Download presentation
Presentation is loading. Please wait.

1
Evaluation and Treatment of Galactorrhea

2
Introduction: Galactorrhea, or inappropriate lactation, is very common. Requires estrogen, progesterone, and most importantly prolactin Prolactin is secreted by the lactotroph cells of the anterior pituitary gland Galactorrhea incidence: –20-25% of women experience this problem in their lifetime –Can also occur in males

3
Pituitary Anatomy and Function

4
Pituitary Function

5
Posterior Pituitary –supplied by the inferior hypophyseal artery –vasopressin and oxytocin released into circulation Anterior Pituitary –lacks major arterial blood supply –bathed in a dense network of portal blood containing both hypothalamic hormones and paracrine and autocrine factors released from the pituitary cells themselves

6
Normal Lactation and Prolactin Prolactin normally secreted at a low basal rate, from the anterior pituitary Dopamine is the main constituent of prolactin inhibiting factor Prolactin acts at the breast to promote milk secretion and at the ovaries to regulate the release of LH and FSH Prolactin levels are highest in sleep

7
Differential Diagnosis of Galactorrhea Pregnancy and Postpartum Breast stimulation Pituitary adenomas Bronchogenic carcinoma Renal ca Lymphoma Molar pregnancy Craniopharyngioma Sarcoid TB Hypothyroidism Renal failure Cushing’s dz Acromegaly Meds and Herbs Chest wall irritation Burns Breast surgery Idiopathic (35%)
")
8
Causes: Galactorrhea may be physiologic –preg women may produce milk for up to 2 years after stopping breast feeding –fluctuating hormone levels during puberty or menopause can lead to galactorrhea –nipple stimulation –“witch’s milk” in up to 5% of neonates first month of life

9
Causes, cont. Neoplastic Processes –most tumors of brain and pituitary gland associated with galactorrhea are benign –20% incidence of pit tumors in women with galactorrhea –34% incidence of pit tumors in women with galactorrhea and amenorrhea

10
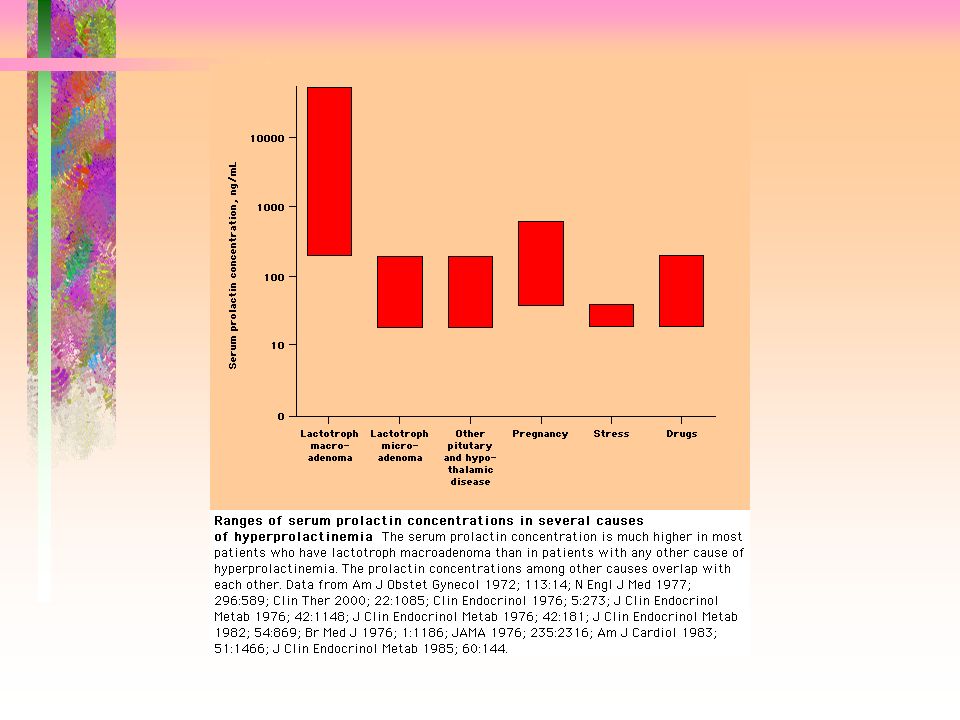
Pituitary hyperprolactinoma Most common tumor resulting in high prolactin benign growth present in 10 - 30 % of the population present with headache, galactorrhea, amenorrhea, defects in peripheral vision, acne, hirsutism, decreased fertility excellent prognosis

11
Hypothalamic-Pituitary Disorders Any disruption of the communication b/w the pituitary and hypothalamus glands can result in increased prolactin secretions and milk production Dopamine affecting conditions: –craniopharyngiomas, infiltrative diseases, pituitary stalk resection, empty-sella syndrome

12
Systemic Diseases Chronic Renal Failure –as a result of decreased clearance by the kidney of prolactin Most common is hypothyroidism –low thyroid hormone results in increased levels of thyrotropin-releasing hormone which increases prolactin secretion

13
Meds Causing Galactorrhea Verapamil H2 antagonists (cimetidine) Estrogens Opiates Dopamine receptor antagonists (Haldol, Risperdal) Reserpine Alpha-methyldopa
 Estrogens Opiates Dopamine receptor antagonists (Haldol, Risperdal) Reserpine Alpha-methyldopa")
14
Meds Antipsychotic meds and Reglan have lactogenic activity b/c of their antidopaminergic effects SSRI’s –Researchers think that serotonin may have a role in regulating prolactin secretion.

