –Metabolomics

75
Ki67 ObeseObese+Met Lean Lean+Met Caspase 3 P-AMPK P-S6 Immunohistochemistry

76
Open Clinical Trials of Metformin in Ovarian Cancer 9/28/2016 76 CenterTitleTrial typeTumor typesStudy interventions University of Chicago NCT02122185 Metformin Hydrochloride and Combination Chemotherapy in Treating Patients With Stage III- IV Ovarian, Fallopian Tube, or Primary Peritoneal Cancer Randomized, placebo controlled, phase II trial Ovarian /Fallopian tube/Primary peritoneal Patients receive metformin BID or placebo BID in combination with standard chemotherapy for 6 courses. University of Michigan Cancer Center NCT01579812 A Phase II Evaluation of Metformin, Targeting Cancer Stem Cells for the Prevention of Relapse in Patients With Stage IIC/III/IV Ovarian, Fallopian Tube, and Primary Peritoneal Cancer Open label, efficacy trialOvarian/ Fallopian tube/ Primary Peritoneal (1) Patients receiving primary surgical debulking followed by standard chemotherapy will initiate metformin prior to primary surgery. (2) Patients treated with neoadjuvant chemotherapy will be initiated on metformin prior to the initiation of chemotherapy. Fox Chase Cancer Center NCT02050009 The Use and Safety of Metformin, Carboplatin and Paclitaxel in Non-Diabetic Patients With Recurrent, Platinum Sensitive Ovarian Cancer and the Feasibility of Using a Core Biopsy for RNA- Seq Open label, efficacy trialOvarianPatients receive metformin BID on days 1- 21, paclitaxel IV over 3 hours on day 1, and carboplatin IV over 30 minutes on day 1. UNC Lineberger Comprehensive Cancer Center & Gynecologic Oncology Associates A Phase II, Open-Label, Non- Randomized, Pilot Study of Paclitaxel, Carboplatin and Oral Metformin for Patients Newly Diagnosed with Stage II-IV Epithelial Ovarian, Fallopian Tube or Primary Peritoneal Carcinoma Open label, efficacy trialOvarian/ Fallopian tube/ Primary Peritoneal (1) Patients receiving primary surgical debulking followed by standard chemotherapy + metformin (2) Patients treated with neoadjuvant chemotherapy + metformin followed by surgery
 Patients receiving primary surgical debulking followed by standard chemotherapy will initiate metformin prior to primary surgery. (2) Patients treated with neoadjuvant chemotherapy will be initiated on metformin prior to the initiation of chemotherapy. Fox Chase Cancer Center NCT The Use and Safety of Metformin, Carboplatin and Paclitaxel in Non-Diabetic Patients With Recurrent, Platinum Sensitive Ovarian Cancer and the Feasibility of Using a Core Biopsy for RNA- Seq Open label, efficacy trialOvarianPatients receive metformin BID on days 1- 21, paclitaxel IV over 3 hours on day 1, and carboplatin IV over 30 minutes on day 1. UNC Lineberger Comprehensive Cancer Center & Gynecologic Oncology Associates A Phase II, Open-Label, Non- Randomized, Pilot Study of Paclitaxel, Carboplatin and Oral Metformin for Patients Newly Diagnosed with Stage II-IV Epithelial Ovarian, Fallopian Tube or Primary Peritoneal Carcinoma Open label, efficacy trialOvarian/ Fallopian tube/ Primary Peritoneal (1) Patients receiving primary surgical debulking followed by standard chemotherapy + metformin (2) Patients treated with neoadjuvant chemotherapy + metformin followed by surgery.")
77
20,531 genes in endometrioid endometrial cancer samples Gene Expression Linear regression modeling Covariates Age, grade, stage, race BMI status Non-obese: BMI < 30 Obese: BMI ≥ 30

78
9/28/2016 78 Obese (N=185) Non-obese (N=105) Age (mean)60.864.5 Race White83%81% Black9% Other8%10% Stage I and II77%83% III and IV23%17% Grade G130%28% G235%28% G335%44% Demographics
 Non-obese (N=105) Age (mean) Race White83%81% Black9% Other8%10% Stage I and II77%83% III and IV23%17% Grade G130%28% G235%28% G335%44% Demographics")
79
Genomic Differences in Endometrial Tumors Related to BMI 181 genes significantly up- or down-regulated with increasing BMI (q-value<0.01) –Lipoprotein Lipase –Insulin receptor substrate-1 –Insulin-like growth factor binding protein 7 –Insulin-like growth factor binding protein 4 –Progesterone receptor DAVID analysis –Cell cycle –DNA metabolism
 –Lipoprotein Lipase –Insulin receptor substrate-1 –Insulin-like growth factor binding protein 7 –Insulin-like growth factor binding protein 4 –Progesterone receptor DAVID analysis –Cell cycle –DNA metabolism")
80
9/28/2016 80 Obesity and Endometrial Cancer in LKB1/p53 Mice LKB1 fl/fl p53 fl/fl »Deletion of LKB1 and p53 »Invasive cancer develops over 8 weeks »High Fat versus Low Fat Diet »Exposure to metformin or placebo

81
Obesity and Metformin in LKB1/p53 Mice Endometrial tumors are double in size in the obese mice. Metformin has increased efficacy in the obese mice. Genomics and metabolomics are ongoing… 9/28/2016 81

82
Conclusions Ovarian/endometrial tumors arising in the setting of obesity are genomically and metabolically different than their lean counterparts – may have different targets for treatment. The association between obesity, insulin resistance and increased risk and poor outcomes in ovarian/endometrial cancer patients makes metformin an attractive agent for the prevention and treatment of this disease. Multiple clinical trials are in progress. Other pharmacologic interventions – statins, orlistat…..

83
Thank you! Choice CHois/noun: choice; plural noun: choices 1. an act of selecting or making a decision when faced with two or more possibilities."the choice between good and evil"synonyms: option, alternative, possible course of action

Similar presentations










: Department.>")





 Scientific Achievements.>")


 Connects the body.>")