15
Meds Amphetamines, cannabis, benzos, opiates all may cause galactorrhea Herbs: –Anise, blessed thistle, fennel, marshmallow, red clover, red raspberry

16
Evaluation Thorough H&P –duration –pregnancy status –acne, hirsutism, menstrual irregularity –headaches –visual field defects –med list including illegal drugs and herbs

17
Evaluation, cont. Physical examination –visual fields, skin, thyroid, breasts Laboratory tests –serum pregnancy test, prolactin level, renal function test, TSH –Prolactin level > 200 is almost always associated with a prolactinoma

20
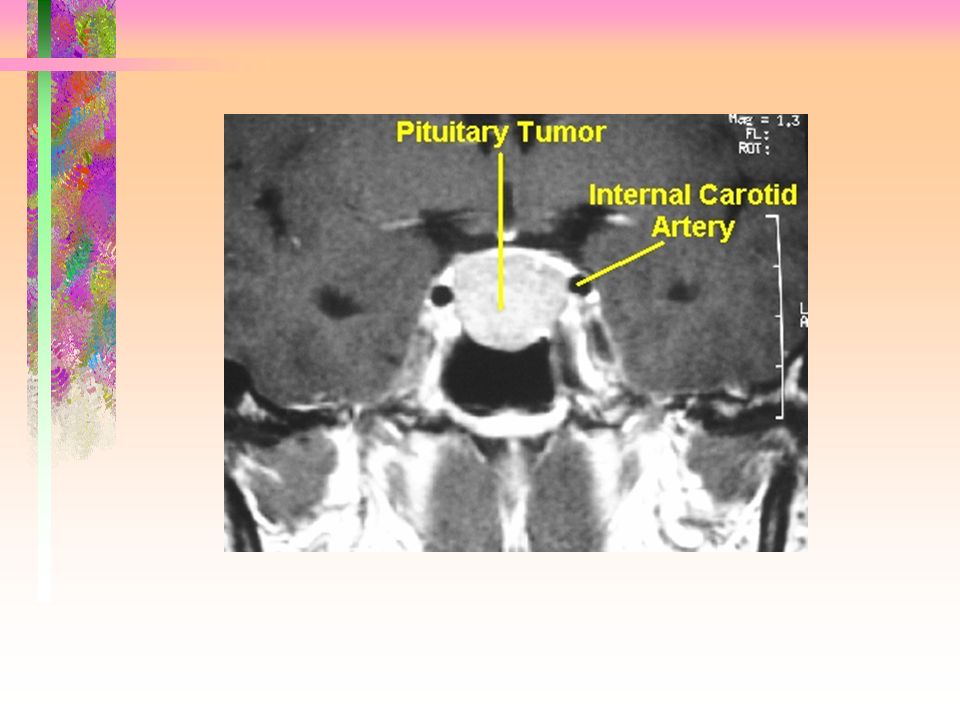
Imaging Studies MRI for prolactin level > 20 Mammography not necessary unless pt has symptoms of breast pathology

25
Treatment Decreasing or eliminating the pt’s symptoms Normal Prolactin level –reasurrance –avoid excessive breast stimulation –d/c med or offending agent

26
Treatment, cont. High Prolactin level –Normal MRI protect against osteoporosis by administering dopamine agonists in the absence of a tumor bromocriptine or cabergoline repeat prolactin levels q 3 to 6 months

27
Treatment, cont. High Prolactin level –Prolactinoma treatment depends on size and symptoms –headache or visual changes indicate need for surgery –microadenomas (less than 1cm) treatment include close observation and/or medical therapy –f/u prolactin levels q 3 to 6 months –bromocriptine or cabergoline
 treatment include close observation and/or medical therapy –f/u prolactin levels q 3 to 6 months –bromocriptine or cabergoline.")
28
Bromocriptine and Cabergoline Activate the lactotroph D2-receptor sites and inhibit the synthesis of prolactin shrink tumors, restore vision, fertility, menses cause nausea, vomiting, headache, and nasal congestion cabergoline has less SE’s and is dosed twice- weekly

29
Bromocriptine and Cabergoline Bromocriptine is the drug of choice in women wishing to conceive D/C once pregnancy is suspected Management is recommended by a specialist in pregnancy

30
Surgery Indicated in patients who cannot tolerate meds, experience rapid visual loss, symptoms not responding to meds Cure rates are poor –50% for microadenomas –25% for macroadenomas

Similar presentations













>")








>")
